Abstract
End-stage heart failure (ESHF) represents a phase of progressive disease characterized by refractory symptoms, frequent hospitalizations, high mortality, and substantial physical and psychosocial burden for patients and caregivers. Despite advances in guideline-directed medical therapy and device-based interventions, many patients with ESHF experience diminished quality of life and face complex decisions regarding advanced therapies and end-of-life care. Palliative care and hospice services offer a patient-centered approach that prioritizes symptom relief, goals-of-care alignment, and support for patients and families across the disease trajectory, yet remain underutilized in this population. This narrative review examines the evolving role of palliative care in ESHF, with particular attention to its integration in ambulatory and inpatient settings, its intersection with advanced therapies such as continuous inotropes and mechanical circulatory support, and its relationship to hospice care at the end of life. We synthesize current guideline recommendations, clinical trial data, and observational studies demonstrating that palliative care improves symptom burden, quality of life, psychosocial outcomes, and advance care planning, while potentially reducing hospital utilization. Additionally, this review explores the nuanced role of mechanical circulatory support within a palliative framework and highlights the challenges of hospice enrollment for patients with ESHF, including those with left ventricular assist devices. By emphasizing early, longitudinal palliative engagement and clear differentiation between palliative and hospice care, this review underscores opportunities to improve goal-concordant care for patients with ESHF and identifies areas for future research to optimize care delivery, prognostication, and caregiver support.
Keywords
End-stage heart failure, Palliative care, Hospice care, Quality of life, Mechanical circulatory support
Abbreviations
ESHF: End-Stage Heart Failure; PC: Palliative Care; GDMT: Guideline-Directed Medical Therapy; MCS: Mechanical Circulatory Support; HC: Hospice Care; ESC: European Society of Cardiology; NYHA: New York Heart Association; ACC: American College of Cardiology; AHA:American Heart Association; HFSA: Heart Failure Society of America; LVAD: Left Ventricular Assist Device; KCCQ: Kansas City Cardiomyopathy Questionnaire; FACIT-Pal: Functional Assessment of Chronic Illness Therapy–Palliative; PT: Physical Therapy; OT: Occupational Therapy; SNFs: Skilled Nursing Facilities; ICDs: Implantable Cardioverter-Defibrillators; CRTs: Cardiac Resynchronization Devices; DT: Destination Therapy; ECMO: Extracorporeal Membrane Oxygenation
Introduction
The increasing prevalence of heart failure and its management has been a major focus of clinical and research efforts, especially since its designation as an epidemic in 1997 [1]. Currently, approximately 6.7 million adults over the age of 20 in the United States are living with heart failure, with projections estimating an increase to 11.4 million by 2050 [2]. Given that nearly one in four individuals will develop heart failure over their lifetime, there has been growing emphasis on strategies to optimize both prevention and management of the disease, especially as morbidity and mortality rise with disease progression. Prior data demonstrate that as patients transition from at-risk states to established disease, five-year survival declines from nearly 100% to 75%. In refractory heart failure, outcomes are substantially worse, with five-year survival rates approaching 20% [3].
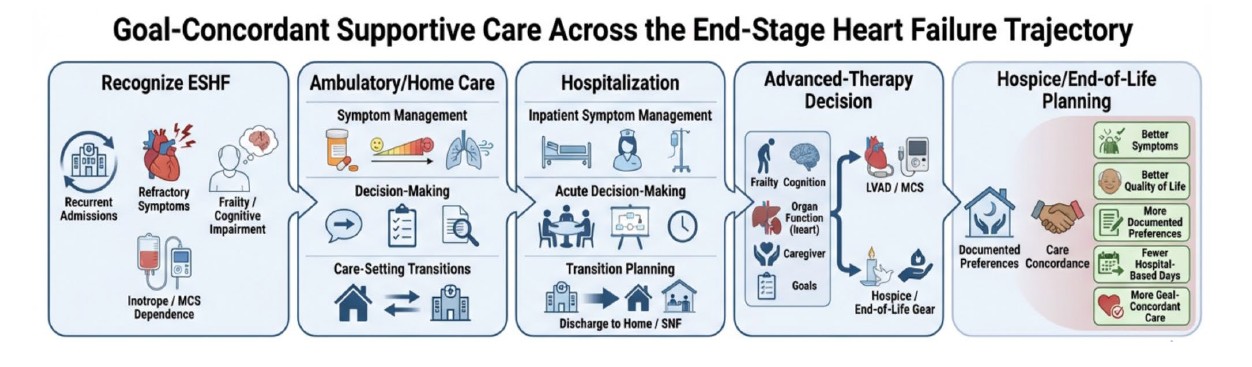
In this context, the significant symptom burden, high mortality, and frequent hospitalizations associated with end-stage heart failure (ESHF) highlight the critical need for a more comprehensive, patient-centered approach. Palliative care (PC), with its focus on symptom management, goals-of-care discussions, and quality of life, is an essential complement to heart failure care in this patient population. Importantly, palliative care is distinct from hospice care. Palliative care is a needs-based approach that can be integrated at any stage of illness alongside disease-directed therapies, whereas hospice care is a prognosis-based model of care intended for patients nearing the end of life, typically with an anticipated life expectancy of six months or less. Although hospice represents one form of palliative care, the broader principles of palliative medicine should ideally be incorporated throughout the trajectory of ESHF treatment.
Current heart failure treatment focuses on using guideline-directed medical therapy (GDMT) to reduce deaths and hospitalizations. However, nearly one in four patients hospitalized for heart failure are readmitted within 30 days of discharge [4]. The model by Chun et al. describes three phases of lifetime readmission risk in heart failure and shows that patients with ESHF account for up to 50% of heart failure–related hospital readmissions [5]. These repeated hospitalizations are not only debilitating for patients, but also place a significant expense burden on the U.S. healthcare system, with estimated annual heart failure-related costs predicted to be $69.8 billion by 2030 [6].
For patients with ESHF, PC offers a compassionate alternative to aggressive interventions, shifting the focus from prolonging life at all costs to enhancing comfort, dignity, and quality of living [7]. PC has been shown to reduce hospital readmissions, time on mechanical ventilation, and improve quality of life in ESHF patients [8,9]. Despite the growing population of those with ESHF and these documented benefits, it is estimated that less than 10% of heart failure patients are utilizing palliative services [10]. This literature review examines the evolving role of palliative care, mechanical circulatory support (MCS), and hospice care (HC) in patients with ESHF, highlighting how these approaches intersect to address symptom burden, extend survival, and optimize quality of life during advanced disease. This review provides a unique contribution to the existing literature by offering a stronger focus on the systemic and clinical barriers to hospice enrollment specific to the ESHF population, alongside exploring practical ambulatory care models, and evaluating the physical and psychological toll that ESHF takes on family caregivers.
To create this narrative review, a comprehensive literature search was conducted across the PubMed, EMBASE, and Cochrane Library databases from database inception through January 2026. Search terms included combinations of keywords related to "end-stage heart failure," "palliative care," "mechanical circulatory support," and "hospice." Inclusion criteria were limited to peer-reviewed, English-language clinical trials, observational studies, and systematic reviews evaluating adult populations. To ensure clinical relevance and alignment with current standards of practice, major societal consensus statements and institutional clinical guideline documents were prioritized during the literature selection process.
What is ESHF?
According to the European Society of Cardiology (ESC), ESHF is defined as the following: severe and persistent symptoms of heart failure at the level of New York Heart Association (NYHA) class III or IV; severe cardiac dysfunction associated with ejection fraction of 30% or less, isolated right ventricular failure, non-operable severe valve abnormalities or congenital heart disease, and/or an ejection fraction of at least 40% with both elevated natriuretic peptide level and significant diastolic dysfunction; hospitalization in the past 12 months that have resulted from congestion requiring intravenous diuretics, low cardiac output requiring inotropes or vasopressors, or management of arrhythmias; and severe impairment of exercise tolerance secondary to cardiac etiology [11]. Clinically, ESHF amongst patients is defined as those with marked symptoms of heart failure at rest despite maximal medical therapy and includes those patients who are recurrently hospitalized or cannot be safely discharged without specialized interventions [12]. These patients are often intolerant of neurohormonal antagonism directed by GDMT due to hypotension and/or renal dysfunction, leading to dependence on advanced interventions such as inotropic agent administration, MCS utilization, and/or referral for cardiac transplantation [12].
What is the Role of Palliative Care in ESHF Patients?
Palliative care plays an integral role in the management of ESHF patients. The American College of Cardiology (ACC), American Heart Association (AHA), and Heart Failure Society of America (HFSA) recommends that palliative care and supportive measures be offered to all patients with ESHF [13]. Supportive measures may encompass left ventricular assist device (LVAD) placement, cardiac transplantation, palliative inotropes, and symptom management strategies. Palliative care consultations in patients with these features can be useful, particularly in those being evaluated for advanced therapies, in those requiring inotropic or temporary MCS, those experiencing uncontrolled symptoms, or those with multimorbidity, frailty, and/or cognitive impairment. Evidence from the PAL-HF trial demonstrated that an interdisciplinary palliative care intervention in advanced heart failure improved quality of life, anxiety, depression, and spiritual well-being compared with usual care alone, as reflected in both disease-specific (KCCQ) and general (FACIT-Pal) quality-of-life measures [11]. Advanced heart failure in this trial was defined as patients with severe symptoms (dyspnea at rest), recent decompensation (admitted or discharged within two weeks of enrollment in the trial), and an ESCAPE risk score of ≥4, which corresponds to a > 50% predicted 6-month mortality rate. This trial specifically found that patients receiving the interdisciplinary palliative care intervention reported significantly better symptom burden and psychosocial outcomes over six months, with higher KCCQ and FACIT-Pal scores alongside lower anxiety and depression scores, underscoring the intervention’s broad benefit across both physical and emotional domains [11]. Taken together, these guideline recommendations and clinical trial findings support palliative care as a fundamental component of comprehensive ESHF management, improving symptom control and quality of life while helping address the complex physical, emotional, and supportive needs of this high-risk population.
The Role of Palliative Care in the Ambulatory and Hospitalized Setting for ESHF Patients
Meticulous medical management is the cornerstone of palliative care in ESHF patients, as it allows for symptom alleviation. Continuing to facilitate discussions regarding patients’ goals of care while implementing palliative and supportive measures should be done by all healthcare professionals and does not necessarily require formal palliative care consultation. However, as overall illness progresses in the ambulatory setting, formal palliative consultation should be considered in the setting of refractory symptoms, major medical decisions, and major forms of impairment, as these roadblocks quickly expand into discussions regarding the initiation of, continued use, or discontinuation of life-sustaining therapies. This has led to the development of longitudinal ambulatory palliative care teams [11]. Home-based integrated heart failure disease management and palliative care have been shown to improve quality of life, reduce hospitalizations, and improve symptomatic burden, as seen repeatedly in the literature [14,15]. Furthermore, advancements in telehealth modalities have led to their implementation in the palliative care setting and their ability to monitor symptoms of ESHF patients, with improvements in pain control and clinical symptoms endorsed [16,17]. Table 1 provides different care models and their outcomes in ESHF.
|
Study |
Care model |
Setting / delivery |
Key components |
Main outcome |
|
PREFER |
Integrated HF + palliative home care |
Home-based |
|
|
|
Wong et al. |
Transitional palliative care |
Weekly home visits/calls, then tapering follow-up |
|
|
|
ENABLE CHF-PC |
Telehealth + nurse coaching |
Remote / telehealth |
|
|
|
2024 JCF consensus paper |
Implementation framework |
Consensus roadmap |
|
|
The hospitalized setting offers a unique opportunity for palliative care integration in patients with ESHF, as it serves as a critical juncture for reassessing treatment trajectories, reassessing goals of care, and initiating advance care planning [18]. Early involvement of palliative care in patients with ESHF helps manage symptoms, guide decisions about starting or stopping therapies that affect quality of life, and address comorbidities and functional status; this is a Class I recommendation in ACC/AHA guidelines. The palliative care team can provide valuable input for patients with refractory cardiovascular symptoms. For example, implementation of opioids for refectory dyspnea and medications for treatment of symptomatic hypotension may provide benefit/relief in mitigating symptomatic hypotension from neurohormonal antagonism and implementation of opioids for refractory dyspnea. This has proven to be effective in the management of symptomatic burden, quality of life, and depressive symptoms, as seen through the findings of the Sidebottom trial [19]. Additionally, prompt integration of the palliative care team into the clinical team of an ESHF patient in the hospital setting has also been shown to result in significant improvement in having future-care preferences documented and advance directives completed [20,21]. The SWAP-HF trial studied the use of a social worker-led palliative care intervention versus usual care, and while depression, anxiety, quality of life, or mortality did not improve, this initiative did result in a significantly higher amount of future-care preferences documented and prognostic alignment [20]. Furthermore, newer data have suggested that implementation of a structured trigger tool to improve appropriate and timely palliative care consultations in hospitalized patients with heart failure may lead to significantly more prompt advance directive planning through more timely completion of healthcare proxy forms, POLST forms, and DNR orders [21]. Table 2 displays studies regarding inpatient interventions for ESHF and their outcomes.
|
Study |
Care model |
Setting / delivery |
Key components |
Main outcome |
|
Sidebottom et al. |
Inpatient palliative-care consultation |
Inpatient consultation |
|
|
|
SWAP-HF |
Social-worker-led intervention bridging inpatient to outpatient care |
Social-worker-led bridge; structured care pathway |
|
|
|
Trigger-tool quality-imp rovement study |
Standardized referral criteria |
Automated trigger for consultation based on criteria |
|
|
Ancillary staff also play a key role in providing palliative care for patients with ESHF during hospitalization. In particular, physical therapy (PT), occupational therapy (OT), and skilled nursing facilities (SNFs) help address deconditioning, frailty, and comorbidities in these patients. Physical therapy is the most well-studied component of multidomain rehabilitation in this patient population. Earlier studies in older adults with physical frailty and poor quality of life showed that early transitional rehabilitation improved physical function across several domains [22]. Furthermore, a secondary analysis of the same data showed that frail patients experienced 2.6-fold greater improvements in physical function than prefrail patients, challenging the assumption that frailty limits responsiveness to rehabilitation [23]. Currently, the American Physical Therapy Association emphasizes the ABCDE framework when working with these patients: assessment, behavior modification, cardiorespiratory fitness, dosage, and education [24]. This framework allows physical therapists to tailor interventions to each individual ESHF patient’s needs, based on vitals, physical exam findings, and observations from the initial evaluation [24]. OT has been less studied in these patients; however, a randomized control trial in 2025 demonstrated that occupational performance coaching as an 8-week intervention significantly improved health self-care behavior, activity participation, and reduced depression in heart failure patients through a focus on enhancing behavior change and promotion of healthy habits and routines [25]. Conversely, SNFs have been widely studied in heart failure patients. Notably, patients discharged to SNFs after heart failure hospitalizations have substantially higher mortality and rehospitalization rates than those discharged home at 30 days and 1 year, likely because these patients have a greater burden of comorbidities and worse baseline physical health [26]. However, home health care utilization following discharge from SNF has been found to significantly reduce the 30-day rehospitalization rate [27]. Of note, only approximately 20% of patients discharged from SNF to home received home health care services, suggesting underutilization [27]. Together, Figure 1 summarizes the role of PT- and OT-based rehabilitation in improving function and self-care among patients with ESHF, while highlighting that discharge to SNF represents a higher-risk transition in which home-health support may help reduce rehospitalization.

Figure 1. Rehabilitation and post-acute support in end-stage heart failure.
Role of Inotropes and MCS Devices in ESHF
Currently, the ACC/AHA/HFSA state as a Class 2b recommendation that continuous intravenous inotropic support may be considered as palliative therapy for symptom control and improvement in functional status in those ESHF patients who are ineligible for MCS or cardiac transplantation. Early trials studying routine inotropic use in ESHF patients demonstrated harm, with increased morbidity and/or mortality demonstrated in pivotal studies [28–30]. Notably, these studies preceded the era of GDMT, implantable cardioverter-defibrillators (ICDs), and cardiac resynchronization devices (CRTs). More contemporary data have shown that when used for palliative intent, continuous milrinone usage in the ambulatory setting following hospital discharge was associated with decreased mortality and longer survival when compared to that of dobutamine [31]. Similarly, an Italian observational study of ESHF patients receiving continuous home inotropic infusion demonstrated a significant reduction in hospitalizations compared with the year prior, improvements in natriuretic peptides and renal and hepatic function, and improved quality of life [32]. However, these findings should be interpreted cautiously, as the available evidence supporting ambulatory inotrope therapy remains largely observational, nonrandomized, and subject to significant selection bias. Patients selected for home inotropic therapy are often highly selected based on the presence of functional status, caregiver support, hemodynamic stability, and access to specialized multidisciplinary care, limiting the generalizability of these outcomes to the broader ESHF population. Additionally, both studies referenced were relatively small and underpowered, underscoring the need for larger prospective controlled studies to better define the risks, benefits, and appropriate patient selection criteria for palliative ambulatory inotrope therapy. Figure 2 summarizes the evolving role of palliative inotropes in ESHF, showing that although routine inotrope use was historically associated with harm, contemporary outpatient use may have a selective role for symptom relief and functional support in carefully chosen palliative patients.
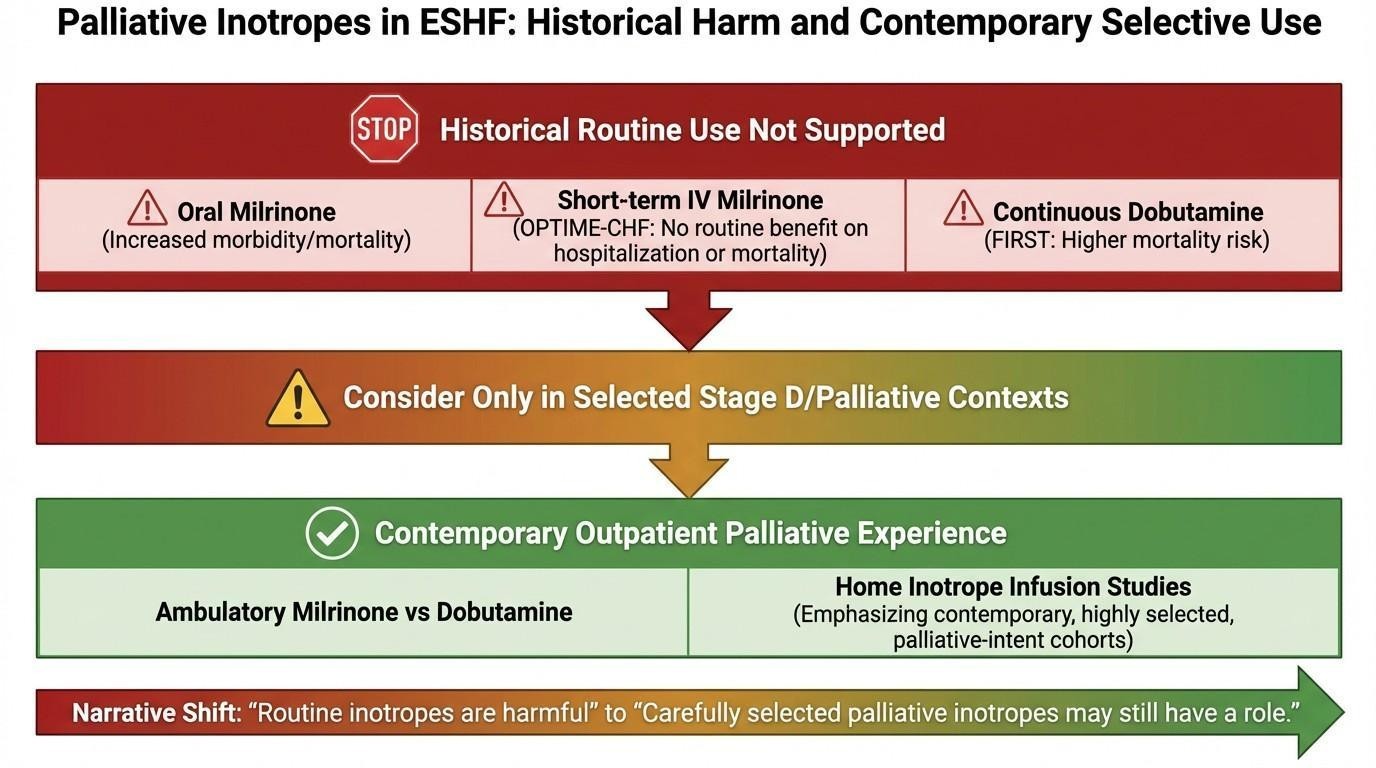
Figure 2. Palliative inotropes in end-stage heart failure: historical harm and contemporary selective use.
MCS occupies a complex role in ESHF, as it is traditionally framed as a life-prolonging intervention but may also be considered, in select patients, within a palliative approach when the primary aim is relief of refractory symptoms and improvement in quality of life. While MCS devices are commonly used to bridge to transplant or recovery, they can also be used for palliative or quality-of-life-focused intent rather than purely restorative goals, particularly in the context of destination therapy (DT) for patients ineligible for heart transplantation [33]. Currently, approximately 81% of LVAD implantations are for destination therapy, reflecting a shift toward using MCS primarily for long-term palliation of symptoms rather than as a bridge to transplant [34]. While patients in this category often have a greater burden of comorbidities, the MOMENTUM 3 trial showed that patients receiving the HeartMate 3 LVAD as destination therapy had survival outcomes comparable to those receiving it as bridge-to-transplant or bridge-to-transplant candidacy, supporting the use of durable MCS in ESHF patients pursuing destination therapy [35,36].
Careful patient selection is essential when considering MCS in a palliative or hospice-adjacent setting, because the potential for symptom relief and functional benefit must be weighed against device-related burdens, clinical risks, and patients’ goals of care. This requires assessment not only of disease severity and prognosis, but also of frailty, end-organ function, caregiver support, cognitive capacity, and willingness to live with a technology-dependent form of care. Additionally, the risks that come with the use of MCS devices must be weighed carefully with each individual patient, including gastrointestinal bleeding, infection, stroke, right ventricular failure, and aortic insufficiency [34]. Temporary MCS devices, such as intra-aortic balloon pump, Impella, or venoarterial Extracorporeal Membrane Oxygenation (ECMO), are generally designed for acute hemodynamic rescue in cardiogenic shock and are therefore most consistent with short-term stabilization or a “bridge-to-decision” strategy rather than a hospice-oriented plan of care [37]. Conversely, durable LVAD therapy may, in selected patients, support palliative goals when it offers meaningful improvement in symptoms, functional capacity, and time outside the hospital [38]. However, this benefit must be balanced against the ongoing burdens of anticoagulation, driveline care, device alarms, caregiver demands, and recurrent complications. Not all forms of MCS are equally compatible with comfort-focused care, and device appropriateness depends not only on the hemodynamic profile but also on whether the practical realities of long-term device management align with the patient’s goals, prognosis, and desired quality of life.
For patients with ESHF who remain on MCS near the end of life, hospice planning must address symptom control, psychosocial support, and the practical and ethical complexities of ongoing device management and possible withdrawal. Enrollment of ESHF patients with an LVAD by hospice agencies is a highly nuanced process due to the lack of incentivization with these patients as there is for low-cost, low-complexity patients [39]. Furthermore, hospice agencies may have limited access to and comfort with cardiac medications for acute or chronic HF symptom management, including diuretics and foundational HF therapies. Limited data exists in this realm of care; however, a retrospective study discussing the qualitative hospice experience with LVAD patients found that that hospices required "just-in-time in-servicing" to prepare teams for challenging care needs including bleeding, delirium, infections, and mechanical failure, demonstrating that hospices must be prepared to manage complex and highly varied needs and must have adequate staff support and access to acute care [40,41].
Ethical considerations surrounding device management and deactivation are also central to palliative care discussions in ESHF patients receiving MCS. Shared decision-making should ideally begin before device implantation and continue longitudinally as patients’ clinical status, functional capacity, and goals of care evolve. These discussions should address the expected benefits and complications of therapy, as well as advanced care planning, acceptable quality of life, and circumstances in which patients would consider device deactivation. ICD deactivation is regarded as the withdrawal of unwanted life-sustaining therapy intended to prevent painful shocks near the end of life. On the other hand, LVAD withdrawal provides additional ethical complexity, as circulatory support cessation may result in rapid death. Despite this, professional societies consider withdrawal of LVAD support ethically permissible when it aligns with patient preferences and goals of care [42]. This highlights the importance of careful interdisciplinary collaboration among providers, patients, and caregivers to ensure decisions made are patient-centered and align with their underlying goals of care.
This is especially necessary as bereaved caregivers have reported feeling uncomfortable with hospice professionals who did not fully understand the LVAD [43]. While MCS remains active, end-of-life care should focus on aggressive symptom management, clear emergency planning, and early discussion of code status to ensure treatment intensity aligns with the patient’s goals. Figure 3 summarizes the role of MCS in ESHF, showing how temporary support and durable LVAD therapy must be weighed against patient-selection factors, device-related burdens, and the need for structured hospice, emergency, and deactivation planning to ensure goal-concordant end-of-life care.
Patients and families should also receive anticipatory guidance regarding likely complications, including bleeding, stroke, infection, device malfunction, and progressive right heart or multiorgan failure. When ongoing support no longer meets the patient’s goals or becomes excessively burdensome, MCS deactivation may be considered through a process that includes informed consent, family preparation, and close coordination among heart failure clinicians, palliative care specialists, hospice teams, and bedside nursing staff [33]. Comfort-focused medications should be prepared before withdrawal and adjusted afterward to relieve dyspnea, pain, anxiety, and distress. Framing these steps within a structured end-of-life plan emphasizes that MCS management in this setting should remain patient-centered, goal-concordant, and grounded in palliation.
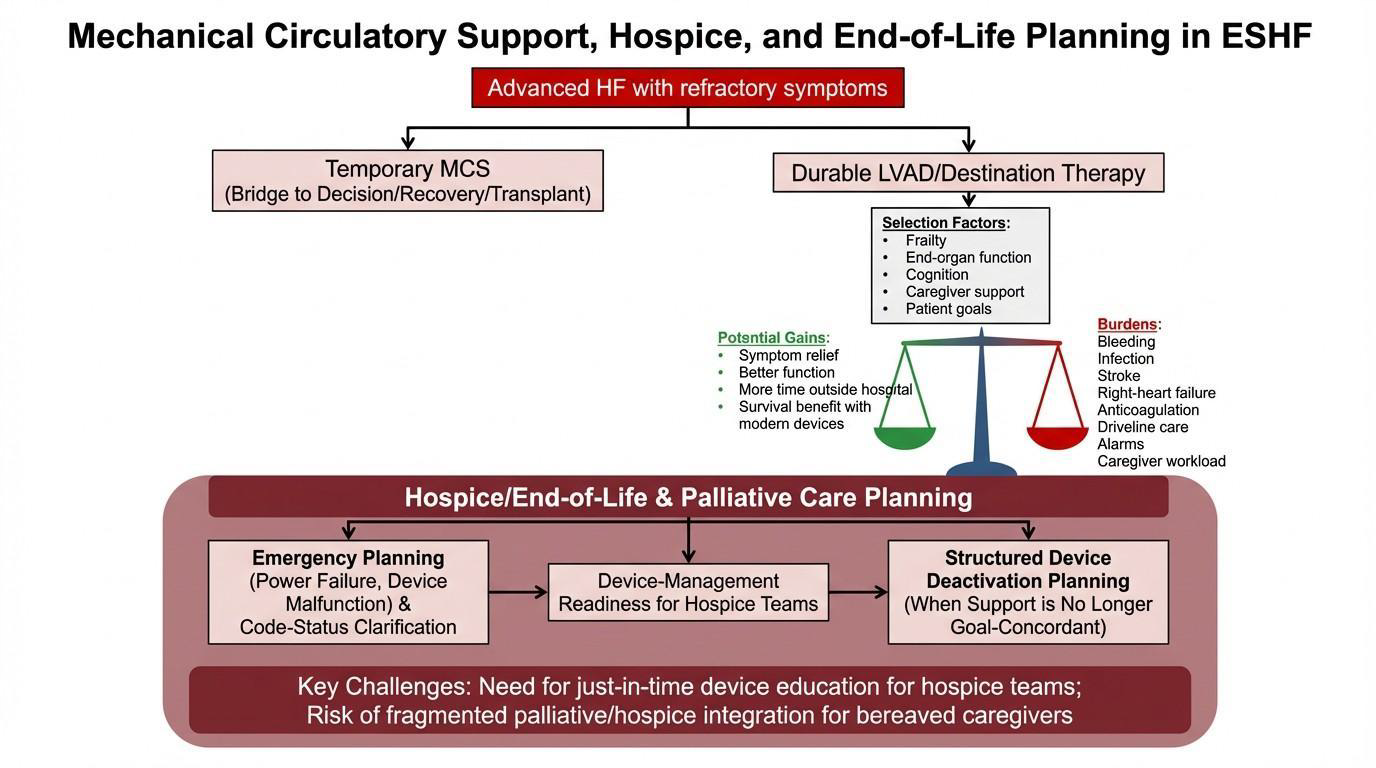
Figure 3. Mechanical circulatory support, hospice, and end-of-life planning in end-stage heart failure.
Hospice Care for ESHF Patients
Hospice care remains an underutilized resource for patients with ESHF, as it may provide comfort-focused care and symptom management. Landmark studies, such as the PAL-HF trial, have shown that patients admitted with heart failure who received care from palliative consultants and a hospice-centered approach reported improved symptom control, better emotional and social functioning, and reduced depression, as compared to aggressive treatment [14,44]. Patients with end-stage disease who have undergone education and grief guidance have repeatedly demonstrated a desire to be outside of the hospital setting towards the end of their life [45]. As misconceptions about hospice are removed, awareness of services such as in-home visits, access to requisite medications and equipment, emergency hotlines, inpatient hospice care when needed, and support for family members through bereavement can further motivate the pursuit of these programs. In congruence, CDC data from 2003 to 2017 showed that the proportion of deaths related to heart failure occurring in hospice facilities rose from 0.2% to 8.2%, and deaths at home rose from 20.6% to 30.7% [43]. Despite growing education and a wide range of benefits, hospice remains underutilized in cardiovascular disease.
Several barriers limit consistent hospice enrollment. Provider-related barriers include reluctance to offer hospice, difficulty identifying appropriate patients, discomfort discussing hospice, and concern that offering hospice could be misconstrued as “giving up”. Patient and family barriers include a lack of awareness of hospice services, the misconception that hospice is only for cancer patients, and the belief that hospice equates to abandoning hope [44]. Rectifications and action plans can include enhanced patient education that clearly distinguishes between palliative and hospice care, emphasizes comfort as a primary goal, highlights proven improvements in mental and social well-being, and reinforces that the aim is to prevent harm through aggressive management [46,47]. A common misconception is that palliative and hospice care are interchangeable. In reality, palliative care is need-based rather than prognosis-based and can be delivered alongside disease-directed therapy. Hospice care, by contrast, is a specific model of palliative care designed for patients nearing the end of life. Palliative care should be seamlessly integrated throughout the heart failure trajectory, with referral to hospice when its philosophy aligns with the patient's and family's goals [47]. In fact, patients should be informed that these approaches have been studied outside the cardiac domain, where early palliative care in end-stage disease has been associated with improved patient outcomes [49].
Given the demonstrated benefits, providers should carefully consider the timing of palliative care involvement in patients with heart failure. Eligibility criteria may vary and often include both disease-specific and treatment-related indicators. Disease-related factors can include advanced states such as cardiac cachexia or multiorgan failure, while treatment-related indicators may involve intolerance to guideline-directed medical therapy or a clinician-estimated life expectancy of ≤6 months, which is consistent with formal hospice eligibility criteria. In addition, needs-based criteria may be particularly useful in guiding appropriate referrals. These include severe physical symptoms (≥7/10 on a numeric rating scale), significant emotional burden, spiritual or existential distress, and functional decline marked by dependence in three or more basic activities of daily living [50]. Referral is especially appropriate for patients with an anticipated survival of less than six months, in accordance with the 2022 ACC/AHA/HFSA guidelines.
Psychosocial Support for Loved Ones
A significant factor in patient outcomes across all areas of medicine is the dynamic between patients and their family members. For example, spouses who hold negative perceptions of the illness or demonstrate poor problem-solving skills may contribute to worsening depression in patients [51]. Evidence suggests that mental health therapy can help alleviate some of this burden [52]. Among chronic conditions, heart failure is associated with a particularly poor quality of life, as reported by patients. This is due to a combination of factors, including the disease itself, the complexity of medical regimens, the need for close follow-up and serial testing, frequent hospitalizations, and the influence of family support and stress [51–53]. When families are engaged in care and have a clear understanding of the diagnosis, their ability to support patients at home can significantly improve outcomes [54]. However, the impact of the disease on family members themselves is seldom addressed.
Caregivers assume a substantial burden as primary support systems for patients with chronic illnesses. Their responsibilities are extensive and include managing diet and medications at home, navigating hospitalizations, and learning about the diagnosis and associated treatment plans [51]. A study performed by Schulz and Beach in 1999 found that caregivers experiencing high levels of strain had an increased risk of mortality compared to non-strained caregivers or non-caregiving family members, largely due to exhaustion and depression [55]. Additional polling of family members indicates that caregivers often report a reduced quality of life, due to the level of involvement required to provide adequate care. Notably, quality of life appears to decline further during periods surrounding hospital admissions, reinforcing the association between increased caregiving demands and negative outcomes [55]. Interviews with caregivers suggest a need for improved communication with patients, opportunities to maintain social engagement to reduce isolation, and better education regarding treatment regimens and expected disease trajectories [57–61]. In this context, caregiving often necessitates significant lifestyle adjustments, such as adopting dietary changes alongside the patient, managing medication schedules, coordinating medical appointments, and balancing these responsibilities with their own personal and health needs [60].
Resources available to family members can vary based on their level of involvement, awareness of available resources, and willingness to seek support. Limited studies have examined the impact of providing caregivers with resources, including psychological education, skill teachback, counseling, decision-making assistance, care coordination, and patient-inclusive education [62–64]. In general, these interventions have received positive feedback.
Several validated tools have also been developed to assess caregiver burden and psychological distress, including the Zarit Burden Interview (ZBI) and the Caregiver Strain Index (CSI), which may help identify caregivers at increased risk for burnout, depression, or declining health [65]. The ZBI contains twenty-two questions across several domains, evaluating emotional stress, physical exhaustion, social isolation, financial strain, feelings of guilt, and impact on the caregiver’s personal health, among others. Compared to the ZBI, the CSI is shorter and quicker to administer and focuses more on practical and functional caregiving strain. Routine incorporation of caregiver screening into HF and palliative care visits may facilitate earlier referral to supportive services such as social work, counseling, respite care, caregiver support groups, home health assistance, and palliative care programs. Despite growing recognition of caregiver burden, standardized implementation of these support pathways remains inconsistent across healthcare systems. However, further investigation is needed to assess their effectiveness across different populations and to establish standardized guidelines or screening processes that promote a more integrated, patient-and family-centered treatment approach.
Conclusion
ESHF is marked by an escalating symptom burden, frequent health care utilization, and complex decision-making that extends beyond the scope of disease-directed therapies alone. As this review highlights, palliative care plays a central role in addressing the physical, emotional, and psychosocial needs of patients with ESHF while supporting informed, goal-concordant decisions across ambulatory, inpatient, and end-of-life settings. Evidence consistently demonstrates that early and integrated palliative care improves symptom control, quality of life, advance care planning, and patient–family communication without precluding the use of advanced therapies such as inotropes or mechanical circulatory support. Hospice care, when aligned with patient goals, offers additional benefits through comfort-focused management, caregiver support, and care delivery in preferred settings, yet remains underutilized due to prognostic uncertainty, systemic barriers, and misconceptions surrounding end-of-life care in heart failure. Optimizing care for patients with ESHF requires reframing palliative and hospice services as complementary components of comprehensive heart failure management. Through earlier integration, multidisciplinary collaboration, and individualized care planning, palliative-focused approaches can meaningfully enhance the quality and dignity of care for patients living with and dying from ESHF.
Future Directions
Future efforts should focus on integrating palliative care earlier in the course of end-stage heart failure rather than reserving it for the final stages of disease or repeated hospitalizations. More standardized referral triggers, improved prognostic tools, and closer collaboration among cardiology, primary care, palliative care, hospice, and rehabilitation teams may help ensure that care remains goal-concordant and patient-centered. Additional work is also needed to address the unique challenges faced by patients with MCS devices and to reduce the barriers that continue to limit hospice enrollment in this population. Finally, expanding psychosocial and caregiver support services will be essential to improving quality of life not only for patients with end-stage heart failure, but also for the families who care for them.
References
2. Bozkurt B, Ahmad T, Alexander K, Baker WL, Bosak K, Breathett K, et al. HF STATS 2024: heart failure epidemiology and outcomes statistics an updated 2024 report from the Heart Failure Society of America. J Card Fail. 2025 Jan 1;31(1):66–116.
3. Ammar KA, Jacobsen SJ, Mahoney DW, Kors JA, Redfield MM, Burnett JC Jr, et al. Prevalence and prognostic significance of heart failure stages: application of the American College of Cardiology/American Heart Association heart failure staging criteria in the community. Circulation. 2007 Mar 27;115(12):1563–70.
4. Krumholz HM, Merrill AR, Schone EM, Schreiner GC, Chen J, Bradley EH, et al. Patterns of hospital performance in acute myocardial infarction and heart failure 30-day mortality and readmission. Circ Cardiovasc Qual Outcomes. 2009 Sep;2(5):407–13.
5. Desai AS. The three-phase terrain of heart failure readmissions. Circ Heart Fail. 2012 Jul 1;5(4):398–400.
6. Heidenreich PA, Albert NM, Allen LA, Bluemke DA, Butler J, Fonarow GC, et al. Forecasting the impact of heart failure in the United States: a policy statement from the American Heart Association. Circ Heart Fail. 2013 May;6(3):606–19.
7. Writing Committee; Hollenberg SM, Stevenson LW, Ahmad T, Bozkurt B, Butler J, Davis LL, et al. 2024 ACC Expert Consensus Decision Pathway on Clinical Assessment, Management, and Trajectory of Patients Hospitalized With Heart Failure Focused Update: A Report of the American College of Cardiology Solution Set Oversight Committee. J Am Coll Cardiol. 2024 Sep 24;84(13):1241–67.
8. Diop MS, Bowen GS, Jiang L, Wu WC, Cornell PY, Gozalo P, et al. Palliative Care Consultation Reduces Heart Failure Transitions: A Matched Analysis. J Am Heart Assoc. 2020 Jun 2;9(11):e013989.
9. Hutchinson RN, Gutheil C, Wessler BS, Prevatt H, Sawyer DB, Han PKJ. What is Quality End-of-Life Care for Patients With Heart Failure? A Qualitative Study With Physicians. J Am Heart Assoc. 2020 Sep 15;9(18):e016505.
10. Gelfman LP, Kalman J, Goldstein NE. Engaging heart failure clinicians to increase palliative care referrals: overcoming barriers, improving techniques. J Palliat Med. 2014 Jul;17(7):753–60.
11. Crespo-Leiro MG, Metra M, Lund LH, Milicic D, Costanzo MR, Filippatos G, et al. Advanced heart failure: a position statement of the Heart Failure Association of the European Society of Cardiology. Eur J Heart Fail. 2018 Nov;20(11):1505–35.
12. Morris AA, Khazanie P, Drazner MH, Albert NM, Breathett K, Cooper LB, et al. Guidance for Timely and Appropriate Referral of Patients With Advanced Heart Failure: A Scientific Statement From the American Heart Association. Circulation. 2021 Oct 12;144(15):e238–50.
13. Heidenreich PA, Bozkurt B, Aguilar D, Allen LA, Byun JJ, Colvin MM, et al. 2022 AHA/ACC/HFSA Guideline for the Management of Heart Failure: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. J Am Coll Cardiol. 2022 May 3;79(17):e263–421.
14. Rogers JG, Patel CB, Mentz RJ, Granger BB, Steinhauser KE, Fiuzat M, et al. Palliative Care in Heart Failure: The PAL-HF Randomized, Controlled Clinical Trial. J Am Coll Cardiol. 2017 Jul 18;70(3):331–41.
15. Brännström M, Boman K. Effects of person-centred and integrated chronic heart failure and palliative home care. PREFER: a randomized controlled study. Eur J Heart Fail. 2014 Oct;16(10):1142–51.
16. Wong FK, Ng AY, Lee PH, Lam PT, Ng JS, Ng NH, et al. Effects of a transitional palliative care model on patients with end-stage heart failure: a randomised controlled trial. Heart. 2016 Jul 15;102(14):1100–8.
17. Bakitas MA, Dionne-Odom JN, Ejem DB, Wells R, Azuero A, Stockdill ML, et al. Effect of an Early Palliative Care Telehealth Intervention vs Usual Care on Patients With Heart Failure: The ENABLE CHF-PC Randomized Clinical Trial. JAMA Intern Med. 2020 Sep 1;180(9):1203–13.
18. Chuzi S, Saylor MA, Allen LA, Desai AS, Feder S, Goldstein NE, Groninger H, Kirkpatrick JN, Tulsky JA, Steiner JM, Lever N. Integration of palliative care into heart failure care: consensus-based recommendations from the Heart Failure Society of America. J Card Fail. 2025 Mar 1;31(3):559–73.
19. Bohula EA, Landzberg MJ, Menon V, Alviar CL, Barsness GW, Crousillat DR, et al. Palliative and End-of-Life Care During Critical Cardiovascular Illness: A Scientific Statement From the American Heart Association. Circulation. 2025 Jun 17;151(24):e1075–90.
20. Sidebottom AC, Jorgenson A, Richards H, Kirven J, Sillah A. Inpatient palliative care for patients with acute heart failure: outcomes from a randomized trial. J Palliat Med. 2015 Feb;18(2):134–42.
21. O'Donnell AE, Schaefer KG, Stevenson LW, DeVoe K, Walsh K, Mehra MR, et al. Social Worker-Aided Palliative Care Intervention in High-risk Patients With Heart Failure (SWAP-HF): A Pilot Randomized Clinical Trial. JAMA Cardiol. 2018 Jun 1;3(6):516–9.
22. Bhattacharya A, Chakrabarty S, Cabrales J, VanHorn A, Lemoine J, Tsao L, et al. Implementation of a palliative care consultation trigger tool for hospitalised patients with acute decompensated heart failure. BMJ Open Qual. 2023 Aug;12(3):e002330.
23. Kitzman DW, Whellan DJ, Duncan P, Pastva AM, Mentz RJ, Reeves GR, et al. Physical Rehabilitation for Older Patients Hospitalized for Heart Failure. N Engl J Med. 2021 Jul 15;385(3):203–16.
24. Pandey A, Kitzman DW, Nelson MB, Pastva AM, Duncan P, Whellan DJ, et al. Frailty and Effects of a Multidomain Physical Rehabilitation Intervention Among Older Patients Hospitalized for Acute Heart Failure: A Secondary Analysis of a Randomized Clinical Trial. JAMA Cardiol. 2023 Feb 1;8(2):167–76.
25. Dias KJ, Shoemaker MJ, Lefebvre KM, Heick JD. A Knowledge Translation Framework for Optimizing Physical Therapy in Patients With Heart Failure. Phys Ther. 2021 Jun 1;101(6):pzab079.
26. Ahmadizadeh Z, Shanbehzadeh S, Taghavi S, Kessler D, Khaleghparast S, Akbarfahimi M. Occupational Performance Coaching on Health Self-Care Behavior and Activity Participation for Adults With Heart Failure: A Randomized Controlled Trial. Am J Occup Ther. 2025 Jan 1;79(1):7901205130.
27. Allen LA, Hernandez AF, Peterson ED, Curtis LH, Dai D, Masoudi FA, et al. Discharge to a skilled nursing facility and subsequent clinical outcomes among older patients hospitalized for heart failure. Circ Heart Fail. 2011 May;4(3):293–300.
28. Weerahandi H, Bao H, Herrin J, Dharmarajan K, Ross JS, Jones S, et al. Home Health Care After Skilled Nursing Facility Discharge Following Heart Failure Hospitalization. J Am Geriatr Soc. 2020 Jan;68(1):96–102.
29. Packer M, Carver JR, Rodeheffer RJ, Ivanhoe RJ, DiBianco R, Zeldis SM, et al. Effect of oral milrinone on mortality in severe chronic heart failure. The PROMISE Study Research Group. N Engl J Med. 1991 Nov 21;325(21):1468–75.
30. Cuffe MS, Califf RM, Adams KF Jr, Benza R, Bourge R, Colucci WS, et al. Short-term intravenous milrinone for acute exacerbation of chronic heart failure: a randomized controlled trial. JAMA. 2002 Mar 27;287(12):1541–7.
31. O'Connor CM, Gattis WA, Uretsky BF, Adams KF Jr, McNulty SE, Grossman SH, et al. Continuous intravenous dobutamine is associated with an increased risk of death in patients with advanced heart failure: insights from the Flolan International Randomized Survival Trial (FIRST). Am Heart J. 1999 Jul;138(1 Pt 1):78–86.
32. Eaton RE, Kissling KT, Haas GJ, McLaughlin EM, Pickworth KK. Rehospitalization of Patients with Advanced Heart Failure Receiving Continuous, Palliative Dobutamine or Milrinone. Am J Cardiol. 2022 Dec 1;184:80–9.
33. Gentile P, Masciocco G, Palazzini M, Tedeschi A, Ruzzenenti G, Conti N, et al. Intravenous continuous home inotropic therapy in advanced heart failure: Insights from an observational retrospective study. Eur J Intern Med. 2023 Oct;116:65–71.
34. Heidenreich PA, Bozkurt B, Aguilar D, Allen LA, Byun JJ, Colvin MM, et al. 2022 AHA/ACC/HFSA Guideline for the Management of Heart Failure: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. Circulation. 2022 May 3;145(18):e895–1032.
35. Tedford RJ, Leacche M, Lorts A, Drakos SG, Pagani FD, Cowger J. Durable Mechanical Circulatory Support: JACC Scientific Statement. J Am Coll Cardiol. 2023 Oct 3;82(14):1464–81.
36. Molina EJ, Shah P, Kiernan MS, Cornwell WK 3rd, Copeland H, Takeda K, et al. The Society of Thoracic Surgeons Intermacs 2020 Annual Report. Ann Thorac Surg. 2021 Mar;111(3):778–92.
37. Mehra MR, Uriel N, Naka Y, Cleveland JC Jr, Yuzefpolskaya M, Salerno CT, et al. A Fully Magnetically Levitated Left Ventricular Assist Device - Final Report. N Engl J Med. 2019 Apr 25;380(17):1618–27.
38. Kirklin JK. The 2023 ISHLT guidelines for durable mechanical circulatory support: A must read for all advanced heart failure practitioners. J Heart Lung Transplant. 2023 Jul;42(7):847–8.
39. Teuteberg W, Maurer M. Palliative Care Throughout the Journey of Life With a Left Ventricular Assist Device. Circ Heart Fail. 2016 Oct;9(10):e003564.
40. Chuzi S, Saylor MA, Allen LA, Desai AS, Feder S, Goldstein NE, et al. Integration of palliative care into heart failure care: consensus-based recommendations from the Heart Failure Society of America. J Card Fail. 2025 Mar 1;31(3):559–73.
41. McIlvennan CK, Jones J, Allen LA, Swetz KM, Nowels C, Matlock DD. Bereaved Caregiver Perspectives on the End-of-Life Experience of Patients With a Left Ventricular Assist Device. JAMA Intern Med. 2016 Apr;176(4):534–9.
42. Makdisi T, Makdisi G. Ethical challenges and terminal deactivation of left ventricular assist device. Ann Transl Med. 2017 Aug;5(16):331.
43. Pandey D, Mahmood A, Harounian J, Fleming-Damon C, Mencias M, Portenoy RK, et al. Providing End-of-Life Care for Patients With Left Ventricular Assist Devices: Experience of a Hospice Agency. J Pain Symptom Manage. 2021 May;61(5):891–7.
44. Braun LT, Grady KL, Kutner JS, Adler E, Berlinger N, Boss R, et al. Palliative Care and Cardiovascular Disease and Stroke: A Policy Statement From the American Heart Association/American Stroke Association. Circulation. 2016 Sep 13;134(11):e198–225.
45. Bajwah S, Oluyase AO, Yi D, Gao W, Evans CJ, Grande G, et al. The effectiveness and cost-effectiveness of hospital-based specialist palliative care for adults with advanced illness and their caregivers. Cochrane Database Syst Rev. 2020 Sep 30;9(9):CD012780.
46. Cardenas V, Rahman A, Zhu Y, Enguidanos S. Reluctance to Accept Palliative Care and Recommendations for Improvement: Findings From Semi-Structured Interviews With Patients and Caregivers. Am J Hosp Palliat Care. 2022 Feb;39(2):189–95.
47. Hupcey JE. The state of palliative care and heart failure. Heart Lung. 2012 Nov-Dec;41(6):529–30.
48. Kavalieratos D, Gelfman LP, Tycon LE, Riegel B, Bekelman DB, Ikejiani DZ, Goldstein N, Kimmel SE, Bakitas MA, Arnold RM. Palliative Care in Heart Failure: Rationale, Evidence, and Future Priorities. J Am Coll Cardiol. 2017 Oct 10;70(15):1919–30.
49. Courtright KR, Madden V, Bayes B, Chowdhury M, Whitman C, Small DS, et al. Default Palliative Care Consultation for Seriously Ill Hospitalized Patients: A Pragmatic Cluster Randomized Trial. JAMA. 2024 Jan 16;331(3):224–32.
50. Chang YK, Allen LA, McClung JA, Denvir MA, Philip J, Mori M, et al. Criteria for Referral of Patients With Advanced Heart Failure for Specialized Palliative Care. J Am Coll Cardiol. 2022 Jul 26;80(4):332–44.
51. Dunbar SB, Clark PC, Quinn C, Gary RA, Kaslow NJ. Family influences on heart failure self-care and outcomes. J Cardiovasc Nurs. 2008 May-Jun;23(3):258–65.
52. de Leon CF, Grady KL, Eaton C, Rucker-Whitaker C, Janssen I, Calvin J, et al. Quality of life in a diverse population of patients with heart failure: BASELINE FINDINGS FROM THE HEART FAILURE ADHERENCE AND RETENTION TRIAL (HART). J Cardiopulm Rehabil Prev. 2009 May-Jun;29(3):171–8.
53. Chung ML, Moser DK, Lennie TA, Rayens MK. The effects of depressive symptoms and anxiety on quality of life in patients with heart failure and their spouses: testing dyadic dynamics using Actor-Partner Interdependence Model. J Psychosom Res. 2009 Jul;67(1):29–35.
54. Stamp KD, Dunbar SB, Clark PC, Reilly CM, Gary RA, Higgins M, et al. Family context influences psychological outcomes of depressive symptoms and emotional quality of life in patients with heart failure. J Cardiovasc Nurs. 2014 Nov-Dec;29(6):517–27.
55. Schulz R, Beach SR. Caregiving as a risk factor for mortality: the Caregiver Health Effects Study. JAMA. 1999 Dec 15;282(23):2215–9.
56. Luttik ML, Jaarsma T, Veeger NJ, van Veldhuisen DJ. For better and for worse: Quality of life impaired in HF patients as well as in their partners. Eur J Cardiovasc Nurs. 2005 Mar;4(1):11–4.
57. Luttik ML, Blaauwbroek A, Dijker A, Jaarsma T. Living with heart failure: partner perspectives. J Cardiovasc Nurs. 2007 Mar-Apr;22(2):131–7.
58. Mårtensson J, Dracup K, Fridlund B. Decisive situations influencing spouses' support of patients with heart failure: a critical incident technique analysis. Heart Lung. 2001 Sep-Oct;30(5):341–50.
59. Boyd KJ, Murray SA, Kendall M, Worth A, Frederick Benton T, Clausen H. Living with advanced heart failure: a prospective, community based study of patients and their carers. Eur J Heart Fail. 2004 Aug;6(5):585–91.
60. Barnes S, Gott M, Payne S, Parker C, Seamark D, Gariballa S, et al. Characteristics and views of family carers of older people with heart failure. Int J Palliat Nurs. 2006 Aug;12(8):380–9.
61. Aldred H, Gott M, Gariballa S. Advanced heart failure: impact on older patients and informal carers. J Adv Nurs. 2005 Jan;49(2):116–24.
62. Hudson PL, Aranda S, Hayman-White K. A psycho-educational intervention for family caregivers of patients receiving palliative care: a randomized controlled trial. J Pain Symptom Manage. 2005 Oct;30(4):329–41.
63. Given B, Sherwood PR. Family care for the older person with cancer. Semin Oncol Nurs. 2006 Feb;22(1):43–50.
64. Martire LM. The "relative" efficacy of involving family in psychosocial interventions for chronic illness: are there added benefits to patients and family members? In: Database of Abstracts of Reviews of Effects (DARE): Quality-assessed Reviews [Internet]. York (UK): Centre for Reviews and Dissemination (UK); 1995.
65. Domeisen Benedetti F, Hechinger M, Fringer A. Self-Assessment Instruments for Supporting Family Caregivers: An Integrative Review. Healthcare (Basel). 2024 May 14;12(10):1016.