Abstract
Hydatid cysts are zoonotic infections caused by the larval stage of Echinococcus granulosus. While the liver and lungs are the primary organs affected by these parasitic cysts, subcutaneous involvement is relatively rare, with an estimated incidence of up to 3%.
In this report, we present the case of a 45-year-old Tunisian man diagnosed with a subcutaneous intermuscular hydatid cyst. The patient underwent monobloc excision of the cyst without intraoperative rupture, and the postoperative course was uneventful.
Solitary hydatid cysts in the subcutaneous tissue are uncommon, and their intermuscular localization, as observed in our case, is exceptionally rare. Diagnosing a primary hydatid cyst in atypical locations presents significant challenges and often necessitates a combination of imaging techniques and serological tests.
The optimal treatment for hydatid cysts remains total excision of the cyst along with its intact wall.
Keywords
Hydatic cyst, Subcutaneous, Intermuscular, Excision
Introduction
Subcutaneous hydatid cyst represents a rare localization of hydatid disease [1]. Clinically, it is usually an asymptomatic, very slowly growing mass, until the size of the cyst is noticed [2]. The symptoms usually occur when the cyst becomes large enough to cause local pressure symptoms, local pain or rarely neurological deficit [2].
The diagnosis is suspected to be based on clinical history, serological testing, and imaging findings and is confirmed intraoperatively [3]. Due to its unusual presentation, diagnosing a subcutaneous hydatid cyst can be challenging. We report the case of a 45-year-old man diagnosed with a subcutaneous intermuscular hydatid cyst.
Case Presentation
A 45-year-old Tunisian man of rural origin, with no medical or surgical history, who presented with back swelling that has been occurring for 6 months. Examination revealed an afebrile patient in good general condition with a large right paramedian dorsal mass measuring 10 cm. This mass was adherent to the deep surface and slightly tender on palpation, with normal skin opposite. Ultrasound showed a well-limited oval mass with anechoic content, posterior enhancement and a clear wall containing at least four vesicles. It measures 5.2 cm x 2.1 cm x 4.4 cm high and it was located 1.25 cm from the epidermal surface.
In order to study the ratios of the mass more closely, an MRI scan was carried out, which revealed a right paramedian intermuscular fluid formation located between the erector spinae muscles on the inside and the trapezius on the outside, with a fusiform shape measuring 96 mm in height and 52 x 30 mm in larger dimensions in the axial plane. This formation has a multiloculated appearance and does not show any significant enhancement after injection of gadolinium. This mass initially suggests a hydatid origin (Figure 1). The hydatid serology was positive, and the TAP CT did not reveal any other sites of disease. The patient had monobloc excision of the cyst with no intraoperative rupture (Figure 2 and Figure 3) and the postoperative course was uncomplicated. Histological examination confirmed the diagnosis of a muscular hydatid cyst. At the 6-month and 1-year follow-up, clinical, biological, and ultrasonographic evaluations revealed no evidence of local or visceral recurrence.
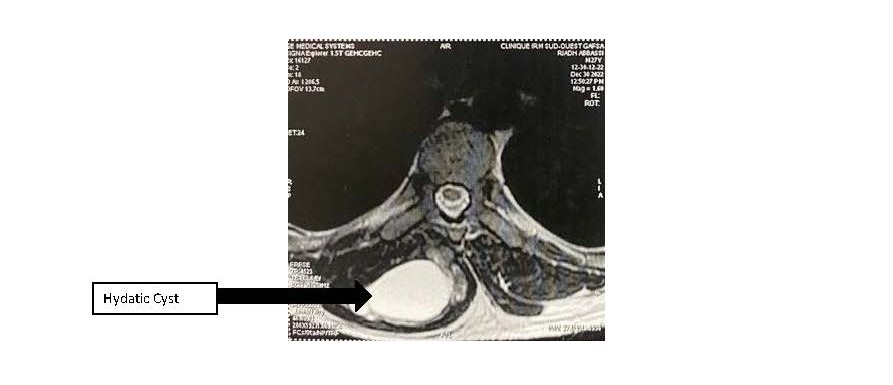
Figure 1. MRI showing multiloculated cyst.
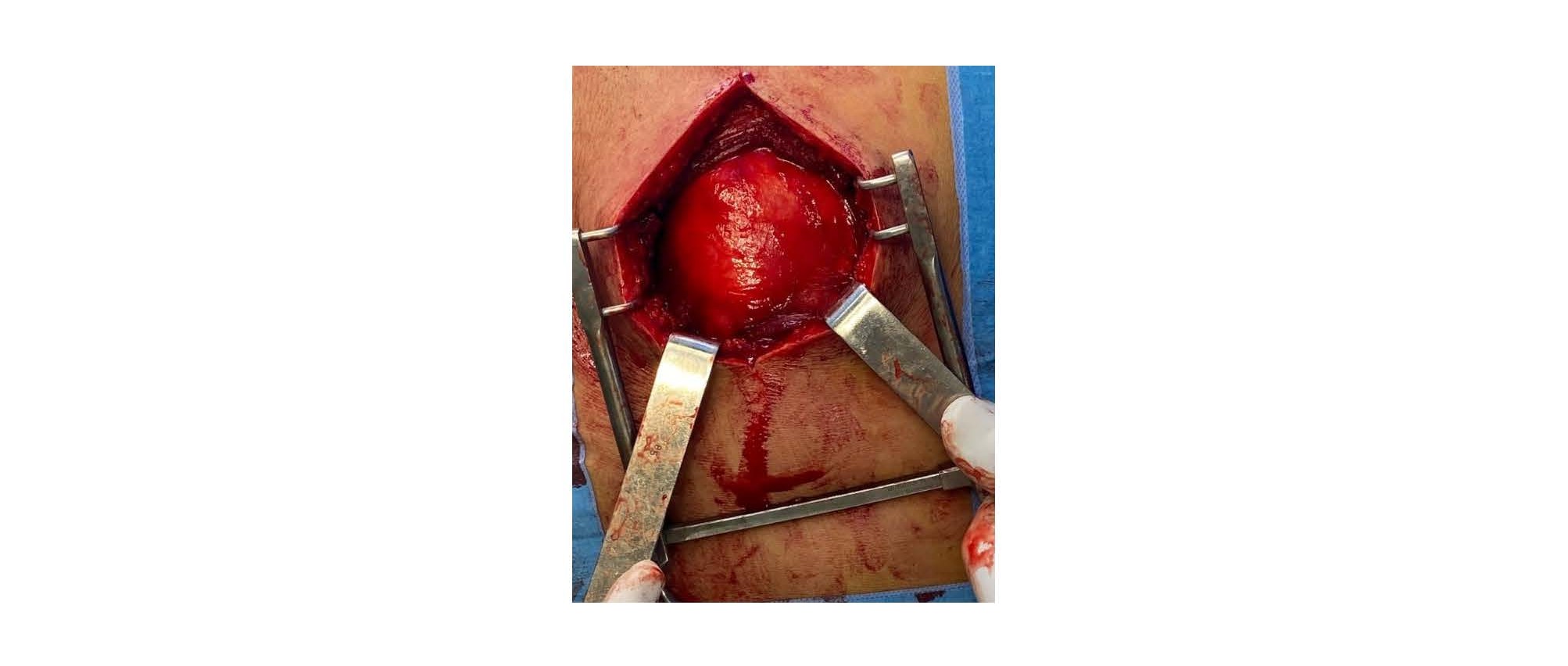
Figure 2. Peroperative view of a hydatid cyst situated between the erector spinae muscles medially and the trapezius muscle laterally.
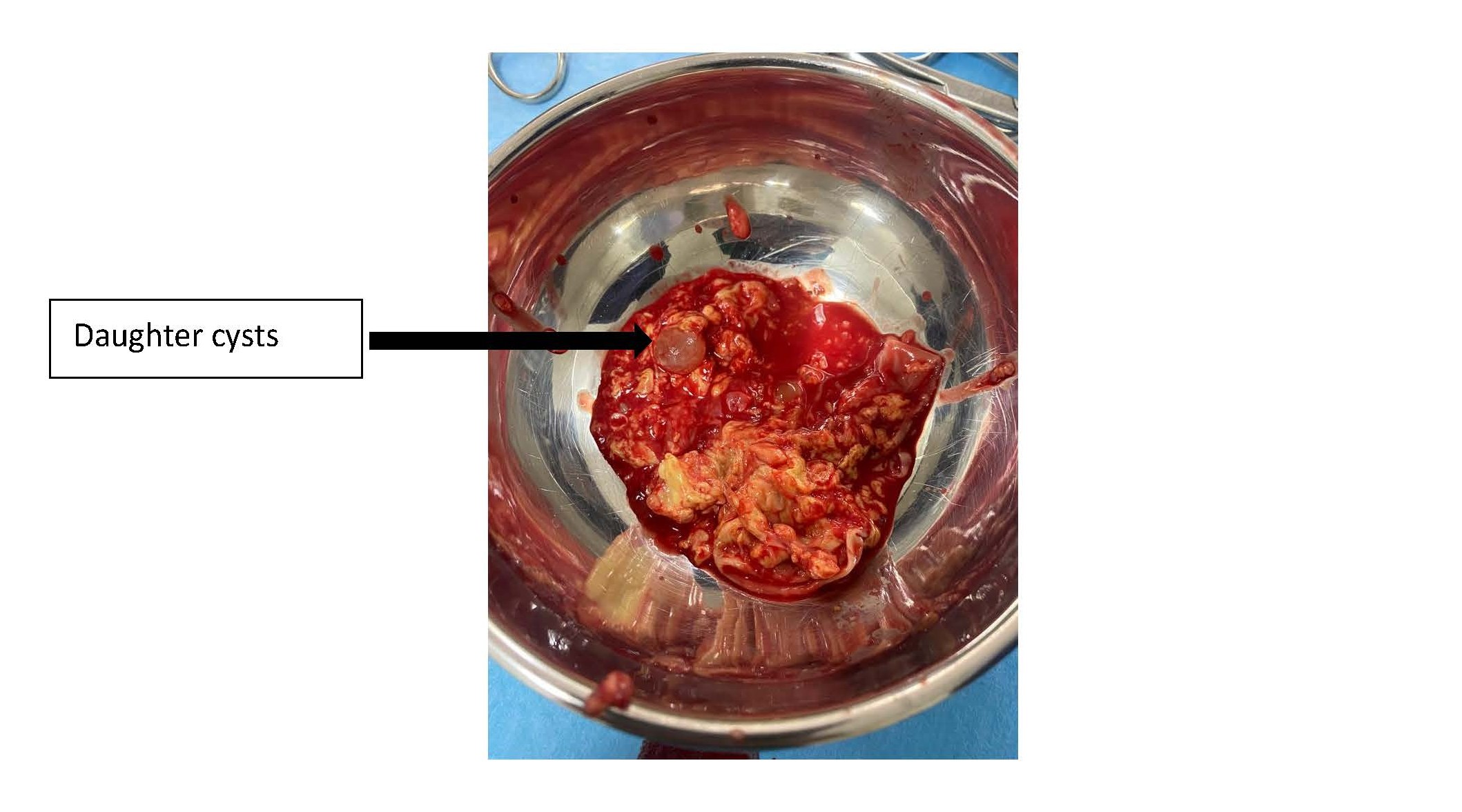
Figure 3. Multivesicular content observed after cyst incision.
Discussion
The mechanism of soft tissue localization is unclear. Eggs of the ingested parasite penetrate the intestinal wall, join the portal system and reach the liver where most of them are taken up in the hepatic sinuses. A few eggs may pass through the liver (first filter) and reach the lung (second filter) and systemic circulation causing hydatid disease in other organs. Possible diffusion through lymphatic channels has also been reported [4].
This mechanism can explain exceptional localizations such as subcutaneous and intramuscular [5]. Primary subcutaneous localization of hydatid cysts is rare, accounting for only 2.3% even in endemic areas [1,6].
In a large Greek series of patients, the incidence of extra-hepatic and extra-pulmonary hydatidosis was 9% [6].
Most reported cases of subcutaneous hydatid cysts are located, in decreasing order of frequency, in the thigh (27%), the hypogastric region, the thorax, and the head and neck region [3]. Dorsal localization is extremely rare which accounts for the peculiarity of our case.
The clinical presentation is nonspecific, typically limited to a painless, non-inflammatory swelling with preservation of the general condition. In cases of fissuration or surinfection, the cyst may mimic a pyogenic abscess or a malignant tumor [7]. Therefore, the possible differential diagnoses can include lipoma, hematoma, cystic lymphangioma and soft tissue tumors [8].
It is important to know that positive serology is significant for the diagnosis [7]. Serological tests allow laboratory confirmation in 80–90% of cases; however, a negative result does not rule out the diagnosis of hydatid cyst [9] and according to the literature, the ELISA test is more sensitive [7]. Therefore, according to literature, it is rarely positive for extrahepatic and extrapulmonary cysts (25%) [5].
Ultrasound is the examination of choice, and MRI is recommended for doubtful forms and for locoregional assessment [4]. Computed tomography (CT) is the imaging modality of choice for patients with pacemakers or indwelling cardiac stents in whom MRI is contraindicated [9]. Moreover, MRI and CT are crucial imaging modalities for the diagnosis of complicated hydatid cysts, including rupture and superinfection [2].
In the present case, ultrasound facilitated the initial diagnosis, revealing features suggestive of either hydatidosis or a benign tumor. The diagnosis of hydatid disease was subsequently confirmed by MRI.
The best therapeutic option is surgical exeresis of the intact cyst to avoid local recurrence and the risk of anaphylactic shock [4]. If exeresis is not possible, the cyst contents can be aspirated intraoperatively or under ultrasound guidance and then irrigated with a scolicidal solution [8]. In our case, we successfully performed the excision of the intact cyst.
Although our patient was successfully treated surgically, the most effective approach to combat hydatid disease remains prevention. Preventing human infection relies on appropriate sanitation and hygiene practices, with particular emphasis on thorough handwashing after contact with dogs, dog feces, or soil contaminated with parasite eggs. In endemic areas, careful washing of raw vegetables and the use of safe drinking water are essential preventive measures [10].
Conclusion
Solitary hydatid cysts in subcutaneous tissue are rare, and their subcutaneous intermuscular location as in our case is exceptional [5]. The clinical symptoms are poor and non-specific [1] and it is difficult to diagnose a primary hydatic cyst in atypical localization without a combination of imaging techniques and serological tests [2]. The best treatment is total excision of the cyst with an intact wall [5] but the best way to combat hydatid disease, wherever it occurs, is prevention [1].
Declarations
Ethics approval and consent to participate
This work does not require ethical considerations or approval. Informed consent to participate in this study was obtained from the patient
Consent for publication
Written informed consent was obtained from the patient for the publication of this case report and the accompanying images. A copy of the written consent is available for review by the Editor-in-Chief of this journal upon request.
Availability of data and materials
Data are available from the corresponding author on reasonable request.
Competing interests
The authors declare that they have no competing interests.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Authors’ contributions
R.D: data collection and manuscript drafting; J.K: validation and supervision; M.N: study conception; M.T: data analysis; K.BS: validation. All authors have read and approved the final manuscript.
Acknowledgements
The authors thank the surgical and nursing teams of Ibn Aljazzar Hospital, Kairouan for their assistance in patient management and the colleagues who provided guidance during manuscript preparation.
References
2. Orhan Ö, Kaptan AY, Percin A, Tekpınar İ, Sepetçi Ö, Cetin VB, et al. Don’t miss it: Extremity-located cyst hydatid may mimic soft tissue tumors. Joint Diseases and Related Surgery. 2023 Sep 20;34(3):687–93.
3. Abdellaou M, Edderai M. Kyste hydatique sous-cutané solitaire de la région fessière: cas clinique. PAMJ Clinical Medicine. 2022 Mar 1;8(35).
4. Lemrhari B, Baha H, Azzouzi S, Chiheb S. Kyste hydatique sous cutané isolé: à propos d’un cas et revue de la literature. Pan African Medical Journal. 2016 Sep 20;24(1).
5. Habboubi K, Kedous MA, Lahmar AA, Miladi M, Annabi H, Mbarek M. Le kyste hydatique des parties molles. Revue du Rhumatisme. 2016 Nov 1;83:A289–90.
6. Prousalidis J, Tzardinoglou K, Sgouradis L, Katsohis C, Aletras H. Uncommon sites of hydatid disease. World journal of surgery. 1998 Jan;22(1):17–22.
7. Mekki RA, Souei MM, Allani M, Bahri M, Arifa N, Gharbi HJ, et al. Kyste hydatique des tissus mous: apport de l’IRM (À propos de trois observations). Journal de radiologie. 2005 Apr 1;86(4):421–5.
8. Ahmed H, Almasoudi E, Hetaimish B, Samargandi R. Primary Hydatid Cyst of the Thigh: Atypical Location and Perioperative Strategies to Minimize Recurrence After Accidental Cyst Rupture. Cureus. 2023 Sep 4;15(8):e42915.
9. Siraj S, Nijrabi MM, Hakimi A, Zaki A, Hares R. Primary intramuscular thigh hydatid cyst: a case report. International Journal of Surgery Case Reports. 2023 Aug 1;109:108589.
10. World Health Organization. Introduction. In: WHO guidelines for the treatment of patients with cystic echinococcosis [Internet]. Geneva: World Health Organization; 2025 [cité 29 déc 2025]. Available from: https://www.ncbi.nlm.nih.gov/books/NBK616291/.