Abstract
Background: Hyperbaric oxygen therapy (HBOT) is used to manage various medical conditions and has been associated with the gradual formation of cataracts after prolonged exposure. However, rapid-onset cataract development remains uncommon. This case describes an unusual presentation of rapid bilateral cataract development following HBOT, occurring over a much shorter timeframe than previously reported in literature.
Case presentation: A 56-year-old woman with hypertension, type 2 diabetes mellitus, and vascular disease experienced a rapid decline in vision following a 40-session, 2-month course of HBOT for a chronic venous leg ulcer. Before HBOT, best-corrected visual acuity had been documented as 20/20 in both eyes. After 2 months of treatment, ophthalmic examination demonstrated bilateral nuclear sclerotic cataracts with a best-corrected visual acuity of 20/40 in both eyes. There was no history of other known cataractogenic exposures. The patient underwent sequential, uncomplicated bilateral phacoemulsification with intraocular lens implantation to achieve mini monovision. Postoperatively, uncorrected visual acuity improved to 20/30 in the right eye and 20/20 in the left eye, with stable refractive outcomes at one month and well-centred lenses on examination.
Conclusions: The temporal association suggests that HBOT may be a potential contributor to accelerated cataractogenesis. Baseline and interval ophthalmic assessments should be considered for patients undergoing HBOT, particularly those with existing risk factors.
Keywords
Hyperbaric oxygen therapy (HBOT), Cataractogenesis, Nuclear sclerotic cataract, Rapid-onset cataract, Bilateral cataracts, Oxidative stress, Reactive oxygen species (ROS), Phacoemulsification, Case report
Introduction
Hyperbaric oxygen therapy (HBOT) is a proven supplementary treatment used to improve tissue oxygenation in a variety of hypoxic and ischemic situations, such as chronic non-healing wounds, radiation-induced injury, decompression sickness, and carbon monoxide poisoning [1]. HBOT greatly increases the quantity of dissolved oxygen in plasma by administering 100% oxygen at high atmospheric pressures. This improves oxygen transport to damaged tissues and stimulates angiogenesis, fibroblast activity, and wound healing [1,2]. Despite being widely regarded as safe, HBOT is linked to a variety of ocular adverse effects, the most prevalent of which are temporary myopic changes and, less frequently, cataract development [3–5].
The crystalline lens is particularly susceptible to oxidative stress due to its avascular nature and reliance on tightly regulated oxygen homeostasis [6]. The lens is kept in a comparatively hypoxic environment during physiological conditions, which shields lens proteins from oxidative damage [6]. Exposure to supraphysiologic oxygen levels during HBOT disrupts this balance, leading to the generation of reactive oxygen species and oxidative modification of lens crystallin’s, ultimately resulting in protein aggregation and loss of transparency characteristic of nuclear sclerotic cataracts [6].
Previous research has demonstrated a link between frequent or prolonged exposure to HBOT and the development of cataracts, which usually happen gradually over long treatment periods [3,5,7]. Rapid bilateral cataract development over a brief period of time is still rare and poorly described in the literature. This case highlights a potentially accelerated form of oxygen-induced cataractogenesis and emphasizes the need for greater clinical awareness and surveillance in at-risk patients by describing an uncommon presentation of early-onset bilateral nuclear cataracts after a typical course of HBOT.
Patient Consent Statement
Written informed consent was obtained from the patient for publication of this case report and any accompanying images.
Case Presentation
A 56-year-old woman presented with rapidly declining vision in both eyes over two weeks. Her medical history included type 2 diabetes mellitus, controlled hypertension, and vascular disease. She had recently completed a 2-month course of HBOT, which included 40-sessions (2.4 ATA, 90 minutes per session, five days per week) for a chronic venous ulcer of the left lower limb.
Before HBOT, she reported good functional vision, documented as best corrected visual acuity of 20/20 in both eyes eight months earlier, requiring only reading glasses. She denied ocular trauma, steroid use, or radiation exposure.
After the 2-month HBOT exposure, best-corrected visual acuity was 20/40 in both eyes. Intraocular pressures measured 20 mmHg bilaterally. Slit-lamp biomicroscope revealed bilateral grade 3 nuclear sclerotic cataracts in both eyes, as shown in Figures 1A and 1B. The anterior chambers were deep and quiet. Fundus examination was unremarkable aside from a peripheral retinopexy scar in the left eye from a remote asymptomatic horseshoe tear. No diabetic retinopathy was observed.
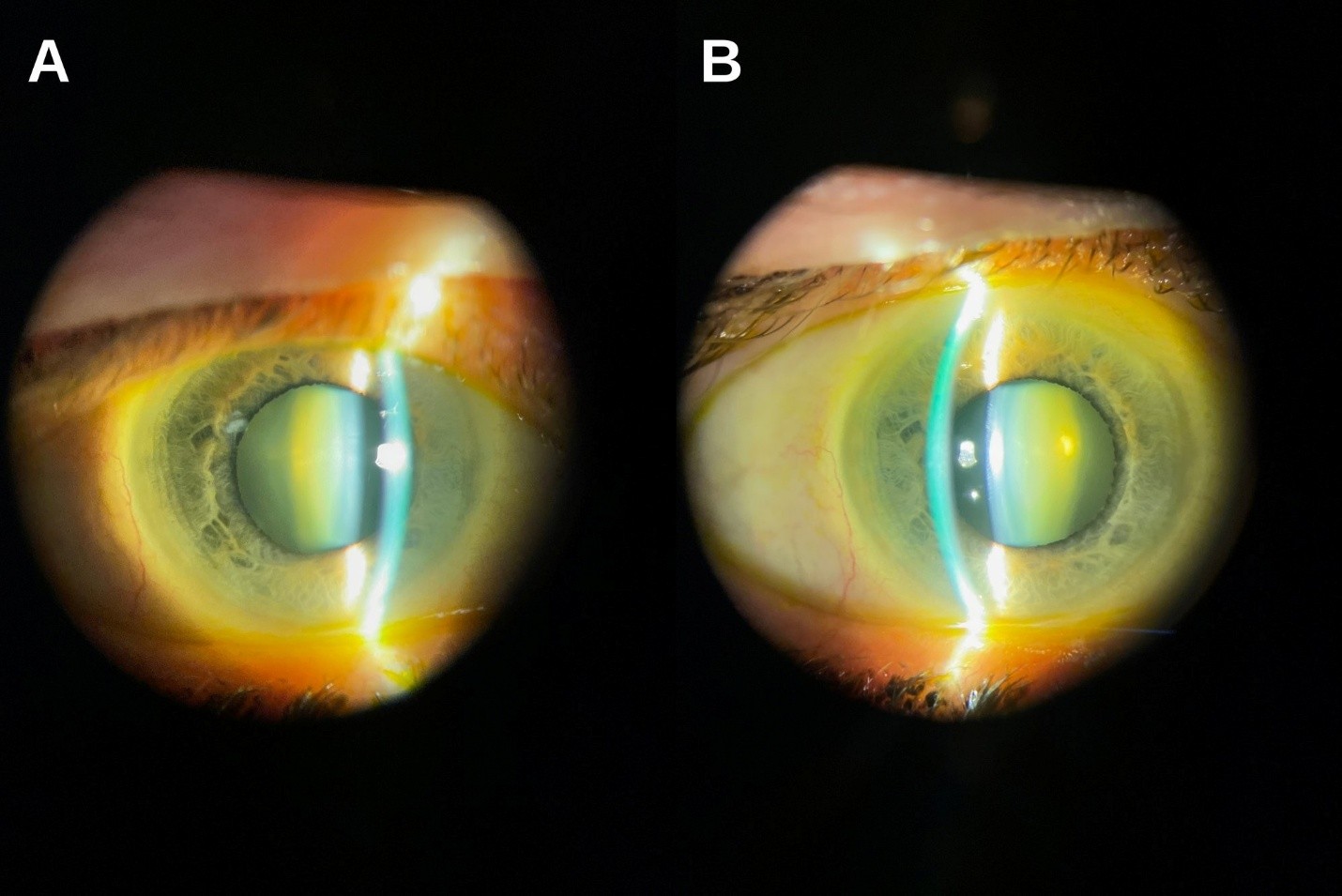
Figure 1. Preoperative slit-lamp photograph demonstrating bilateral moderate nuclear sclerotic cataracts.
Given the rapid progression of visually significant cataracts, sequential bilateral phacoemulsification cataract extractions with implantation of monofocal intraocular lenses (Johnson & Johnson PureSee DET) were performed, targeting mini-monovision (right eye −1.00 D, left eye plano). Both procedures were uncomplicated.
On postoperative day 1, uncorrected visual acuity improved to 20/30 in the right eye and 20/25 in the left eye. At one-week, uncorrected visual acuity was 20/30 in the right eye and 20/20 in the left eye with J3 binocular near acuity. At one month, both eyes demonstrated clear corneas, well-centred intraocular lenses, and stable refraction (-0.75 -0.50 x 95 OD and plano OS).
Given the close temporal relationship between HBOT completion and cataract onset, with no alternative rapid cataractogenic exposures identified, an HBOT-induced mechanism is strongly suggested.
Discussion
Hyperbaric oxygen therapy significantly increases the concentration of dissolved oxygen in plasma, with arterial oxygen tensions exceeding 1,500 mmHg during treatment [1]. This supraphysiologic oxygen delivery enhances diffusion into tissues that are normally relatively hypoxic, including avascular structures such as the crystalline lens [2]. Under physiological conditions, the lens maintains very low oxygen partial pressures, a protective environment that limits oxidative stress and preserves lens transparency [6]. Disruption of this tightly regulated balance during HBOT can lead to increased generation of reactive oxygen species, resulting in oxidative modification and aggregation of lens crystallin’s, which are key events in the development of nuclear sclerotic cataracts [6].
The association between prolonged HBOT exposure and cataract formation has been described previously, most notably in patients undergoing extended treatment courses, where lens changes typically develop gradually over months or years [3,7]. In contrast, the present case is notable for the unusually rapid onset of bilateral nuclear cataracts occurring within weeks of completing HBOT. This accelerated timeline suggests that individual susceptibility factors may play an important role in modulating the lens response to oxidative stress. Systemic conditions such as diabetes mellitus and vascular disease, both present in this patient, may impair antioxidant defences or alter lens metabolism, thereby lowering the threshold for oxygen-induced lens damage and accelerating cataractogenesis [5].
From a clinical standpoint, this case highlights the need for increased awareness of ocular complications associated with HBOT, particularly in patients with underlying systemic risk factors [3–5]. While HBOT remains a valuable and often essential therapeutic modality, consideration should be given to baseline ophthalmic evaluation before treatment initiation, as well as interval assessment in patients reporting visual symptoms during or shortly after therapy [3,4]. Additionally, informed consent discussions should include cataract formation as a potential adverse effect, especially for patients anticipated to undergo prolonged or intensive HBOT regimens. Early recognition of HBOT-associated lens changes may facilitate timely ophthalmic referral and intervention, thereby minimizing visual morbidity.
Value Statement
What was known
Prolonged hyperbaric oxygen therapy (HBOT) has been associated with gradual cataract development in some patients, presumably due to increased oxidative stress on the crystalline lens during repeated exposure to high oxygen levels [3,7]. Prior literature documents lens changes occurring over years following extended HBOT courses, but an abrupt onset has been considered uncommon [3,5].
What this paper adds
This case report highlights an unusually rapid onset of bilateral nuclear cataracts shortly after completing a standard course of HBOT, occurring on a brisk timeline compared with previously published cases. It underscores the need for baseline and interval ophthalmic screening and heightened clinical awareness when managing patients undergoing HBOT, especially those with systemic vascular risk factors such as diabetes and hypertension.
Acknowledgements
The authors have no acknowledgements to declare.
Disclosures
Blinded conflict of interest disclosure
The authors report no conflicts of interest.
Blinded financial support disclosure
The authors received no public or private financial support for this work.
References
2. Bennett MH, Cooper JS. Hyperbaric oxygen therapy and associated cataracts. InStatPearls [Internet] 2024 Jan 9. StatPearls Publishing.
3. Palmquist BM, Philipson B, Barr PO. Nuclear cataract and myopia during hyperbaric oxygen therapy. Br J Ophthalmol. 1984 Feb;68(2):113–7.
4. McMonnies CW. Hyperbaric oxygen therapy and the possibility of ocular complications or contraindications. Clin Exp Optom. 2015 Mar;98(2):122–5.
5. Gengel KC, Hendriksen S, Cooper JS. Hyperbaric related myopia and cataract formation. InStatPearls [Internet] 2023 Jul 4. StatPearls Publishing.
6. Sharma KK, Santhoshkumar P. Lens aging: effects of crystallins. Biochim Biophys Acta. 2009 Oct;1790(10):1095–108.
7. Micun Z, Dobrzyńska W, Sieśkiewicz M, Zawadzka I, Dmuchowska DA, Wojewodzka-Zelezniakowicz M, et al. Hyperbaric Oxygen Therapy in Ophthalmology: A Narrative Review. J Clin Med. 2023 Dec 20;13(1):29.