Abstract
Background: Screening for type 1 diabetes (T1D) can be challenging, causing diagnostic delay and potentially serious health consequences. Continuing education (CE) in T1D is lagging but could help improve clinician knowledge of and engagement in T1D screening behaviors.
Materials and methods: This retrospective, case-control study assessed pre-/post-changes in clinician knowledge of T1D screening and management (N=4817) following exposure to an interactive, multicomponent CE program (DETECT T1D) from May 2024 to January 2025. Using medical claims, it evaluated pre/post practice change by comparing learners and matched non-learner controls (N=9361) on T1D screening behaviors during the 12 months pre-education vs all available month’s post-education through May 2025.
Results: Post-education, learners demonstrated multiple knowledge and competence gains, including understanding the T1D presentation in adults versus children and identifying appropriate autoantibody screening strategies. Learners achieved a 54% increase in screenings (i.e., 668 more new screenings) following DETECT T1D education vs non-learners (1913 new screenings for learner’s vs 1245 new screenings for non-learners). Primary care, pediatric, and advanced practice provider learners in particular achieved a 116 % gain in screenings vs non-learners (715 new screenings vs 332 new screenings). Learners across all specialties and in all geographic regions demonstrated gains in new screenings vs non-learners.
Conclusion: Interactive, immersive, multicomponent CE may be a feasible and effective pathway to improving clinician detection of T1D. Exposure to this type of learning could have positive downstream effects for patients in terms of more timely diagnosis and earlier intervention, including with disease-modifying therapies that can delay T1D clinical progression.
Keywords
Type 1 diabetes, Continuing education, Type 1 diabetes screening, Type 1 diabetes islet autoantibodies, Presymptomatic type 1 diabetes
Introduction
Type 1 diabetes (T1D) is a chronic autoimmune disease characterized by damage to and destruction of insulin-producing beta cells in the pancreas [1]. T1D is estimated to affect 9.2 million people globally, with rates steadily rising worldwide over the past 2 decades [1]. These rates are even higher when considering the millions of people with presymptomatic T1D, in which a person exhibits antibodies indicative of T1D but may or may not experience glycemic dysregulation [1,2]. Not all individuals with a genetic susceptibility to T1D (i.e., a parent, sibling, or twin with T1D) go on to develop the disease. This demonstrates the complex relationship between genetic risk and necessary cofactors, such as viral infections that stimulate the pathogenic immune response [3]. Indeed, approximately 90% of T1D cases are diagnosed in individuals without a first-degree relative with T1D [4]. This highlights the value of screening all individuals for T1D rather than focusing only on those considered genetically susceptible [5].
Screening for presymptomatic stages of T1D (i.e., stage 1 and stage 2 T1D) can be challenging for numerous reasons [6,7]. Patients are often normoglycemic, so clinicians may not realize screening is warranted. Further, clinicians may not know when and how to screen for presymptomatic T1D (e.g., which tests to use, how to integrate screening into clinic workflows). There are also barriers around the use of islet autoantibodies (IAbs) to screen, including the fact that they are mostly used in research or used clinically inconsistently [6]. Clinicians may also lack knowledge about the existence of IAb panels or be unaware of which tests to order and how to do so.
Other obstacles further contribute to difficulties with screening and can lead to diagnostic delay [8]. For instance, nearly half of new cases of T1D have an adult onset [9]. However, T1D has historically been misperceived as a juvenile-onset disease [9,10]. Diagnosis can be challenging because there is wide variability in the symptoms, presentations, and trajectory of adult-onset T1D, and these differ markedly from juvenile T1D [9,10]. Consequently, T1D can be mistaken for type 2 diabetes (T2D), especially T1D in adults [8,10]. A retrospective analysis of electronic medical records data from 4.7 million patients with at least 1 healthcare encounter for T1D or T2D found a T1D misdiagnosis rate of approximately 10% [9]. However, the authors noted that they used “very conservative” cohort definitions in their study design and suggest 10% likely underestimates the true rate of cases of T1D being misdiagnosed as T2D [9]. Additionally, a retrospective online survey of adults with T1D and parents of children with T1D (N=3030) found nearly one-quarter (24%) of respondents were initially misdiagnosed with another condition, usually T2D (77%) [11]. In that same study, more than 40% of people who developed T1D after age 30 were initially treated for T2D.
Failure to appropriately screen for and accurately diagnose T1D can lead to treatment delay and serious health consequences for patients, including suboptimal glycemic control and an increased risk for acute and long-term complications (e.g., diabetic ketoacidosis, microvascular and macrovascular complications) [10,12]. On the other hand, screening for IAbs, coupled with timely follow-up and appropriate monitoring, can potentially reduce the risk of complications (e.g., diabetic ketoacidosis), helping patients preserve their functioning and quality of life [12]. Additionally, not screening and detecting T1D earlier represents a missed opportunity to potentially enroll patients in other clinical trials that could be of benefit (e.g., clinical trials for patients with stage 1 or stage 2 T1D). With the landmark approval of teplizumab for presymptomatic, stage 2 T1D, screening is also of paramount importance for identifying individuals who could be eligible for disease-modifying therapies [13].
Continuing education (CE) for healthcare professionals is one potential strategy to improve the screening and diagnosis of T1D by increasing clinician knowledge and shaping practice behaviors. This approach could also help address documented knowledge gaps by clinicians in the care of patients with T1D [8]. However, the role of CE in improving clinicians’ T1D knowledge/competence and practice behaviors has been understudied. The current study sought to evaluate the real-world impact of an immersive, interactive CE initiative about T1D (i.e., DETECT T1D) on clinician knowledge and competence about screening and management of T1D. It also sought to evaluate impact of the program on clinician screening behaviors, based on medical claims data.
Materials & Methods
Data were analyzed from 9361 unique learners who participated in DETECT T1D between May 2024 and January 2025, and their matched controls. Learners were categorized in 2 groups: 1) diabetes/endocrine-focused specialists (i.e., endocrinologists and pediatric endocrinologists) or 2) primary care providers (PCPs), pediatricians, and advanced practitioners (e.g., nurse practitioners and physician assistants/associates). The study was exempt from Institutional Review Board approval.
Study design
This retrospective, case-controlled study assessed pre-post changes in clinician knowledge and competence related to T1D screening and management. It also evaluated pre-post clinician practice change using a medical claims analysis. For the claims analysis, learners and matched non-learner controls were compared on T1D screening behaviors during the 12 months pre-education vs screening behaviors during all available month’s post-education through May 2025. Claims assessed included Common Procedural Terminology codes 86341 (islet cell antibodies) and 86337 (insulin antibodies).
Statistical approach
Univariate analyses were employed to compare pre- and post-test results on knowledge/competence among DETECT T1D learners. This consisted of 2 primary metrics. Analysis of covariance was conducted to assess change in screening for T1D between learners and matched controls/non-learners. These results were statistically measured and adjusted to eliminate any pre-education differences between learners and the non-learner control group. Second, a z-test was utilized to observe the net-difference in prescriber penetration, which is the change in number of clinicians screening for T1D pre-education vs post-education.
Assumptions and quality controls included the following: Controls were matched on screening code volume during the pre-education period, clinician specialty, clinician geographic location, medical claims status, overall writing decile, and age. Managed care influences were assumed to be similar between participating test and nonparticipating control clinicians. A clinician must have generated at least 1 prescription for any pharmaceutical product during the most current 12 months to be included in the analysis. This eliminated any clinician who was longer be practicing and writing prescriptions. Given the vast reach of DETECT, with over 20000 clinician learners in its first year, and that the ratio for the matches was low for the top specialties, the learners also had a higher T1D volume than potential controls. Finally, a random sample was used to ensure the matched pairs were representative of the specialty group distribution that were targeted. Some replication for endocrinologists was required.
Outcomes
Outcomes included change in knowledge and competence and change in screening behaviors in the 12-months pre-education vs all available month’s post-education through to May 2025.
Intervention
The DETECT T1D program is a multifaceted, interactive, immersive CE initiative that disseminates information on the screening and early detection of T1D, as well as therapeutic advances to delay disease progression. The development of therapies to delay progression to clinical T1D has the potential to alter paradigms of care, and thus DETECT T1D places an emphasis on screening, early detection, multidisciplinary care, and patient education to help bring these advances to practice. The program is comprised of several features. Clinicians have access to a wide range of education tools and resources through the DETECT T1D website, including high-definition animations, downloadable apps, simulations, poster and pocket card portals, on-demand CE programs, podcasts, and more (Figure 1). DETECT also includes virtual reality experiences offered at association meetings (e.g., American Association of Clinical Endocrinology, Endocrine Society’s Annual Meeting) as well as conference symposia and summits at association meetings (e.g., American Diabetes Association, Pediatric Endocrine Society). Finally, the platform includes recurring interactive learning series, including 20 regional summits, 50 Clinical Conversations, 50 Grand Rounds, and 100 TeleECHO sessions (based on Project ECHO®; Extension for Community Healthcare Outcomes).
Results
Participant characteristics
Two populations were studied for these analyses. For the pre/post-test education gains, scores were analyzed from 4817 clinicians who participated in DETECT T1D between May 2024 and January 2025. The practice change analyses included 9361 participating clinicians and their matched non-learner controls. This number represents the random sample that constituted about half of the exposed leaners. The total sample was comprised of 13% pediatricians, 10% pediatric endocrinologists, 27% endocrinologists, 30% PCPs, and 21% advanced practitioners. Regional distribution of the sample was fairly even, with the largest population being from the West region of the United States (35%). The age of the sample was a normal distribution with few learners under the age of 35 or over the age of 65.
Pre-post education gains
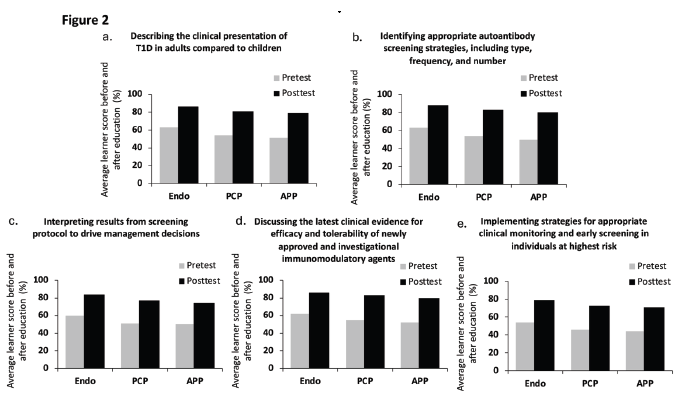
All clinician groups demonstrated gains in education, with the largest being among PCPs and advanced practitioners. These clinicians demonstrated knowledge and competence gains across 5 key topic areas: ability to understand the presentation of T1D in adult’s vs children; ability to identify appropriate autoantibody screening strategies; ability to interpret screening results; ability to discuss newly approved and investigational immunomodulatory treatments; and ability to implement monitoring and screening strategies for high-risk patients (Figure 2).
Pre-post screening behavior change (medical claims analysis)
Learners across all clinician groups achieved a 54% gain in screenings (i.e., 668 more new screenings) following DETECT T1D education vs non-learner controls (1913 new screenings for learner’s vs 1245 new screenings for non-learners). Primary care, pediatric, and advanced practice provider learners in particular achieved a 116% gain in screenings (i.e., 383 more new screenings) vs non-learner controls (715 new screenings vs 332 new screenings).
Pre-post screening behaviors by subgroup
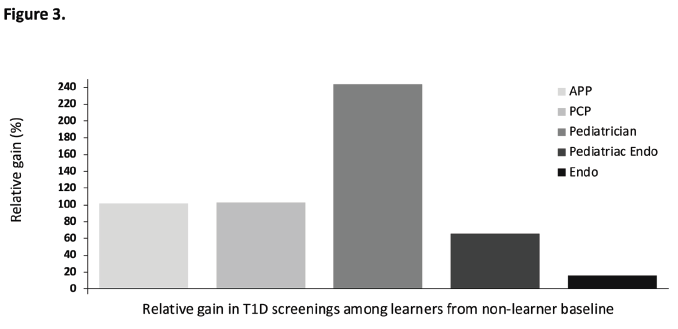
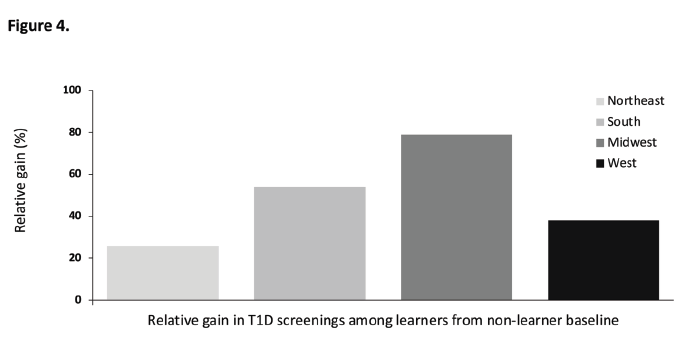
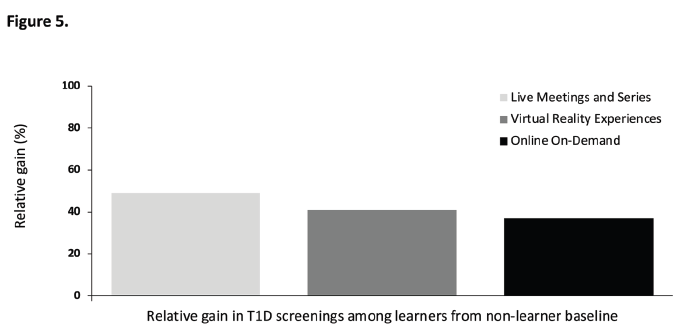
Outcomes across specialties are shown in Figure 3. Learners across all specialties demonstrated gains in new screenings vs non-learners, with the largest gains occurring among pediatricians. Outcomes by geographic region are shown in Figure 4. Learners across all regions demonstrated gains in new screenings vs non-learners, with the largest gains among those in the Midwest. Finally, as shown in Figure 5, outcomes by education format suggest that all 3 learning formats were associated with gains in new screenings vs non-learners and that gains were comparable across all education formats.
Discussion
Exposure to an interactive, immersive, multicomponent CE program (DETECT T1D) was associated with marked improvements in clinician knowledge of and competence in screening for and managing T1D. Participating in DETECT T1D was also associated with desirable changes in clinician behavior. Compared with matched non-learners, learners showed a greater increase in new T1D screenings from 12 months prior to the education through the post-education period, up through May 2025. Learners across all specialties screened more new patients for T1D than non-learners, underscoring the importance of a multidisciplinary educational audience and the need for future education to continue to focus on screening and referral best practices. Across all 4 geographic regions of practice, learners screened more new patients than did non-learners. However, learners in the Midwest achieved the greatest gain in new screenings. This could be attributable to a larger number of learners actively screening in the Midwest than in other regions. This is seen in the higher clinician productivity (i.e., active screenings per clinician) for both the learner and non-learner control group in the pre-education and post-education periods in this region. Finally, there was not a notable change in incremental screening rates across activity formats; thus, continuing a variety of instructional designs in the DETECT curriculum is recommended.
Findings from the current study are consistent with the small number of other published research supporting the role of CE in positively impacting diabetes care. A narrative review from Lan and colleagues highlighted the value of ongoing professional education in aiding healthcare providers in more quickly and accurately recognizing and diagnosing diabetic ketoacidosis in pediatric patients with type 1 diabetes [14]. A second review found interprofessional education on diabetes care that emphasizes multidisciplinary, collaborative teamwork was associated with improvements in provider knowledge, skills, and competence as well as better patient outcomes (e.g., reduced complications such as foot ulcers) [15]. CE in the diabetes field has also demonstrated an impact in treatment decision-making. In a study of more than 1500 U.S. physicians, those engaging with a digital, simulation-based education program were more than 4 times as likely to select an evidence-based treatment for the prevention of cardiovascular events among patients with type 2 diabetes post-education than physicians not exposed to the education (odds ratio 4.49 [95% confidence interval 1.45–13.97]; P=0.001) [16]. Finally, additional evidence suggests the benefits of diabetes-related CE (e.g., improved knowledge and skills) may be heightened when education is offered in web-based and other digital modalities (e.g., scenario-based simulations, gamification) as compared to traditional formats [17]. This lends further support for better understanding the impact and scalability of initiatives such as DETECT in improving real-world clinician and patient outcomes.
This study’s findings align those from other diabetes-related Project ECHO® programs, which demonstrated improvements in PCP knowledge, confidence, and self-efficacy in managing complex diabetes cases and an increase in specialists’ prescribing of newer diabetes medication [18]. These programs are also associated with positive patient outcomes such as decreased inpatient hospitalizations, decreased inpatient spending, and increased uptake of prescription-related quality measures (e.g., increased metformin utilization) [19,20]. However, none of these ECHO® programs were focused specifically on T1D. Walker et al. demonstrated the feasibility and proof of concept of a pilot TeleECHO® program designed to improve PCP knowledge and management of T1D (N=70), particularly in communities with limited access to diabetes specialists [21]. However, to our knowledge, the study investigators have not yet reported on practice change or patient outcomes from the full version of the program.
It is important to note that although the current study’s outcomes are consistent with the small body of research exploring professional CE and diabetes practice outcomes, they diverge somewhat from research on whether CE broadly (not diabetes-specific CE) improves provider practice behaviors. A Cochrane review found educational meetings are more effective than no intervention at all, but the certainty of evidence comparing educational meetings to other educational initiatives was weak [22]. Similarly, a more recent review of continuing professional development demonstrated that although multi-component CE is more effective at improving patient outcomes than standalone programming, little research is available and much of what exists is of low quality [23]. On the other hand, a synthesis of systematic reviews that assessed whether CE impacts physician behaviors found consistent improvements in physician knowledge and inconsistent (but generally positive) results in terms of clinical practice outcomes [24]. Similar to the current study, this review observed that CE that is interactive, dynamic, lengthy, and provided repeatedly appears to have a greater effect on physician performance than static, standalone content [24]. Researchers have cautioned that it can be difficult to determine the extent to which didactic and interactive professional education actually shapes clinician behaviors because of the variability in how CE is defined and conducted across studies [25].
The current study could help address certain barriers to improved T1D detection and management. First, CE programming in diabetes is generally lacking. An analysis of all continuing medical education courses from leading research and primary care medical schools in 2019 found 2.2% of total course hours were devoted to diabetes (i.e., 202 hours out of 9355 total) [26]. This omission is critical because research shows CE can lead to clinician behavior
change of high public health import, such as reduced opioid prescribing [27]. The positive outcomes from DETECT T1D help lend support for financing and scaling up online interactive CE programs in diabetes care.
Second, little empirical data exist on the role of CE in shaping clinician behaviors and patient outcomes in diabetes care, and what programs do exist appear targeted at T2D or diabetes in general. For instance, one small study of medical residents (N=129) found case-based online medication education about diabetes management in inpatients, provided over 2 years, was associated with significant improvement in patients achieving target glycemia values compared with prior to the education [28]. In another analysis, exposure to CE focused on T2D and obesity—which included case-based, interactive, web-based medical education programming—was associated with increased scores of knowledges and competence (e.g., of treatment options, in treatment selection) as well as intended changes in practice behaviors [29]. Notably, neither of these studies were focused on T1D specifically. Further, in the latter study, “intent to change practice behaviors” was self-reported and not tied to objective indicators, such as medical claims data. These gaps underscore the value of the current study in helping to grow the small but important literature on CE-related practice change in T1D care.
CE initiatives like DETECT T1D are also valuable because many PCPs, pediatricians, endocrinologists, and other clinicians struggle with aspects of T1D diagnosis and management [8]. Knowledge gaps appear to exist in several areas, including awareness of presymptomatic T1D and its symptoms, how to make a correct diagnosis and avoid misclassification, how to interpret and follow up on results from T1D screening, and recognizing the role of disease-modifying therapies as an evidence-based treatment option for T1D, especially for early-stage T1D [8]. Current practice patterns suggest providers could benefit from increased training and education-related interventions to close gaps between recommended practices and real-world behaviors. For instance, autoantibody screening is recommended for the early detection of T1D and, if appropriate, referral to treatment with disease-modifying therapy [30]. However, provider awareness of, readiness for, and attitudes toward implementing autoantibody T1D screening in clinical practice are suboptimal [31,32]. Although knowledge is likely just one barrier that accounts for these patterns, it is reasonable to hypothesize that interventions such as interactive, multidisciplinary CE could help mitigate or possibly prevent them.
Initiatives that successfully increase T1D screening rates (such as DETECT) could have important implications for the appropriate use and incorporation of disease-modifying therapies into individualized treatment plans for managing T1D. This is crucial because the current standard treatment approach of lifelong exogenous insulin replacement is suboptimal for many patients (e.g., high cost, the need for constant readjustment of insulin doses) and does not address the autoimmune processes underlying T1D [33]. The advent of disease-modifying medications for this population represents a new opportunity for patients to slow the decline of beta cells and delay disease progression and the onset of symptoms [33].
Finally, outcomes from this study reflect the utility of multidisciplinary CE for improving T1D care as opposed to focusing only on endocrine/diabetes–related specialists. Diabetes is increasingly considered a multidisciplinary condition due to its chronicity, complexity, and multimorbidity [34]. Multidisciplinary team–based interventions for diabetes patients are associated with improved clinical outcomes (e.g., better glycemic control), psychosocial functioning, and healthcare resource utilization (e.g., decreased hospitalizations, reduced mean time from specialty referral to visit) [34]. Relatedly, data from the current study showed an increase in screening among PCPs, which is consistent with current guidance recommending screening for T1D be performed in primary care settings (by PCPs and pediatricians) [35]. CE aimed at the full range of generalists and specialists involved in the screening, diagnosis, and management of patients with or at risk for T1D could help maximize patient outcomes.
The encouraging findings reported here are bolstered by several strengths. This study analyzed data from a large, geographically well-represented sample. Rather than relying on clinician self-report, it used objective metrics (i.e., medical claims data) to characterize practice behavior change associated with CE exposure. This study could also help address a notable gap in the literature (i.e., the lack of studies on T1D-related CE) and well-documented knowledge gaps among clinicians when it comes to screening for and diagnosing T1D.
Study limitations include the fact that learners were likely exposed to other forms of education (e.g., promotions) that the investigators could not control, making it difficult to determine the extent to which changes in knowledge/competence and practice behaviors are attributable to DETECT T1D rather than other factors. The study sample could be considered biased given that it included highly motivated clinicians who voluntarily participated in the education programming. Beyond preexisting knowledge gaps, the data do not clarify the possible barriers that prevented screening from beginning in the first place (e.g., clinician reluctance, difficulty accessing IAb panels). However, the investigators are currently conducting research to better address this question using behavioral analysis techniques. Finally, the data do not capture discussions between clinicians and patients about screening that did not lead to actual screening (e.g., a clinician offering screening but a patient declining).
Conclusions
Interactive, immersive, multicomponent CE may be a feasible and effective strategy for improving the detection of T1D by specialists and by primary care, pediatric, and advanced practice clinicians. This is evidenced by the current study’s findings of demonstrated gains in knowledge and competence pre-post education, as well as a 54% gain in T1D screenings across all clinicians. Exposure to this type of learning could have positive downstream effects for patients in terms of more timely diagnosis and early identification of patients who are eligible for disease-modifying therapy, potentially leading to reduced disease burden and better patient outcomes. However, this would need to be investigated further in future research. T1D is a chronic, complex, highly comorbid disease that affects an increasing number of children and adults across the globe. CE has the potential to directly benefit individual patients and populations as a whole by improving quality of care. T1D-specific CE that has demonstrated effectiveness at impacting clinician knowledge and practice behaviors could lead to better health and well-being for a multitude of individuals.
Conflicts of Interest
Lauren Welch, Nicole Longo, Shpetim Karandrea, and Tom Bregartner are employees of Med Learning Group. Jay Shubrook has received consulting fees from Abbott, Bayer, BI, Eli Lilly, Insulet, Mardigal, Novo Nordisk, and Sanofi; contracted research with Breakthrough T1D; and fees for non-CME services from Corcept.
Funding Statement
Educational programming provided in DETECT T1D was supported by independent medical education grants from Sanofi US.
Acknowledgements
The authors wish to acknowledge Donna Rhoads, MBA, MS, and Nathan Kelleher of IQVIA Digital Inc., for their contribution to the study, providing claims data analysis and editorial support. Editorial support was also provided by Emily A. Kuhl, PhD, and funded by Med Learning Group.
Author Contribution Statement
All authors contributed equally to the development of this manuscript and were responsible for the study conception, design, and manuscript writing.
Availability of Data and Materials
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
References
2. Bonifacio E, Ziegler AG. Type 1 diabetes risk factors, risk prediction and presymptomatic detection: Evidence and guidance for screening. Diabetes Obes Metab. 2025 Aug; 27:28–39.
3. Kotsiri I, Xanthi M, Domazinaki CM, Magiorkinis E. The role of viral infections in the immunopathogenesis of type 1 diabetes mellitus: A narrative review. Biology. 2025 Aug 2;14(8):981.
4. Turtinen M, Härkönen T, Parkkola A, Ilonen J, Knip M, Finnish Pediatric Diabetes Register. Characteristics of familial type 1 diabetes: effects of the relationship to the affected family member on phenotype and genotype at diagnosis. Diabetologia. 2019 Nov;62(11):2025–39.
5. Sims EK, Besser REJ, Dayan C, Geno Rasmussen C, Greenbaum C, Griffin KJ, et al. Screening for Type 1 Diabetes in the General Population: A Status Report and Perspective. Diabetes. 2022 Apr 1;71(4):610–23.
6. Leichter SB, Felton JL, Geno Rasmussen C, Rizzuto P, Bellini N, Ebekozien O, et al. Establishing Screening Programs for Presymptomatic Type 1 Diabetes: Practical Guidance for Diabetes Care Providers. J Clin Endocrinol Metab. 2025 Jul 15;110(8):2371–82.
7. American Diabetes Association. Summary of the American Diabetes Association type 1 diabetes screening & awareness roundtable. 2024. Available from: https://diabetes.org/sites/default/files/2024-04/ADA-T1D-Screening-and-Awareness-Roundtable-Report.pdf
8. Leslie RD, Evans-Molina C, Freund-Brown J, Buzzetti R, Dabelea D, Gillespie KM, et al. Adult-Onset Type 1 Diabetes: Current Understanding and Challenges. Diabetes Care. 2021 Nov;44(11):2449–56.
9. Cheheltani R, King N, Lee S, North B, Kovarik D, Evans-Molina C, et al. Predicting misdiagnosed adult-onset type 1 diabetes using machine learning. Diabetes Res Clin Pract. 2022 Sep;191:110029.
10. Evans‐Molina C, Oram RA. Type 1 diabetes presenting in adults: Trends, diagnostic challenges and unique features. Diabetes Obes Metab. 2025 Aug; 27:57–68.
11. Muñoz C, Floreen A, Garey C, Karlya T, Jelley D, Alonso GT, et al. Misdiagnosis and Diabetic Ketoacidosis at Diagnosis of Type 1 Diabetes: Patient and Caregiver Perspectives. Clin Diabetes. 2019 Jul;37(3):276–81.
12. Simmons KM, Sims EK. Screening and prevention of type 1 diabetes: where are we? J Clin Endocr Metab. 2023 Dec;108(12):3067–79.
13. Evans-Molina C, Oram RA. Teplizumab approval for type 1 diabetes in the USA. Lancet Diabetes Endocr. 2023 Feb 1;11(2):76–7.
14. Lan YY, Kovinthapillai R, Kędzia A, Niechciał E. Enhancing primary care recognition of type 1 diabetes in children: Diagnostic challenges and strategies to prevent diabetic ketoacidosis. J Clin Med. 2026 Jan 9;15(2):533.
15. Sidani S, Patel KD. Interprofessional education in diabetes care—findings from an integrated review. Diabetol. Aug 28;4(3):356–75.
16. Lucero KS, Larkin A, Zakharkin S, Wysham C, Anderson J. The Impact of Web-Based Continuing Medical Education Using Patient Simulation on Real-World Treatment Selection in Type 2 Diabetes: Retrospective Case-Control Analysis. JMIR Med Educ. 2023 Aug 29;9:e48586.
17. Huang Z, Semwal M, Lee SY, Tee M, Ong W, Tan WS, et al. Digital Health Professions Education on Diabetes Management: Systematic Review by the Digital Health Education Collaboration. J Med Internet Res. 2019 Feb 21;21(2):e12997.
18. Ehrhardt N, Bouchonville M, Peek ME, Thomas CC, Zou T, Cuttriss N, et al. Tele mentoring With Project ECHO: A New Era in Diabetes-Related Continuing Education for Primary Care to Address Health Disparities. J Diabetes Sci Technol. 2023 Jul;17(4):916–24.
19. Blecker S, Lemieux E, Paul MM, Berry CA, Bouchonville MF, Arora S, et al. Impact of a Primary Care Provider Tele-Mentoring and Community Health Worker Intervention on Utilization in Medicaid Patients with Diabetes. Endocr Pract. 2020 Oct;26(10):1070–6.
20. Cantor JC, Chakravarty S, Farnham J, Nova J, Ahmad S, Flory JH. Impact of a Provider Tele-mentoring Learning Model on the Care of Medicaid-enrolled Patients With Diabetes. Med Care. 2022 Jul 1;60(7):481–7.
21. Walker AF, Cuttriss N, Haller MJ, Hood KK, Gurka MJ, Filipp SL, et al. Democratizing type 1 diabetes specialty care in the primary care setting to reduce health disparities: project extension for community healthcare outcomes (ECHO) T1D. BMJ Open Diabetes Res Care. 2021 Jul;9(1):e002262.
22. Forsetlund L, Bjørndal A, Rashidian A, Jamtvedt G, O'Brien MA, Wolf F, et al. Continuing education meetings and workshops: effects on professional practice and health care outcomes. Cochrane Database Syst Rev. 2009 Apr 15;2009(2):CD003030.
23. Ali S, Sethi A, Soltani A, Nazar Z. Impact of continuing professional development (CPD) on patient outcomes: a systematic scoping review. BMC Med Educ. 2025 Oct 2;25(1):1284.
24. Cervero RM, Gaines JK. The impact of CME on physician performance and patient health outcomes: an updated synthesis of systematic reviews. J Contin Educ Health Prof. 2015 Spring;35(2):131–8.
25. Ranganathan S, Prasad V. CME: Is it Meeting the Mark? Am J Med. 2023 Jul;136(7):618–19.
26. Berry NA, Fumo NE, Berry BB. Continuing medical education rarely addresses leading public health problems including diabetes and obesity. J Diabetes Clin Res. 2020 Dec 30;2(4):109–13.
27. Kaley A, Brenner JM, Prince AM, Wojcik SM. Effect of a targeted quality improvement education on opioid prescribing. BMJ Open Qual. 2023 Aug;12(3):e001915.
28. Tamler R, Green DE, Skamagas M, Breen TL, Lu K, Looker HC, et al. Durability of the effect of online diabetes training for medical residents on knowledge, confidence, and inpatient glycemia. J Diabetes. 2012 Sep;4(3):281–90.
29. Harris SB, Idzik S, Boasso A, Neunie SQ, Noble AD, Such HE, et al. The Educational Impact of Web-Based, Faculty-Led Continuing Medical Education Programs in Type 2 Diabetes: A Survey Study to Analyze Changes in Knowledge, Competence, and Performance of Health Care Professionals. JMIR Med Educ. 2022 Oct 14;8(4):e40520.
30. Moore DJ, Leibel NI, Polonsky W, Rodriguez H. Recommendations for Screening and Monitoring the Stages of Type 1 Diabetes in the Immune Therapy Era. Int J Gen Med. 2024 Jul 9;17:3003–14.
31. Demeterco-Berggren C, Jacobsen LM, Guttmann-Bauman I, Ospelt EL, Smego A, Hannon TS, et al. 1293–P: Real-world status of autoantibody screening and teplizumab administration readiness among centers participating in the T1D Exchange Quality Improvement Collaborative (T1DX-QI). Diabetes. 2024 Jun 14;73(Supplement_1):1293–P.
32. Ospelt E, Hardison H, Rioles N, Noor N, Weinstock RS, Cossen K, et al. Understanding Providers' Readiness and Attitudes Toward Autoantibody Screening: A Mixed-Methods Study. Clin Diabetes. 2024 Winter;42(1):17–26.
33. Michels AW, Gottlieb PA, Nelson B, Dayan C. Autoimmune Type 1 Diabetes in the Era of Disease-Modifying Immune Therapy. Diabetes Metab Res Rev. 2025 Oct;41(7):e70091.
34. Andersen JD, Jensen MH, Vestergaard P, Jensen V, Hejlesen O, et al. The multidisciplinary team in diagnosing and treatment of patients with diabetes and comorbidities: A scoping review. J Multimorb Comorb. 2023 Mar 20;13:26335565231165966.
35. Phillip M, Achenbach P, Addala A, Albanese-O'Neill A, Battelino T, Bell KJ, et al. Consensus Guidance for Monitoring Individuals With Islet Autoantibody-Positive Pre-Stage 3 Type 1 Diabetes. Diabetes Care. 2024 Aug 1;47(8):1276–98.