Abstract
Spondylolysis, a defect of the pars interarticularis, is a frequent cause of low back pain in young adults. A 19-year-old male presented with a year of chronic pain that recently worsened, limiting ambulation. He denied trauma, fever, neurological symptoms, or bowel/bladder dysfunction. Examination revealed an antalgic gait without focal tenderness or deficits. Given the underlying chronicity and functional limitation in a young patient, lumbar radiographs were obtained, which demonstrated a pars defect at L4. Spondylolysis most commonly involves L5, may progress to spondylolisthesis, and is strongly associated with repetitive lumbar stress, particularly in athletes. Current imaging guidelines discourage routine radiography for uncomplicated low back pain without red flags; however, selective imaging may be warranted when clinical features increase the pre-test probability of structural pathology. Management is typically conservative with activity modification, physical therapy, and selective bracing, with surgery reserved for refractory cases. This case underscores individualized imaging decisions in young patients with disabling symptoms and highlights an uncommon L4 presentation.
Keywords
Spondylolysis, Pars interarticularis defect, Low back pain, Lumbar spine, Radiography, Spondylolisthesis, Scottie dog sign, Athletes, Conservative management
Introduction
Spondylolysis is a defect or stress fracture of the pars interarticularis and represents a common cause of low back pain in adolescents and young adults. It is most frequently localized at L5, followed by L4, and is associated with repetitive lumbar extension/rotation and sport-related loading. Familial clustering and ethnic variation suggest a genetic predisposition [1–3]. Recent reviews reaffirm the burden of pars injuries in athletic populations and emphasize conservative care as first-line management [4, 5]. Despite its prevalence, diagnosis may be delayed due to nonspecific clinical features; therefore, recognizing radiographic signs, particularly the Scottie dog sign, remains essential for frontline clinicians.
Case Report
A 19-year-old, physically active male with no significant past medical history presented to the emergency department with worsening low back pain. He reported approximately one year of chronic, non-radiating pain that acutely worsened over the prior two weeks and was now limiting ambulation with an antalgic gait. He denied trauma, fever, bowel or bladder incontinence, paresthesia, or weakness. Over-the-counter analgesics provided only transient relief. On examination, he appeared well. Gait assessment confirmed an antalgic pattern. There was no midline spinal tenderness, deformity, or neurological deficit. Given the prolonged symptom duration and functional limitation, lumbosacral radiography was obtained, revealing a pars interarticularis defect at L4 consistent with spondylolysis (Figure 1). Conservative management with rest, analgesics, activity modification, and referral to physical therapy was initiated. A spine specialist referral was arranged from the ED for outpatient follow-up.
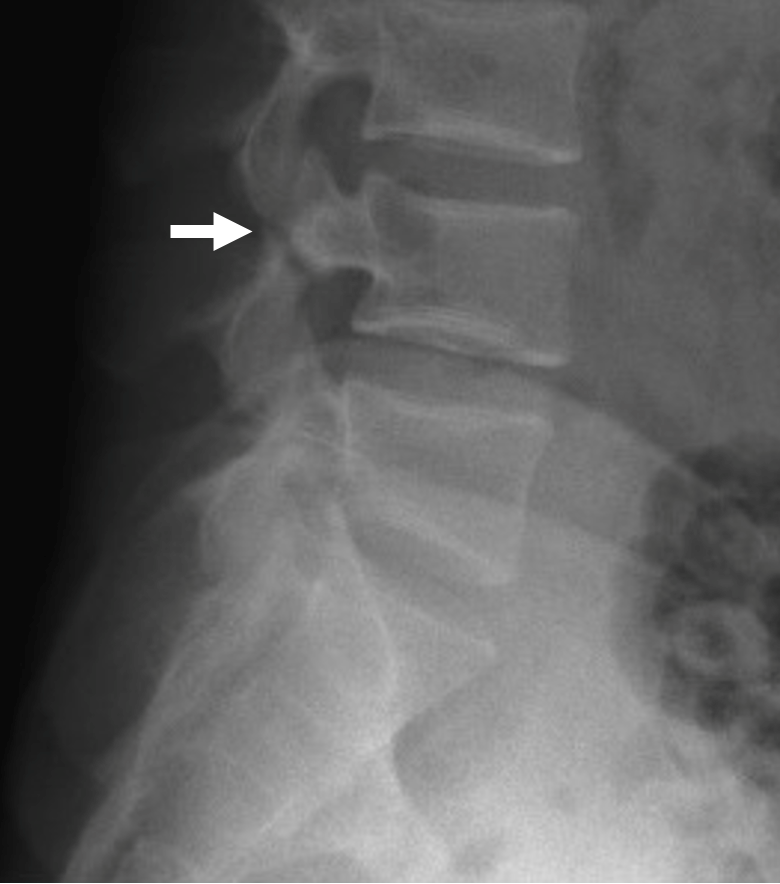
Figure 1. Lateral lumbosacral spine radiograph indicating a pars interarticularis defect at L4 (white arrow).
Discussion
Epidemiology and level
Spondylolysis most often affects L5 (≈85–95%), followed by L4 (≈5–15%), and may progress to spondylolisthesis in a subset of cases [6]. Contemporary athletic cohorts continue to show substantial prevalence in adolescents and young adults [4, 5]. Although L4 involvement is less common, there does not appear to be a consistent difference in prognosis solely by level; progression risk relates more to factors such as bilaterality, persistent pain, and chronic defects. A 2024 systematic review highlights imaging features that may predict progression from spondylolysis to spondylolisthesis [7].
Imaging considerations and "Scottie dog" sign
On oblique radiographs, the pars defect is classically visualized as a cortical defect in the "neck" of the Scottie dog sign, aiding rapid recognition and triage in acute care settings. In this case, an annotated lateral radiograph (Figure 1) indicates the L4 defect.
Guidelines and selective imaging
The American College of Radiology (ACR) Appropriateness Criteria advise that imaging is usually not appropriate for initial evaluation of uncomplicated acute, subacute, or chronic low back pain without red flags [8]. However, guidelines also recognize that imaging may be appropriate when symptoms persist, function is significantly limited, or when surgical/interventional planning is contemplated. In this young patient with acute-on-chronic symptoms and an antalgic gait, selective radiography rendered the diagnosis and expedited referral. In addition to clinical yield, well-targeted imaging can mitigate costs and unnecessary radiation exposure, prevent prolonged diagnostic uncertainty, and reduce the need for repeat visits [9].
Conservative management (standard of care)
Initial treatment includes activity modification (limiting hyperextension/rotation), a phased physical therapy program emphasizing lumbopelvic stabilization and progressive return to sport, and short-term analgesia [4,5]. Short-term bracing may be considered for pain control and to facilitate bone healing in select patients [4]. Return to activity is anticipated over several weeks to months, and tailored to the patient's symptoms and functional progression. For patients with refractory pain or instability, surgical intervention remains an option. The patient in this case was referred to a spine specialist with an expected favorable prognosis for recovery through conservative management.
Prevention in youth/athletes
Technique refinement (avoiding excessive lumbar extension), periodized training/load management, core and hip strengthening, and early reporting of back symptoms may reduce the risk of pars stress injury and improve outcomes [4,5].
Clinical contribution of this case
This report emphasizes judicious, patient-centered imaging in young adults with disabling symptoms, illustrates a didactic sign (Scottie dog), and adds to the literature on the less common L4 localization.
Conclusion
This case highlights an uncommon presentation of L4 spondylolysis in a young adult. While current guidelines discourage routine lumbar radiographs for low back pain, selective imaging remains appropriate when symptoms are prolonged and functionally limiting. In such patients, targeted radiography can clarify the diagnosis, guide conservative management, and help prevent progression to spondylolisthesis.
Acknowledgments
None.
Author Contributions Statement
ZW: patient care, data collection, figure annotation request/preparation, manuscript drafting, manuscript revision. Final approval by the sole author.
Conflicts of Interest
The author declares no conflicts of interest.
Funding Statement
No funding was received.
References
2. Tower SS, Pratt WB. Spondylolysis and associated spondylolisthesis in Eskimo and Athabascan populations. Clinical Orthopaedics and Related Research®. 1990 Jan 1;250:171–5.
3. Kato K, Hakozaki M, Mashiko R, Konno SI. Familial development of lumbar spondylolysis: a familial case report of 7-and 4-year-old brothers and their father. Journal of International Medical Research. 2021 May;49(5):03000605211015559.
4. Choi JH, Ochoa JK, Lubinus A, Timon S, Lee YP, Bhatia NN. Management of lumbar spondylolysis in the adolescent athlete: a review of over 200 cases. The Spine Journal. 2022 Oct 1;22(10):1628–33.
5. Lima MV, Caffaro MF, Santili C, Watkins IV RG. Spondylolysis and Spondylolisthesis in Athletes. Revista Brasileira de Ortopedia. 2024 May 20;59(1):e10–6.
6. Standaert CJ, Herring SA. Spondylolysis: a critical review. British journal of sports medicine. 2000 Dec 1;34(6):415–22.
7. Sima S, Chen X, Sheldrick K, Lu A, Diwan AD. Imaging predictors of progression of lumbar spondylolysis to spondylolisthesis: a systematic review. The Spine Journal. 2024 Aug 1;24(8):1431–42.
8. Hutchins TA, Peckham M, Shah LM, Parsons MS, Agarwal V, Boulter DJ, et al. ACR appropriateness criteria® low back pain: 2021 update. Journal of the American College of Radiology. 2021 Nov 1;18(11):S361–79.
9. Kjelle E, Brandsæter IØ, Andersen ER, Hofmann BM. Cost of low-value imaging worldwide: a systematic review. Applied health economics and health policy. 2024 Jul;22(4):485–501.