Abstract
Verruciform xanthoma is an uncommon benign mucocutaneous lesion that has a verruciform (wart-like) appearance. It was first described by Shafer in the year 1971 affecting the oral mucosa. The most common site for verruciform xanthoma is the oral mucosa. Extraoral verruciform xanthoma is extremely uncommon. It has been reported on the anogenital skin such as the vulva, scrotum, penis, and extremities. These lesions typically show presence of foamy histiocytes in the connective papillae. We present a rare case of verruciform xanthoma arising on the tongue in a middle-aged male.
Keywords
Verruciform Xanthoma, Foamy histiocytes, Tongue
Introduction
Verruciform xanthoma is an uncommon benign mucocutaneous lesion that has a verruciform (wart-like) appearance [1]. It was first described by Shafer in the year 1971 affecting the oral mucosa [2]. The most common site for verruciform xanthoma is the oral mucosa of the gingiva and alveolar mucosa. Extraoral verruciform xanthoma is extremely uncommon; it has been reported on the anogenital skin such as the vulva, scrotum, penis, and extremities [3,4]. These lesions can be mistaken for benign, premalignant and malignant conditions. Histopathological examination is the gold standard for the diagnosis of verruciform xanthomas. Morphologically, these lesions are characterized by the presence of Para keratinized epithelium having papillary or verrucous growth with connective tissue papillae extending up to the surface. The papillae characteristically contain of foam cells also called xanthoma cells. In this article, we discuss a case of verruciform xanthoma arising on the tongue in a middle-aged male along with its clinical and pathologic features and treatment modalities.
Case Report
A forty-three-year-old male presented to the outpatient department with a complaint of a growth on the right lateral border of the tongue for 6 months. There was no associated medical or family history. Intra-oral examination revealed a pedunculated well-defined growth measuring 2.0 cm in greatest dimension on the right lateral border of the tongue. The overlying mucosal surface was papillomatous and the adjacent mucosa appeared normal. A provisional diagnosis of Benign Verruco-papillary lesion was made. The patient was planned for curative excision of the lesion considering its likely benign origin. Excisional biopsy was performed by excising the entire pedunculated lesion. Primary closure was done after achieving haemostasis and the healing was uneventful.
The excised specimen was sent for histopathological examination. The specimen received consisted of a single grey white soft tissue piece measuring 1.5×1.0×0.3 cm with a white papillomatous surface. Formalin fixed paraffin embedded sections were evaluated under light microscope. Histopathological sections showed Papillomatous squamous epithelial hyperplasia with acute on chronic inflammation & aggregates of foamy histiocytes in the papillae. The features were consistent with Verruciform Xanthoma (Figures 1A-1C). Immunohistochemical staining for CD68 and CD163 showed strong immunoreactivity in the foam cells (Figures 2A and 2B). All the peripheral and deep margins of the excised specimen were uninvolved. The patient did well postoperatively, and no recurrence was noted two months post -surgery.
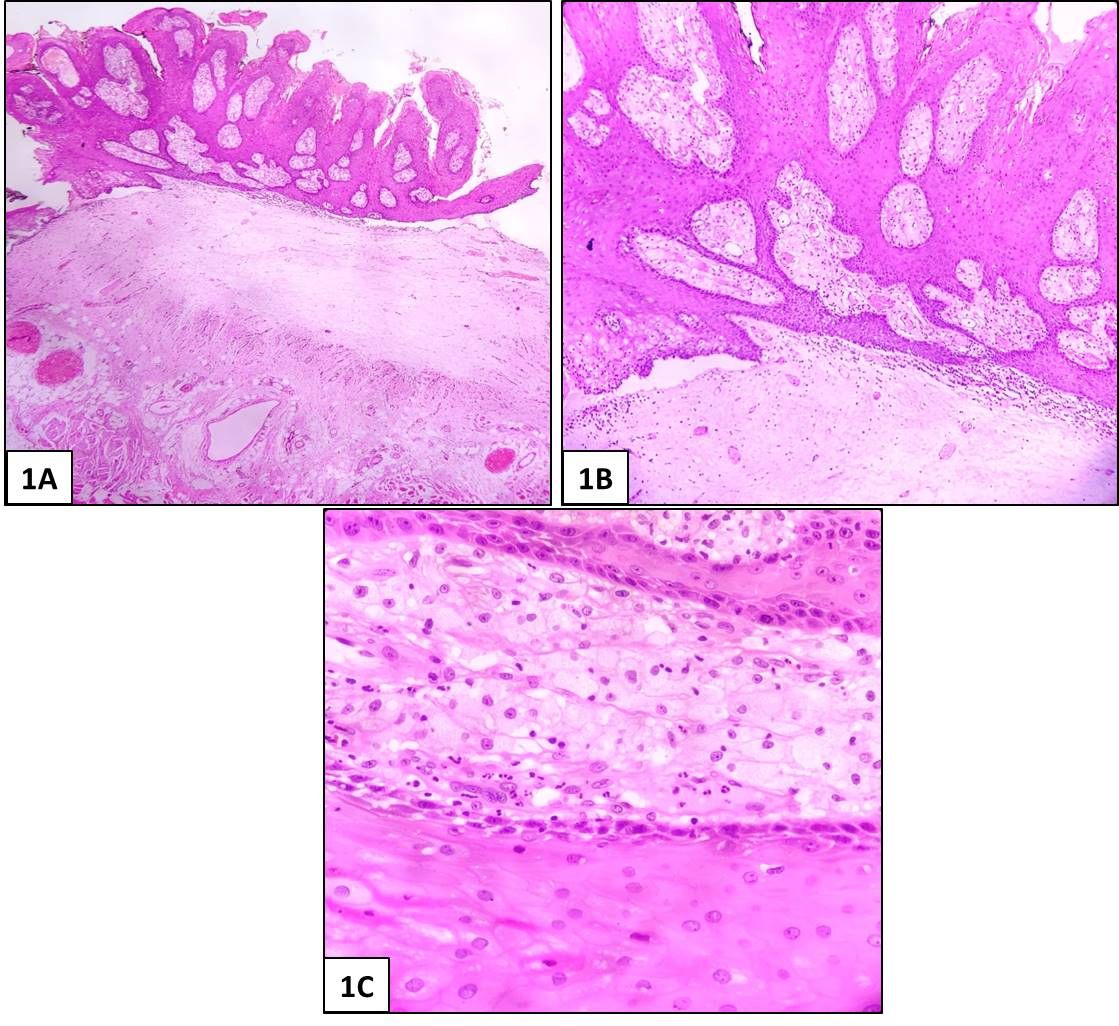
Figure 1. Excisional Biopsy Photomicrographs. A, B) Photomicrograph showing papillomatous lesion with aggregates of foamy histiocytes in the papillae (A- HE-40x; B- HE- 100x). C) Photomicrograph showing foamy histiocytes in papillae (HE-400x).
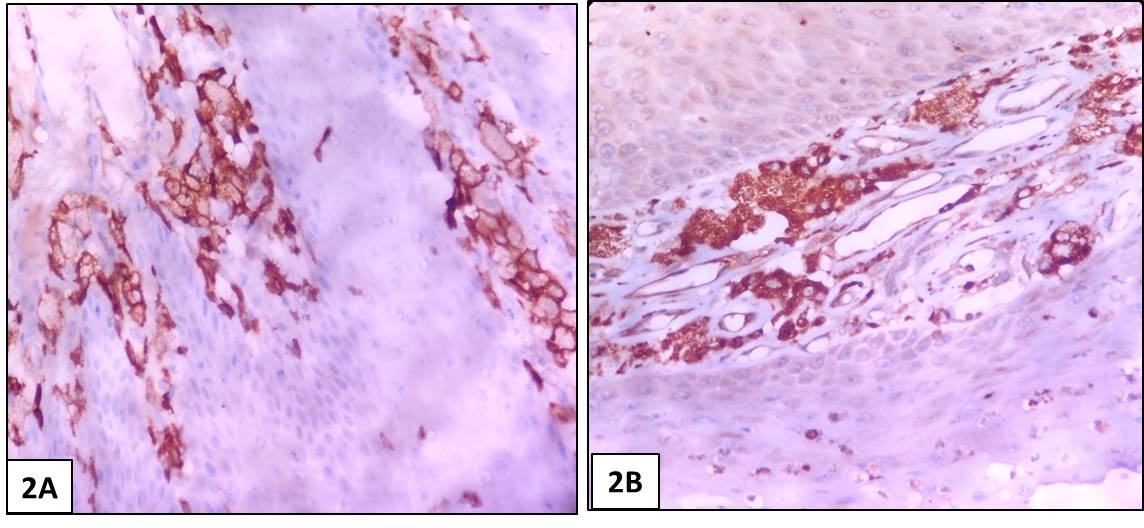
Figure 2. Immunohistochemistry photomicrographs. A) Photomicrograph showing foamy histiocytes immunopositive for CD 163 (IHC- 400x). B) Photomicrograph showing foamy histiocytes immunopositive for CD 68 (IHC- 400x).
Discussion
Verruciform Xanthoma is an uncommon clinicopathologic entity predominantly affecting the mucosa of the oral cavity and genital mucosa. It was first described by Shafer in 1971 where he described 15 cases of this condition in the oral cavity and coined the term ‘Verruciform Xanthoma’. The most frequently involved site in the oral cavity is the masticatory mucosa with the gingival margin being involved most commonly followed by hard palate, tongue, buccal mucosa, floor of the mouth, alveolar mucosa, soft palate and the junction between hard and soft palate. The occurrence of this entity in extra-oral sites is rare and was first reported by Santa Cruz in 1979, when he reported two cases involving the vulva. [1-3]
The pathogenesis of these lesions is unknown. Unlike its cutaneous counterpart, no disturbance of lipid metabolism, or evidence of missense mutation in exon 6 of the 3β-hydroxysteroid dehydrogenase (NSDHL) gene that plays an important role in cholesterol biosynthesis or relation to HPV has been reported. Various hypotheses have been postulated for oral verruciform xanthomas such as local irritation including trauma or inflammation which may cause epithelial degeneration which in turn causes the release of lipids scavenged by macrophages. However, this theory is not tenable for the lesions occurring in the nontrauma prone sites of the oral cavity such as the soft palate or floor of the mouth. Also, the absence of degenerating epithelial cells on histology and the persistence of foamy cells in the connective tissue is not explained. [3-6]
Some authors have stated the probable pathogenesis to be as follows: ‘following keratinocyte damage by a yet unknown inciting agent, cytokines chemotactic for neutrophils are released, producing a rapid growth of the epidermis leading to the verruciform architecture and parakeratosis. The damaged and degenerating keratinocytes that move downwards into the papillary dermis and submucosal region are engulfed by dendritic cells, which develop into foam cells, losing in the process their normal histiocytic markers such as factor XIIIa’ [6].
Verruciform xanthomas are usually asymptomatic, solitary, pedunculated slow growing lesions with a predilection for middle-aged males. [4-6] Similar findings were observed in our case.
The diagnostic finding of verruciform xanthoma is the presence of foam cells in the submucosal stroma. Based on the light microscopic appearance, Nowparast et al. have stratified verruciform xanthomas into three different types:those with a warty or verrucous appearance, a papillary or cauliflower architecture and those with a slightly raised or flat lesion [7-8]. Recently, many studies have been conducted to understand the mechanism of formation of foam cells as well as their migration to the subepithelial region. CD68 is a protein highly expressed by cells in the monocyte lineage, by circulating macrophages, and by tissue macrophages. CD163 is the high affinity scavenger receptor for the haemoglobin-haptoglobin complex and in the absence of haptoglobin - with lower affinity - for haemoglobin alone. It also is a marker of cells from the monocyte/macrophage lineage. Immunohistochemical studies suggest that foam cells originate from macrophages because of their strong immunoreactivity to CD?68 and CD-163 antibodies. In the present case also, the foam cells showed strong immunoreactivity to CD-68 and CD-163.
Mostafa et al., suggested that epithelial hyperplasia with elongation of the epithelial rete ridges is illusory and is not the result of proliferation of epithelial cells with downward growth of the rete ridges but rather the effect of an upward pushing effect of the accumulated macrophages towards the epithelium. This causes the thinning of the epithelium overlying the macrophages in the connective tissue papillae. Nowparast et al., suggested that the verrucous and papillary architecture may be secondary to the presence of foam cells which affect the nutrition and metabolism of the epithelial cells leading to a hyperkeratotic change [8-9].
The treatment of choice is complete surgical excision which is very effective with no recurrence. No conclusive evidence of malignant transformation of pre-existing Verruciform Xanthoma exists in the literature [9].
Conclusion
Verruciform xanthoma is a rare muco?cutaneous lesion which is thought to be a multifactorial chronic reactive process. Irrespective of its extra?oral or intra?oral location, the clinical appearance is non?pathognomonic. It should be considered in the differential diagnosis of other commonly occurring verruco?papillary lesions in the oral cavity. A histopathological examination revealing xanthoma cells/ foam cells is mandatory for the confirmatory diagnosis of Verruciform Xanthomas. Such case reports will highlight the importance of histopathology in diagnosis of Verruciform Xanthomas and rule out malignant verrucopapillary lesions.
References
2. Byakodi S, Kumar B, Patil S, Shinde S. Verruciform xanthoma of the tongue. National Journal of Maxillofacial Surgery. 2017 Jan;8(1):78-80.
3. Hiraishi Y, Tojyo I, Kiga N, Tanimoto K, Fujita S. A case of verruciform xanthoma arising in the tongue. Journal of Clinical and Diagnostic Research: JCDR. 2016 Dec;10(12):ZD07-08.
4. Tamiolakis P, Theofilou VI, Tosios KI, Sklavounou- Andrikopoulou A. Oral verruciform xanthoma: Report of 13 new cases and review of the literature. Medicina Oral, Patologia Oral Y Cirugia Bucal. 2018 Jul;23(4):e429.
5. Shetty A, Nakhaei K, Lakkashetty Y, Mohseni M, Mohebatzadeh I. Oral verruciform xanthoma: a case report and literature review. Case Reports in Dentistry. 2013 Dec 16;2013.
6. Shafer WG. Verruciform xanthoma. Oral Surgery, Oral Medicine, Oral Pathology. 1971 Jun 1;31(6):784-9.
7. Joshi R, Ovhal A. Verruciform xanthoma: report of five cases. Indian journal of Dermatology. 2012 Nov;57(6):479-82.
8. Dorankula SP, Ramani P, Premkumar P. Verruciform xanthoma of the oral cavity–A case report. Journal of clinical and diagnostic research: JCDR. 2013 Aug;7(8):1799-1801.
9. Dave JS, Mahajan SA, Dongre AM, Rane M. Multiple oral verruciform xanthomas: A rare entity. Indian Journal of Dermatopathology and Diagnostic Dermatology. 2020 Jan 1;7(1):27.