Abstract
Introduction: The implications of obesity, especially visceral fat, in health are well known. It would be desirable to control obesity by safe and effective treatment modalities.Aim: To assess the effectiveness of Auricular Acupuncture (AA) on body weight loss in a Portuguese sample.
Methods: After a pre-study, a prospective experimental randomized, controlled and single-blinded study was conducted. The sample included 31 adult women with ages ranging from 20 to 51 years old. The groups had a frequency of physical activity = 2 and = 4 times per week. Individuals with BMI = 24.9 Kg/m2 and pregnant women excluded from the study. All participants were then randomized into one of three groups: group 1 was treated with Vaccaria seeds plus diet therapy, group 2 with ASP needles plus diet therapy and finally, group 3 received only diet therapy. A licensed nutritionist prescribed the hypocaloric diet plan. Baseline evaluation included anthropometric measures collected according to standardized procedures. They received two treatments per week for a total of 6 weeks. After one month of follow-up, all the anthropometric measures were reevaluated. Main parameters: Weight/body composition by bioelectrical impedance analysis. Secondary parameters: Waist to height ratio (WHtR), weight and Body Mass Index (BMI).
Results: Group 2 was significantly associated with lower levels of waist circumference and WHtR (ß= -2,250 95%CI -3,810; -0,691 and ß= -0,014 95%CI -0,023; -0,004, respectively).
Conclusion: We found that the AA with ASP needles has shown the best results on weight and abdominal adiposity loss. The trial has registration number: NCT04834180.
Keywords
Auricular Acupuncture, Hypocaloric diet, Waist circumference, Waist to height ratio, Body Mass Index, Weight, Visceral fat
Introduction
According to the WHO, obesity has more than doubled since 1980 [1]. The reality, however, is that most of the world’s population live in places where overweight and obesity kill more people than underweight. In 2016, more than a third of adults worldwide were classified as overweight or living with obesity, as were 41 million children younger than 5 years [2].
Obesity affects people of all ages, all geographies, and all socioeconomic backgrounds [1]. Several therapeutic options seek to reverse the global epidemic that we are currently facing. Efficient weight control involves a multidisciplinary approach, which can be done through dietary therapy, regular physical activity, behavioral therapy, pharmacotherapy, bariatric surgery (CB) or combinations of different techniques [1,3]. Overweight, obesity and morbid obesity are increasingly prevalent clinical condition throughout the world, with a high mortality rate. It is a multifactorial disease, often associated with other diseases, requiring a therapeutic approach that will reduce weight, an improvement of the associated comorbidities and consequently the improvement of the quality of life of these patients [1,4]. To treat obesity, conventional medicine also uses pharmacological treatment. We have as the most commonly used drug orlistat for the treatment of long-term obesity available on the market [5], since rimonanbant [6] and sibutramine [7] were withdrawn from the market in 2008 and 2010, respectively, as a result of serious cardiovascular and psychiatric adverse effects. However, the association of phentermine + topiramate (Qsymia TM) with lorcaserine (Belvic®) was approved in 2012 [8]. Of all the drugs available on the market, orlistat is the only drug in which its mechanism of action does not involve the Central Nervous System, but in the inhibition of gastrointestinal lipase [9]. Although, conventional treatment (diet therapy, physical exercise, and drug therapy) are usually the first choice, cases of recent onset and no previous adequate treatment history [10]. However, the rate of failure of this type of treatment for morbidly obese individuals is extremely high and there may be a long-term regression in this kind of therapies [11]. AA is a technically simple and virtually painless therapeutic method, often used in several treatments, namely in the treatment of obesity and overweight [12-15]. In fact, the present work focuses on the evaluation of the therapeutic efficacy of AA, as a complementary therapy in the treatment of obesity. For this, an experimental, prospective, controlled, randomized and single blind study was developed, in which it was intended to verify the efficacy in weight loss. This is an issue of particular relevance and interest, as there are few studies that have examined the effects of AA on weight loss, thus offering an additional incentive to perform this work.
Materials and Methods
Participants
This study was approved by the Ethics Committee of Viv Carvalho e Viv Canelas gymnasium and VitaClinic, Portugal. Written informed consents were obtained from all participants before study enrollment. All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards. The present study adheres to the Consolidated Standards of Reporting Trials (CONSORT) statement and Standards for Reporting Interventions in Clinical Trials of Acupuncture (STRICTA). The trial was registered at ClinicalTrials.gov with the Identifier: NCT04834180. The sample in this study included 31 applicants (N=69; 49 women; 20 men; age (mean ± s.d.): 20.8 + 4.71 years; weights: 62.1 + 9.16 kg; heights: 1.69 + 0.07 m; body mass index: 21.73 + 2.25 kg/m2).
Criteria
Inclusion criteria:
• Adults
• Unfamiliar to acupuncture
Exclusion criteria:
• Psychotropic medication
• Psychiatric or thyroid disorders
• Pregnancy
Study design
In a first phase, the following documents were submitted to all those interested in participating in the present study: informed consent, questionnaire on the frequency of physical activity (Figure 1). Before the formation of the experimental groups, and in order to guarantee the greater homogeneity of the groups, the participants were randomized in 3 experimental groups: group 1, received Auriculopressure with vaccaria seeds plus Hypocaloric diet plan; group 2, received auricular acupuncture treatment with Semi-permanent needles (ASP) needles seeds plus Hypocaloric diet plan, and control group 3 (did not receive auriculotherapy treatment, just the Hypocaloric diet plan). Thus, everyone extracted a paper, from an opaque envelope corresponding to the different treatments. Inside of an opaque box were papers defined as 1, 2 and 3, referring to experimental treatment 1, experimental treatment 2 and control treatment, respectively. The random allocation sequence was concealed until interventions were assigned. A staff member enrolled the participants and assigned participants to their groups. The participants and the staff were blinded to the group assignment.
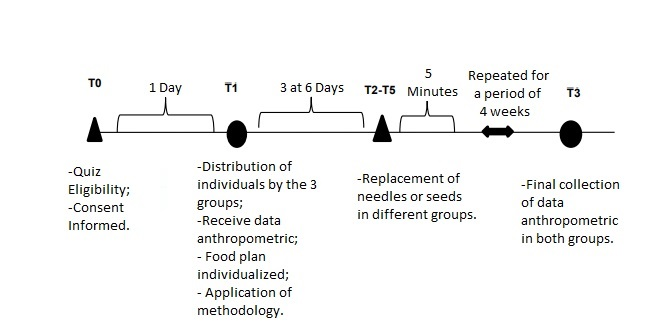
Figure 1. Scheme of the experimental procedure of the study. To: 1 day before the auricular session; T1: Day of the experimental session; T2 to T5: Replacement of needles or seeds in different groups; T3: Final measurement of the anthropometric data in the two groups.
Group and administration
Group 1: At the exterior side of the ear area, standard points were selected according to clinical experience in traditional Chinese medicine: Shenmen (TF4), Stomach (CO4), Hunger, Mouth (CO1), Point Zero HX1) and Sanjiao (CO17). Mustard seeds (Vaccaria ear seeds, Beijing Zhongyan Taihe Medicine, Beijing, China) were used (Figure 2).

Figure 2. Points used in the group Auriculopressure (group 1): 1) Shenmen; 2) Hunger; 3) Mouth; 4) Sanjiao; 5) Point Zero; 6) Stomach.
Group 2: On the outside of the ear standard points were selected according to clinical experience in traditional Chinese medicine: ASP gold needles, strengthening the center with point 0 (the umbilicus) in the dominant ear, Porta Fortunae in the non-dominant ear, Barbiturat in the non-dominant ear, Psychosomatique key point in the dominant ear and the point Aggression (Figure 3).

Figure 3. Points used in the experimental group (group 2): 1) Psychosomatic; 2) Agression; 3) Point Zero; 4) Barbiturate; 5) Porta Fortunae.
Group 3: The hypocaloric diet is defined as reduction of daily calories or foods with high caloric density usually in order to aid weight loss [16].
Outcome measures
All outcomes were collected by the Nutritionist at the baseline and one month later. Data was obtained by crosssectional analysis of Personal data (age, gender, frequency of physical activity, food history) were collected by the application of a survey. The anthropometric data: weight (kg), height (cm) and waist circumference (cm), were measured according to the following procedures:
Primary outcome measure:
• Weight (kg) [Time Frame: 1 month]. A TANITA® bioimpedance scale (model 762) was used to measure the weight and percentage of body fat, as well as visceral fat index. This data was obtained by following the steps in the manual of the scale. Participants were measured using light clothing without shoes. The individual was placed in the middle of the scale, with the feet slightly apart, in order to guarantee a uniform weight distribution [17].
• Waist Perimeter (cm) [Time Frame: 1 month]. A tape measure from SECA® (model 203) was used to measure the waist circumference. The participant was asked to stand, with their feet together, squatting on the floor and relaxed arms hanging freely. As recommended in the literature, the circumference was measured at the end of a normal expiration, in the plane perpendicular to the vertical axis of the body and parallel to the floor, around the abdomen, at the level of the upper border of the iliac crest [17].
Secundary outcome measure:
• Height (cm) [Time Frame: 1 month]. The SECA® stadiometer (model 208) was used to measure stature. Each participant was asked to place their feet slightly apart (about 60º) against the wall, shoulders level and arms positioned along the body. It was certified that the back of the head, shoulder blades, buttocks and heels were touching the vertical surface. The participant was positioned with his head in the Frankfort plane, holding the participant’s chin with his index finger and thumb to keep his head positioned correctly. The top of the stadiometer was placed firmly on the top of the head to compress the individual’s hair [17].
• Body fat (%) [Time Frame: 1 month]. TANITA® bioimpedance scale (model 762)
• Body mass index (kg/m2) is defined as the body mass divided by the square of the body height.
• Waist-to-height ratio (cm2) [Time Frame: 1 month]. The WHTR was obtained by dividing the waist circumference (cm) by height (cm). Participants were later categorized into two groups: Participants at risk (WHTR ≥ 0.5) and non-risk participants (WHTR <18.5, subjects with BMI 18.50 - 24.99 were classified as normal weight, subjects with BMI ≥ 25.
Statistical analysis
The symmetry of the continuous variables was verified by analyzing the asymmetry coefficient (where a value less than 1.5 indicates a symmetric variable) and using histogram and box-plot analysis. The normality of the variables was assessed by the Kolmogorov-Smirnoff test, in which a p value greater than 0.05 indicates a variable with normal distribution. The results of the descriptive analysis of the variables evaluated are presented in the form of mean and respective standard deviation (s.d.) and the ANOVA test was used to compare the mean values between the randomization groups. Simple linear regression and multiple linear regression models were also used to understand the effect of the intervention on the adiposity measures evaluated after one month of followup, adjusting the regression coefficients for the adiposity values at the initial evaluation.
Results
After randomization, 9 women (29.0%) were included in group 1 (“Vaccaria seeds”), 11 (35.5%) were included in group 2 (“ASP needles”) and 11 (35.5%) in group 3 (“control”), making up a total of 31 overweight or obese women (BMI ≥ 25 kg /m2) included in this study, aged between 20 and 51 years. In Table 1, we can find the characteristics of this sample in the initial evaluation, namely the mean values of age, BMI, body fat, waist circumference and ratio between waist circumference and height in each randomization group. During this study 15 people were excluded due to withdrawal.
|
|
Group 1 "Vaccaria Seeds" n= 9 (28,1%) |
Group 2 "ASP' n= 11 (35,5%) |
Group 3 "Control Group" n= 11 (35,5%) |
P* |
|
|
Média (dp) |
|||
|
Age |
32,4 (10,9) |
30,9 (6,8) |
30,3 (12,3) |
0,891 |
|
BMI (Kg/m2) |
27,6 (2,4) |
28,3 (4,6) |
25,8 (1,9) |
0,191 |
|
BF (%) |
36,6 (4,0) |
35,9 (7,5) |
34,9 (4,4) |
0,800 |
|
WC (cm) |
82,9 (8,3) |
84,2 (12,8) |
77,6 (4,6) |
0,233 |
|
RPCA |
0,51 (0,05) |
0,52 (0,09) |
0,47 (0,03) |
0,211 |
Regarding BMI values, group 2 (“ASP needles”) presented a higher average when compared with the other groups (28.3 kg/m2; sd 4.6) in the initial evaluation, while group 3 (“control”) presented the (25.8 kg/m2, sd 1.9), but without statistically significant differences between the three groups (p=0.191). Regarding total body fat levels, group 1 (“Vaccaria seeds”) showed the highest mean value (36.6%; sd 4.0) and group 3 (“control”) showed the lowest values in mean (34.9%; SD 4.4), with no statistical significance (p=0.800). Finally, regarding waist circumference values, group 2 (“ASP needles”) presented the highest mean (84.2 cm; sd 12.8), while group 3 (“control”) presented the highest (77.6 cm; sd 4.6), also without statistical significance (p=0.233). The same trend was observed in relation to the mean values of waist circumference and height, in which the highest values were found in group 2 and the lowest values in group 3 (0.52, sd 0.09 and 0.47, sd 0.03, respectively, p=0.211). After one month of follow-up, we measured the adiposity parameters initially evaluated, whose mean values for each randomization group are presented in table 2.
|
|
Group 1 "Vaccaria Seeds" n= 9 (281%) |
Group 2 "ASP" n= 11 (355%) |
Group 3 "Control Group" n= 11 (355%) |
p* |
|
BMI (Kg/m²) |
27,18 (2,62) |
27,62 (4,57) |
25,38 (1,71) |
0,250 |
|
BF (%) |
35,52 (4,47) |
34,63 (7,54) |
33,98 (4,21) |
0,861 |
|
WC (cm) |
79,68 (7,35) |
80,87(11,00) |
77,23 (4,47) |
0,568 |
|
RPCA |
0,49 (0,04) |
0,50 (0,08) |
0,47 (0,03) |
0,461 |
As expected, the pattern of mean values previously verified in the initial evaluation remained. Group 2 (“ASP needles”) presented the highest mean values for BMI, waist circumference and waist circumference and height ratio (27.62 kg/m2, sd 4.57, 80.87 cm; sd 11.00 and 0.50, sd 0.08, respectively), whereas in group 1 (“Vaccaria seeds”) recorded the highest mean total body fat (35.52%, sd 4.47). In all adiposity parameters, group 3 (“control”) again revealed the lowest values, on average, among the three groups. No statistically significant differences were found between the three randomization groups for any of the adiposity parameters measured in the final assessment. To understand in which of the randomization groups there was a more marked alteration of the adiposity measures, for each of the parameters it was calculated the difference between the values found in the evaluation after one month of follow-up (final evaluation) and the values verified in the initial evaluation (Figures 4-7).
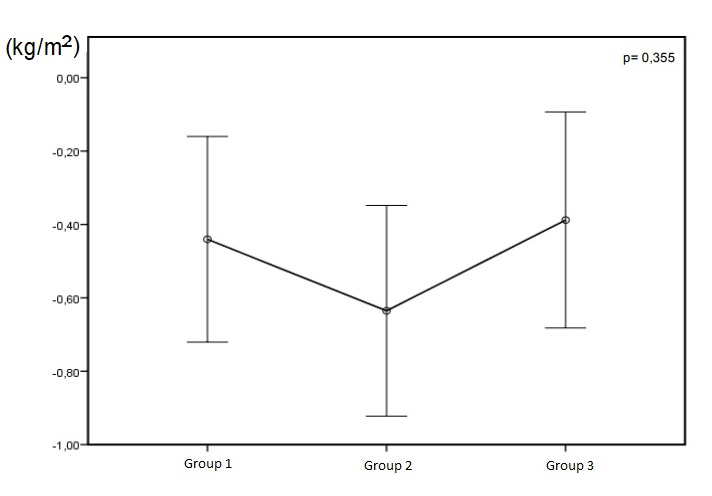
Figure 4. Mean of the difference between the BMI in the final assessment and the BMI at the initial assessment and the respective intervals of confidence at 95%, in each randomization group.

Figure 5. Mean of the difference between the values of total body fat in the final evaluation and in the values verified in the initial evaluation and their Confidence Intervals to 95% in each randomization group.
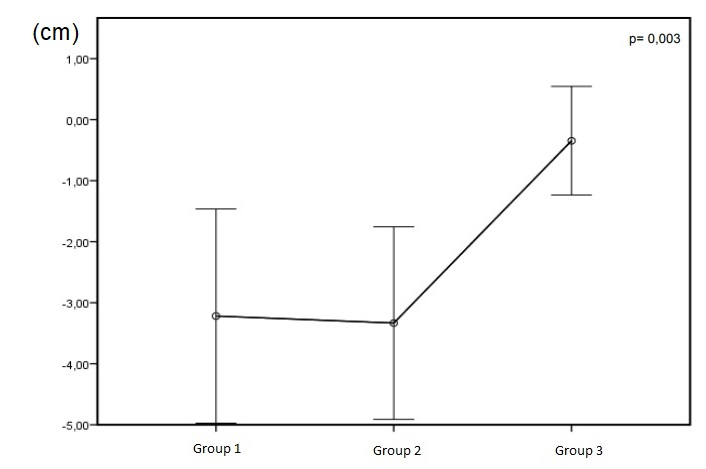
Figure 6. Mean of the difference between the waist circumference values in the final evaluation and the values verified in the initial evaluation and their respectively Intervals of Confidence to 95% in each randomization group.
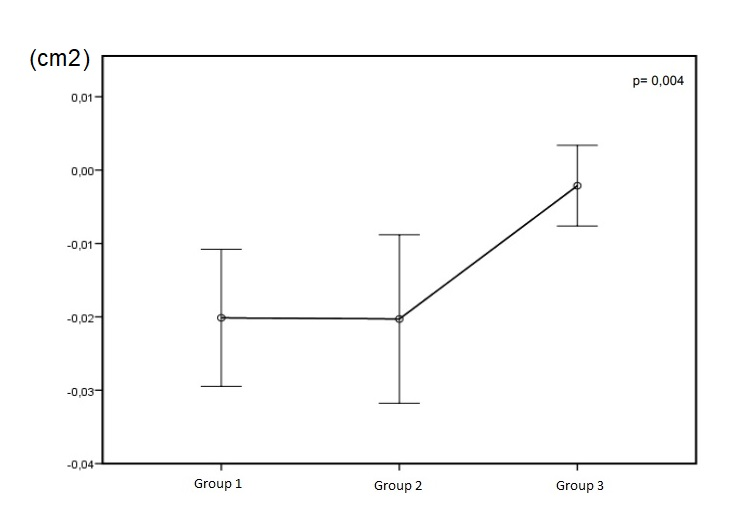
Figure 7. Mean of the difference between the waist/height perimeter ratio values in the final evaluation and the values verified in the initial evaluation and respective Intervals of Confidence to 95% in each randomization group.
Observing the figure, we observed a decrease of BMI in all groups (difference <0), however, this decrease was more marked in group 2 randomization ( “ASP needles”) (0.64 Kg/m2 95% -0.92, -0.35), compared to group 1 (“Vaccaria seeds”) (-0.44 kg/m2, 95% CI -0.72, -0.16) and group 3 ( “Control”), which presented on average a smaller difference (-0.39 kg/m2, 95% CI -0.68;-0.09). Again, between the groups there were no statistically significant differences (overall p value = 0.355).
Analogously to BMI, a decrease in all randomization groups was also observed for total body fat. Group 2 (“ASP needles”) again revealed the most marked difference in body fat between the assessment after one month of follow-up compared to the initial evaluation (-1.27%, 95% CI -2.85, 0.32), whereas in group 3 (“control”) we verified the smallest difference (-0.96%, 95% CI -1.44, -0.48). However, all 3 groups showed statistically similar levels of body fat loss (p=0.891).
Regarding waist circumference, once again the greatest difference was found in group 2 (“ASP needles”) (-3.33 cm, 95% CI -4.91; -1.76), but only slightly higher than in the group 1 (“Vaccaria seeds”) (-3.22 cm, IC95% -4.97; -1.46). The control group (group 3) again presented the smallest difference between waist circumference values in the final evaluation and in the initial evaluation, although also in this group there was loss of abdominal perimeter (-0.34 cm, 95% CI - 1.23, 0.54). Given the discrepancy in the mean values found, the differences between groups 1 and 2, compared to group 3, were statistically significant (p = 0.003).
Although there were statistically significant differences in groups 1 and 2, compared to the control group for the waist circumference and the ratio between waist circumference and height, we tried to understand if the pattern of results remained independent of the initial values of adiposity, that is, if the greater loss of adiposity observed in group 2 (“ASP needles”) is due to the fact that this group has the highest levels of initial adiposity. Through a multiple linear regression analysis, we evaluated the effect of each intervention on the reduction of BMI, total body fat, waist circumference and ratio between waist circumference and height, adjusting the results to the adiposity values in the initial evaluation and using the control group as the reference group (Table 3).
|
BMI |
BF |
WP |
RPCA |
|
|
Group 1 "Vaccaria Seeds" |
-0,050 (-0,450; 0,351) |
-0,098 (-1,345; 1,150) |
-1,958 (-3,466; -0,450) |
-0,012 (-0,021; -0,002) |
|
Group 2 "ASP" |
-0,243 (-0634; 0147) |
-0,266 (-1,589; 1,056) |
-2,250 (-3,810; -0,691) |
-0,014 (-0,023; -0,004) |
|
Group 3 "Control Group" |
Ref (0) |
Ref (0) |
Ref (0) |
Ref (0) |
As expected, taking into account previous waist circumference results, adjusting these values for height (WhTR), group 1 (“Vaccaria seeds”) and group 2 (“ASP needles”) presented the highest loss in the WhTR values [-0.020 (95% CI -0.030; -0.011) and -0.203 (CI 95% -0.032; -0.009), respectively), compared to the control group, where the difference was very close to 0 (-0.002 , 95% CI -0.008; -0.003). Also, as in the case of WC, these differences were statistically significant (p=0.004).
According to the results obtained through the linear regression models, we can verify that even after adjustment for the initial adiposity values, the association remains consistent with the previous results. After one month of intervention, ASP needle treatment was associated with a loss of -0.243 (95% CI -0.634, 0.147) for BMI compared to the control group and a loss of -0.266 (95% CI -1.589, 1.056) of total body fat, although not statistically significant. Regarding the waist circumference, the women who received this intervention had a significant loss of abdominal fat (β = -2,250, 95% CI -3,810, - 0,691), results confirmed by the association observed for the WhTR (β = -0.014, 95% -0.023; -0.004).
Regarding group 1 (“Vaccaria seeds”), results similar to those presented for group 2 were observed, although with associations of smaller magnitude. Other models were also tested, adjusted for variables such as age or sports practice, but without significant changes in the results.
Discussion
In this study, after one month of intervention, the results indicate that both complementary treatments, with Vaccaria seeds and the treatment with APS needles promotes a greater loss of adiposity, when compared to treatment with diet therapy alone. Nevertheless, the intervention group “ASP needles” was what showed a more pronounced loss in all parameters of adiposity evaluated, that indicates a greater effectiveness of this kind of intervention. There was also a significant effect on the loss of abdominal adiposity (waist circumference and waist-to-height ratio) in both intervention groups when compared to the control group, and this effect was also more pronounced in the intervention group in which ASP needles were used, than in the group in which Vaccaria seeds were used. Similar results were demonstrated by other authors. Yeo et al. [18] assessed in a randomized clinical trial with 91 overweight individuals and found a significant decrease in BMI and body fat in the group that received for 8 weeks of AA when compared to the control group. Abdi et al. [19] found similar results in 204 obese participants. Hsu et al. [20] also evaluated the effect of a AA on 60 obese women and, despite not having verified statistically significant differences in adiposity parameters in comparison with the control group, observed that the intervention group had higher levels of leptin and lower ghrelin (appetite-inducing and hormone-inducing hormone, respectively) after a period of six weeks. The same trend was also observed in men [20]. Darbandi et al. [12] studied 80 obese men and demonstrated that both acupuncture and AA had a reduction in body fat. However, other studies did not find any significant effect of acupuncture in the treatment of obesity, demonstrating the existence of contradictory evidence in the literature regarding this theme [19,21,22]. These discrepancies found in the results may be explained in part by differences in the populations tested, both in terms of sociodemographic variables and in terms of anthropometric parameters, differences in study design, or differences in the length of follow-up time of participants. Moreover, given that there is still a consensus and standardization regarding the methodologies and techniques of acupuncture used for the treatment of obesity, it will be difficult to establish direct comparisons between the results presented by different studies.
It has been described that AA may have an effect promoting the release of certain neurotransmitters that act to improve the mood of the individual [23], as well as in the suppression of appetite through the reduction of stress levels and depressive symptomatology, processes mediated via sympathetic and parasympathetic nervous systems [13,23-25]. In fact, the inner part of the ear is enervated by several nerves, including the vagus, glossopharyngeal, trigeminal, facial nerve and the second and third branches of the cervical nerves [13,24,25]. The vagus nerve interacts with the cranial nerve and the nerves of the digestive tract, since they share common pathways to the brain, and it has been suggested that stimulation of the auricular nerves interferes with the appetite signaling pathways [26].
On the other hand, Zhao et al. [27] demonstrated that the use of acupuncture at ‘Zusanli’ (ST-36) and ‘Neiting’ (ST- 44) points led to increased activity in the ventromedial nucleus of the hypothalamus in obese rats, leading to the activation of the satiety and promoting weight loss. In the present study, two different AA methodologies were tested and their effect on adiposity reduction was evaluated. The most common AA points for treatment include the ‘Hunger’ and ‘Stomach’ points (for satiation and satiation, respectively) and ‘Shenmen’ (for sedation and analgesia) [12,21,28,29]. In the intervention group in which Vaccaria seeds were used, the ‘Mouth’, ‘Navel’ (or point 0) and ‘Sanjiao’ points were also tested. These points have already been used in other studies, with significant effects on weight loss and adiposity [12]. In the intervention group in which the ASP needles were applied, the ‘Porta Fortunae’ points were tested in the non-dominant ear, the ‘Navel’ point in the dominant ear, the latter points were chosen because they are related to metabolism (earth phase), ‘Barbiturat’ in the non-dominant ear, which has a regulating function, by its relation with the point 36 of the stomach, the ‘Psychosomatique’ point, a strong point in the mind balance, controlling psychosomatic disorders (and indirectly chronic pain), as it relates to the acupuncture point pericardium 17 and is a coadjutant in the strengthening of Yin, and finally, the ‘Aggression’ point, associated with the liver point 14, with a function of Yang energy regulation of that organ, which controls the emotions of anger and rage [30-32]. Despite the differences in methodology used in comparison to other studies, the results found in the present study are in line with the evidence presented by other laboratory and epidemiological studies demonstrating the efficacy of AA in the loss of total body fat and particularly in the loss of adiposity abdominal. While BMI and total body mass are indicators of generalized adiposity, the waist circumference is strongly correlated with the amount of subcutaneous adipose tissue in the abdominal area. As previously described, several studies have demonstrated that abdominal adiposity is associated with chronic diseases such as type 2 diabetes [33], cardiovascular [34] and metabolic diseases [35] and consequently, reduction of the abdominal perimeter may contribute to a lower risk of development of these diseases, as well as their complications [36]. The additional effect of acupuncture on lipolytic activity and increased lipid metabolism can be seen with a direct effect on redistribution of adipose tissue and lysis of adipocytes, leading, therefore, to a decrease in abdominal adiposity [18,19]. The decrease in waist circumference in the intervention groups of this study was markedly higher than in the control group, which received only diet therapy. Comparing the two interventions (Vaccaria seeds and ASP needles), we found that in both groups there were similar effects on loss of adiposity, and this effect was superior in the intervention group in which the ASP needles were used. Despite this more promising result in reducing adiposity using ASP needles, there are inherent issues in the method that deserve some attention and consideration in individual treatment.
The use of needles may in some cases have adverse effects, namely local pain, inflammation or even infection [37,38]. However, despite the low prevalence of adverse effects, according to the results of our study, the complementary treatment with Vaccaria seeds may present as an effective alternative to ASP needles in susceptible individuals. Because of the small sample size, it is not possible to draw conclusions that allow us the extrapolation of these results to the population from which our sample was drawn. In our conclusions, this study should be replicated in a larger number of individuals, preferably of both sexes, so that it is also possible to test possible interaction effects between intervention effectiveness and gender. However, given the evidence literature, our results appear to be in line with results previously published by several authors. One of the limitations of our study was regarding the follow-up time of the participants. We just performed the follow-up one month, so it was not possible to draw conclusions about the effect of the interventions tested after this period. Since obesity is a chronic disease, for its treatment to be effective the future studies must perform a longer followup. Another limitation of this work that should be noted is the absence of a placebo group in this study design. It is well known that the patient’s expectation regarding the efficacy of acupuncture may influence their results and modify the real effect of the intervention, particularly in small samples [39]. However, some studies have shown that in the placebo group there were not significant results regarding weight and/or fat loss compared to the control group, indicating that the efficacy of these interventions exists regardless of their potential placebo effect [12,18]. As future research prospects, the need for studies evaluating the effect of AA on loss of fat mass with a larger sample size, as well as a longer follow-up period is mandatory.
There is also a need for more evidence to contribute to the understanding of the mechanisms through which AA leads to loss of fat mass, and evidence that clarifies possible reasons for a greater efficacy of acupuncture at the use of needles, comparison with the use of seeds. It has also been suggested that for some types of obesity, the combination of AA and body acupuncture may have an even more significant effect on weight reduction [40]. Given the results published in the literature demonstrating the efficacy of acupuncture in reducing weight and adiposity, it might be relevant to test the combination of these two methodologies.
Conclusions
The conventional approach to the treatment of obesity has proved to be an insufficient response to weight loss and weight control. Thus, there is a need to consider alternative strategies that increase the efficacy of unconventional therapy. According to the results of this study, AA presents as an effective complementary treatment approach in the decrease of adiposity in obese women. After one month of intervention, ASP needle treatment presented the best results in all adiposity parameters, compared to treatment that used diet therapy alone. AA with Vaccaria seeds may be an advantageous alternative to ASP needles in individuals susceptible to adverse effects. In addition, this effect was superior in the reduction of abdominal fat, demonstrating that the application of AA in the obese individual could improve their profile of body fat distribution, consequently reducing the risk of developing diseases such as type 2 diabetes or cardiometabolic diseases. This is the first study that evaluates the efficacy of two different AA methodologies in the treatment of obesity and abdominal fat reduction in the Portuguese population. Since the combination of AA with diet therapy is an effective and relatively simple method, this intervention is suggested as a complementary approach to the reduction of adiposity in overweight or obese women. However, to support these results, there is a need to replicate this study in a larger number of subjects, with a longer follow-up time.
Acknowledgements
We would like to thank all participants. The authors would like to thank Vânia Mendes for assisting with Statistical analysis and also Jürgen Stürmer for assisting with bibliography about the auricular points used.
Conflict of Interest Statement
There are no conflicts of interest as there are no direct financial or other connections with other people or organizations or that can inappropriately influence our work. All research was done by the authors. This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Author Contributions
Diogo Talaia de Matos: Investigation, Methodology, Roles/Writing - original draft, Software, Formal analysis; Andreia Vieira: Conceptualization, Supervision, Writing - review & editing; Maria João Santos: Project administration, Resources; António Moreira: Data curation, Visualization; Jorge Machado: Funding acquisition, Validation.
References
2. Ralston J, Brinsden H, Buse K, Candeias V, Caterson I, Hassell T, et al. Time for a new obesity narrative. The Lancet. 2018 Oct 20;392(10156):1384-6.
3. Clinical Guidelines on the Identification, Evaluation, and Treatment of Overweight and Obesity in Adults: Executive Summary. Expert panel on the identification, evaluation, and treatment of overweight in adults. Am J Clin Nutr. 1998;68(4):899-917.
4. Seidell JC, Halberstadt J. The global burden of obesity and the challenges of prevention. Annals of Nutrition and Metabolism. 2015;66(Suppl. 2):7-12.
5. Stoll M, Bitterlich N, Cornelli U. Randomised, double-blind, clinical investigation to compare orlistat 60 milligram and a customized polyglucosamine, two treatment methods for the management of overweight and obesity. BMC Obesity. 2017 Dec;4(1):1-9.
6. Li MF, Cheung BM. Rise and fall of anti-obesity drugs. World Journal of Diabetes. 2011 Feb 15;2(2):19.
7. Scheen AJ. Sibutramine on cardiovascular outcome. Diabetes Care. 2011 May 1;34(Supplement 2):S114-9.
8. Singh J, Kumar R. Phentermine-topiramate: First combination drug for obesity. International Journal of Applied and Basic Medical Research. 2015 May;5(2):157- 158.
9. Treviño SR. Demographic and Clinical Characteristics, and Adverse Reactions of People With Overweight and Obesity Consumers of Orlistat, Attended by a Call Center (2009 2017). Medwave. 2018 Oct 16;17(6):e7288.
10. Wadden TA, Webb VL, Moran CH, Bailer BA. Lifestyle modification for obesity: new developments in diet, physical activity, and behavior therapy. Circulation. 2012 Mar 6;125(9):1157-70.
11. Delgado-Noguera M, Tort S, Bonfill X, Gich I, Alonso- Coello P. Quality assessment of clinical practice guidelines for the prevention and treatment of childhood overweight and obesity. European Journal of Pediatrics. 2009 Jul;168(7):789-99.
12. Darbandi M, Darbandi S, Owji AA, Mokarram P, Mobarhan MG, Fardaei M, et al. Auricular or body acupuncture: which one is more effective in reducing abdominal fat mass in Iranian men with obesity: a randomized clinical trial. J Diabetes Metab Disord. 2014; 13: 92.
13. Vieira A, Reis AM, Matos LC, Machado J, Moreira A. Does auriculotherapy have therapeutic effectiveness? An overview of systematic reviews. Complementary Therapies in Clinical Practice. 2018 Nov 1;33:61-70.
14. Wang K, Liu Z, Xu B. Impact on the lipid level of obesity of spleen deficiency and damp blockage complicated by hyperlipemia treated with warm needling therapy and auricular acupuncture. Zhongguo zhen jiu= Chinese Acupuncture & Moxibustion. 2016 Mar 1;36(3):225-30.
15. Yu AS, Yang JS, Wei LX, Xie YY. Observation on therapeutic effect of simple obesity treated with acupuncture, auricular point sticking and TDP. Zhongguo zhen jiu= Chinese Acupuncture & Moxibustion. 2005 Nov 1;25(11):828-30.
16. Primo D, Izaola O, Lopez JJ, de Luis DA. Brain derived neurotrophic factor (BDNF) polymorphism rs 10767664 affects metabolic parameters after weight loss secondary to high fat hypocaloric diet with Mediterranean pattern. European Review for Medical and Pharmacological Sciences. 2021 Feb 1;25(4):1944-53.
17. International Society for the Advancement of Kinanthropometry. International standards for anthropometric assessment. Adelaide;. 2001.
18. Yeo S, Kim KS, Lim S. Randomised clinical trial of five ear acupuncture points for the treatment of overweight people. Acupuncture in Medicine. 2014 Apr;32(2):132-8.
19. Abdi H, Zhao B, Darbandi M, Ghayour-Mobarhan M, Tavallaie S, Rahsepar AA, et al. The effects of body acupuncture on obesity: anthropometric parameters, lipid profile, and inflammatory and immunologic markers. The Scientific World Journal. 2012 Jan 1;2012.
20. Hsu CH, Wang CJ, Hwang KC, Lee TY, Chou P, Chang HH. The effect of auricular acupuncture in obese women: a randomized controlled trial. Journal of Women’s Health. 2009 Jun 1;18(6):813-18.
21. Allison DB, Kreibich K, Heshka S, Heymsfield SB. A randomised placebo-controlled clinical trial of an acupressure device for weight loss. International journal of obesity and related metabolic disorders: journal of the International Association for the Study of Obesity. 1995 Sep 1;19(9):653-8.
22. Mazzoni R, Mannucci E, Rizzello SM, Ricca V, Rotella CM. Failure of acupuncture in the treatment of obesity: a pilot study. Eating and Weight Disorders-Studies on Anorexia, Bulimia and Obesity. 1999 Dec 1;4(4):198-202.
23. Lacey JM, Tershakovec AM, Foster GD. Acupuncture for the treatment of obesity: a review of the evidence. International Journal of Obesity. 2003 Apr;27(4):419-27.
24. Gori L, Firenzuoli F. Ear acupuncture in European traditional medicine. Evidence-Based Complementary and Alternative Medicine. 2007 Sep 1;4(S1):13-6.
25. Vieira A, Hinzmann M, Silva K, Santos MJ, Machado J. Clinical effect of auricular acupuncture in anxiety levels of students prior to the exams: A randomized controlled trial. European Journal of Integrative Medicine. 2018 Jun 1;20:188-92.
26. Ito H, Yamada O, Kira Y, Tanaka T, Matsuoka R. The effects of auricular acupuncture on weight reduction and feeding-related cytokines: a pilot study. BMJ Open Gastroenterology. 2015 Dec 31;2(1):e000013.
27. Zhao M, Liu Z, Su J. The time-effect relationship of central action in acupuncture treatment for weight reduction. Journal of Traditional Chinese Medicine= Chung i tsa chih ying wen pan. 2000 Mar 1;20(1):26-9.
28. Huang MH, Yang RC, Hu SH. Preliminary results of triple therapy for obesity. International journal of obesity and related metabolic disorders: journal of the International Association for the Study of Obesity. 1996 Sep 1;20(9):830-6.
29. Abou Ismail LA, Ibrahim AA, Abdel-Latif GA, Abd El- Haleem DA, Helmy G, Labib LM, et al. Effect of acupuncture on body weight reduction and inflammatory mediators in Egyptian obese patients. Open Access Macedonian Journal of Medical Sciences. 2015 Mar 15;3(1):85-90.
30. How C. The comparative study on approach of regulating homeostasis in human body with traditional Chinese medicine. On one of the integration points between Chinese and Western medicine. Zhongguo Zhong xi yi jie he za zhi Zhongguo Zhongxiyi jiehe zazhi= Chinese Journal of Integrated Traditional and Western Medicine. 1998 Apr 1;18(4):198-200.
31. Liu H, Xie Y. Process and key points of clinical literature evaluation of post-marketing traditional Chinese medicine. Zhongguo Zhong yao za zhi= Zhongguo zhongyao zazhi= China Journal of Chinese Materia Medica. 2011 Oct 1;36(20):2848-50.
32. Ye X, Wang J. On English translation of infant Tuina points in traditional Chinese medicine. Journal of Integrative Medicine. 2015 May 15;13(3):205-7.
33. Premanath M, Basavanagowdappa H, Mahesh M, Suresh M. Correlation of abdominal adiposity with components of metabolic syndrome, anthropometric parameters and Insulin resistance, in obese and non obese, diabetics and non diabetics: A cross sectional observational study.(Mysore Visceral Adiposity in Diabetes Study). Indian Journal of Endocrinology and Metabolism. 2014 Sep;18(5):676-82.
34. Elffers TW, de Mutsert R, Lamb HJ, Maan AC, Macfarlane PW, van Dijk KW, et al. Relation of overall and abdominal adiposity with electrocardiogram parameters of subclinical cardiovascular disease in individuals aged 45 to 65 years (from the Netherlands epidemiology of obesity study). The American Journal of Cardiology. 2018 Mar 1;121(5):570-8.
35. Alvero-Cruz JR, MDM GV, JA GL, Linares R. Sensitivity and specificity of abdominal adiposity with metabolic syndrome in the elderly. Revista espanola de geriatria y gerontologia. 2016 Dec 22;52(3):128-34.
36. Menezes A, Artham S, Lavie CJ, Milani RV, O’Keefe J. Erectile dysfunction and cardiovascular disease. Postgraduate Medicine. 2011 May 1;123(3):7-16.
37. Lee M, Lee S, Kim E, Cho YE, Kang JW, Lee JD. Evaluation of bleeding-related adverse events following acupuncture treatment in patients on anticoagulant or antiplatelet drugs: A prospective observational study. Complementary Therapies in Medicine. 2018 Dec 1;41:23- 8.
38. Yamashita H, Tsukayama H, Tanno Y, Nishijo K. Adverse events related to acupuncture. JAMA. 1998 Nov 11;280(18):1563-4.
39. Zhang GS, Zhang CS, Tan HY, Wang Y, DaCosta C, Zhang AL, et al. Systematic review of acupuncture placebo devices with a focus on the credibility of blinding of healthy participants and/or acupuncturists. Acupuncture in Medicine. 2018 Aug;36(4):204-14.
40. Qunli W, Zhicheng L. Acupuncture treatment of simple obesity. Journal of Traditional Chinese Medicine= Chung i tsa chih ying wen pan. 2005 Jun 1;25(2):90-4.