Abstract
Atypical hemolytic uremic syndrome (aHUS) is a rare, life-threatening thrombotic microangiopathy (TMA) caused by complement dysregulation, often leading to end-stage renal disease and death. Recent real-world and post-marketing surveillance studies underscore the critical importance of initiating eculizumab, a terminal complement inhibitor, within seven days of disease onset, which is associated with sustained inhibition of TMA and marked improvement in renal outcomes and survival compared with delayed treatment. We report the clinical course of a 61-year-old previously healthy woman with aHUS who received early empiric eculizumab therapy. She initially presented with intractable vomiting and was hospitalized with a presumed diagnosis of acute pancreatitis; however, diagnostic imaging was unremarkable. On the next day of her hospitalization, laboratory findings consistent with TMA emerged, accompanied by rapid deterioration in renal function and platelet counts, prompting initiation of eculizumab on day 3. Treatment resulted in rapid inhibition of TMA, with substantial improvement in hematologic parameters and renal function reaching near-normal levels by hospital discharge (day 24), with continued improvement observed at follow-up (day 47). This case reinforces the importance of early eculizumab initiation in aHUS and aligns with real-world evidence demonstrating rapid clinical recovery and potential economic benefits through reduced hospitalization and healthcare costs.
Keywords
Atypical hemolytic uremic syndrome, Thrombotic microangiopathies, Eculizumab
Introduction
Idiopathic atypical Hemolytic Uremic Syndrome (aHUS) is a rare, yet devastating TMA marked by hemolytic anemia, thrombocytopenia, and acute renal failure, resulting from uncontrolled terminal complement activation [1]. Prognosis in these patients is poor, with nearly one-third of patients either dying or progressing to end-stage renal disease at initial presentation and more than half requiring dialysis or sustaining irreversible renal injury within the first year, frequently culminating in death [2]. Eculizumab (Soliris®), a terminal complement inhibitor, is a humanized monoclonal antibody that binds with high affinity to the C5 complement protein, thereby blocking the generation of the proinflammatory mediators C5a and C5b-9 [3]. Its efficacy in aHUS has been demonstrated in multiple clinical trials, in which eculizumab consistently resolved and prevented complement-mediated TMA, leading to improved renal function and hematologic recovery [3–5]. Recent observational evidence, including a nationwide Japanese study, further underscores the importance of early recognition of aHUS and adherence to eculizumab therapy [6]. Emerging real-world data also highlights the critical role of treatment timing, as initiating eculizumab within seven days of symptom onset correlates with markedly improved renal function and overall survival [7,8]. Here we report the early initiation of eculizumab therapy in a patient with aHUS, which resulted in a rapid and favorable clinical response, including complete inhibition of complement-mediated TMA, normalization of platelet counts, and a significant improvement of renal function.
Case Report
A 61-year-old woman with a past medical history significant for hypertension, Chronic Obstructive Pulmonary Disease (COPD), and type 2 diabetes mellitus presented with acute, intractable vomiting that began a few hours prior to presentation, accompanied by mild, diffuse abdominal pain. On admission (Day 0), physical examination revealed mild abdominal tenderness to palpation in all quadrants, and vital signs demonstrated hypotension (84/50 mmHg) and tachycardia (126 bpm). The remainder of her physical examination and vital signs were within normal limits. Laboratory studies were notable for an elevated lipase of 2213 U/L; all other values, including CBC and CMP, were within normal limits. She was admitted for suspected acute pancreatitis and treated with IV fluids and bowel rest. Subsequent CT abdomen/pelvis with contrast were unremarkable. On the day following her admission (Day 1), laboratory evaluation revealed significant abnormalities, including WBC 23.5 × 10³/µL, ANC 12.0 × 10³/µL, ALC 1.2 × 10³/µL, creatinine 3.28 mg/dL, sodium 128 mmol/L, phosphorus 2.4 mg/dL, magnesium 1.1 mg/dL, total bilirubin 9.0 mg/dL with a direct fraction of 2.0 mg/dL, AST 285 U/L, ALT 109 U/L, haptoglobin <10 mg/dL, LDH 3511 U/L, and a decrease in lipase to 152 U/L. She subsequently developed anuria and required hemodialysis. Hematology/Oncology was consulted to evaluate and manage suspected TTP versus aHUS. The patient was initiated on daily prednisone 60 mg, intravenous immunoglobulin 0.4 g/kg for five days, and plasmapheresis for possible TTP. Despite these interventions, there was no clinical improvement, and the patient’s platelet count, hemoglobin, BUN, and creatinine continued to deteriorate. Accordingly, plasmapheresis was discontinued after two sessions, and the patient was transferred to our tertiary care center, where empirical therapy with eculizumab 900 mg IV weekly was initiated on day 3 for a presumed diagnosis of aHUS. The patient’s hospital course was complicated by worsening mental and respiratory status necessitating intubation and transfer to the ICU on hospital day 4. She required multiple PRBC transfusions for persistent anemia. She was started on trimethoprim-sulfamethoxazole and penicillin for antibiotic prophylaxis and received meningococcal vaccine in the context of eculizumab-induced complement inhibition. Further workup included infectious, autoimmune, and complement studies, as well as assays for PNH and ADAMTS13, all of which were negative and did not indicate TTP or typical HUS (Table 1).
|
Laboratory Tests |
Result |
Interpretation |
Reference Range |
|
ANCA Titer |
<1:20 |
Negative |
<1:20 |
|
ANCA IFA |
None detected |
Negative |
None detected |
|
C3 |
93 |
Normal |
83–193 mg/dL |
|
C4 |
11 |
Low |
15–57 mg/dL |
|
MPO Ab IgG |
0 |
Negative |
0 –19 AU/mL |
|
dsDNA |
<1:10 |
Normal |
<1:10 |
|
ANA |
Negative |
Negative |
Negative |
|
Scl-70 |
<1.0 Neg |
Normal |
<1.0 Neg |
|
ADAMTS13 |
0.61 |
Not indicative of TTP |
0.68–1.63 IU/mL |
|
Lupus Anticoagulant |
Not detected |
Negative |
Not detected |
|
Hep A IgM |
Non-reactive |
Negative |
Non-reactive |
|
Hep B Core Ab (IgM) |
Non-reactive |
Negative |
Non-reactive |
|
Hep C Ab |
Non-reactive |
Negative |
Non-reactive |
|
Cardiolipin Ab |
<2.0 |
Normal |
<2.0 APL-U/mL |
|
Beta-2 Glycoprotein |
<2.0 |
Normal |
<2.0 U/mL |
|
PNH Assay |
Not detected by flow cytometry |
Negative |
Not detected by flow cytometry |
|
Shiga toxin |
Negative |
Negative |
Negative |
|
GI Pathogen Panel |
Not detected |
Negative |
Not detected |
|
Stool Culture |
Normal flora |
Normal |
Normal flora |
|
CMV Ab |
<30.0 |
Negative |
<30.0 AU/mL |
|
HIV Ag/Ab 4th Gen |
Non-reactive |
Negative |
Non-reactive |
|
EBV DNA |
<35.0 |
Normal |
<35.0 IU/mL |
|
TB Quantiferon |
Not detected |
negative |
Not detected |
|
Diagnostic workups were performed between Day 0 (hospital admission) and Day 15 to confirm the etiology and for differential diagnosis. Majority of the autoimmune workup was done on Day 4; however, some pathogen results were not available until Day 15. |
|||
Notably, C4 was below the lower limit of normal; however, this lab was obtained after the first dose of eculizumab. She subsequently received eculizumab on days 7, 14, and 21. Following the second dose, hematologic parameters, including platelet count and haptoglobin normalized, hemoglobin stabilized without the need for additional PRBC transfusions, and LDH levels declined markedly (Figure 1). By hospital day 14, the patient’s mental status and respiratory function had improved sufficiently to permit extubation, and she had begun producing urine. She remained hemodynamically stable and was discharged on hospital day 24. On discharge, the patient remained on dialysis since her creatinine and electrolytes were not normalized (Table 2). At outpatient follow-up on day 47, laboratory assessments, including CBC and CMP, remained stable, with continued improvement of her platelet and hemoglobin, and near normalization of her BUN and creatinine (Table 2). By day 61, the patient was discontinued from dialysis due to complete recovery of renal function, and on day 85, the internal jugular permacath was permanently removed. The patient continued the maintenance treatment with eculizumab.
|
Laboratory Tests |
Baseline (Day 0) |
Start of Eculizumab (Day 3) |
Day of Discharge (Day 24) |
Follow-up Visit (Day 47) |
Reference Ranges |
|
Hgb |
15.1 |
7.06 |
7.1 |
9.5 |
11.0–15.5 g/dL |
|
WBC |
11.2 |
13.9 |
9.4 |
11.92 |
4.00–10.10 x103/µL |
|
Platelet count |
243 |
9.33 |
222 |
315 |
140–425 x103/µL |
|
Reticulocyte count |
2.59% |
3.3% |
4.54% |
NA |
0.40–2.50 % |
|
Schistocytes |
1+ (Slight) |
2+ (Moderate) |
NA |
NA |
0 |
|
Haptoglobin |
<10 |
<10 |
186 |
NA |
30–200 mg/dL |
|
BUN |
15 |
84 |
44 |
32 |
8–23 mg/dL |
|
Cr |
0.72 |
5.22 |
6.13 |
1.43 |
0.49–1.02 mg/dL |
|
Total bilirubin |
0.6 |
1.7 |
0.2 |
<0.2 |
<1.2 mg/dL |
|
LDH |
3511 |
4097 |
324 |
NA |
120–246 U/L |
|
Sodium |
129 |
132 |
126 |
135 |
135–147 mmol/L |
|
Potassium |
4.7 |
5.2 |
5.5 |
4.6 |
3.5–5.5 mmol/L |
|
Chloride |
94 |
95 |
89 |
93 |
96–108 mmol/L |
|
ALT |
48 |
49 |
15 |
16 |
<33 U/L |
|
AST |
45 |
210 |
15 |
23 |
<32 U/L |
|
ALP |
135 |
55 |
79 |
142 |
40–156 U/L |
|
Albumin |
3.6 |
2.9 |
2.3 |
3.6 |
3.5–5.2 g/dL |
|
Fibrinogen |
NA |
116 |
223* (Day 10) |
NA |
194–448 mg/dL |
|
PT |
16.3 |
NA |
10.9* (Day 17) |
NA |
9.6–12.4 sec |
|
PTT |
35 |
NA |
29* (Day 17) |
NA |
- 31 sec |
|
Clinical laboratory values during patient hospitalization and course of the eculizumab treatment. NA: Laboratory values were not available/ not done. *Fibrinogen, PT and PTT assays were performed on different days as specified, before the day of discharge. |
|||||
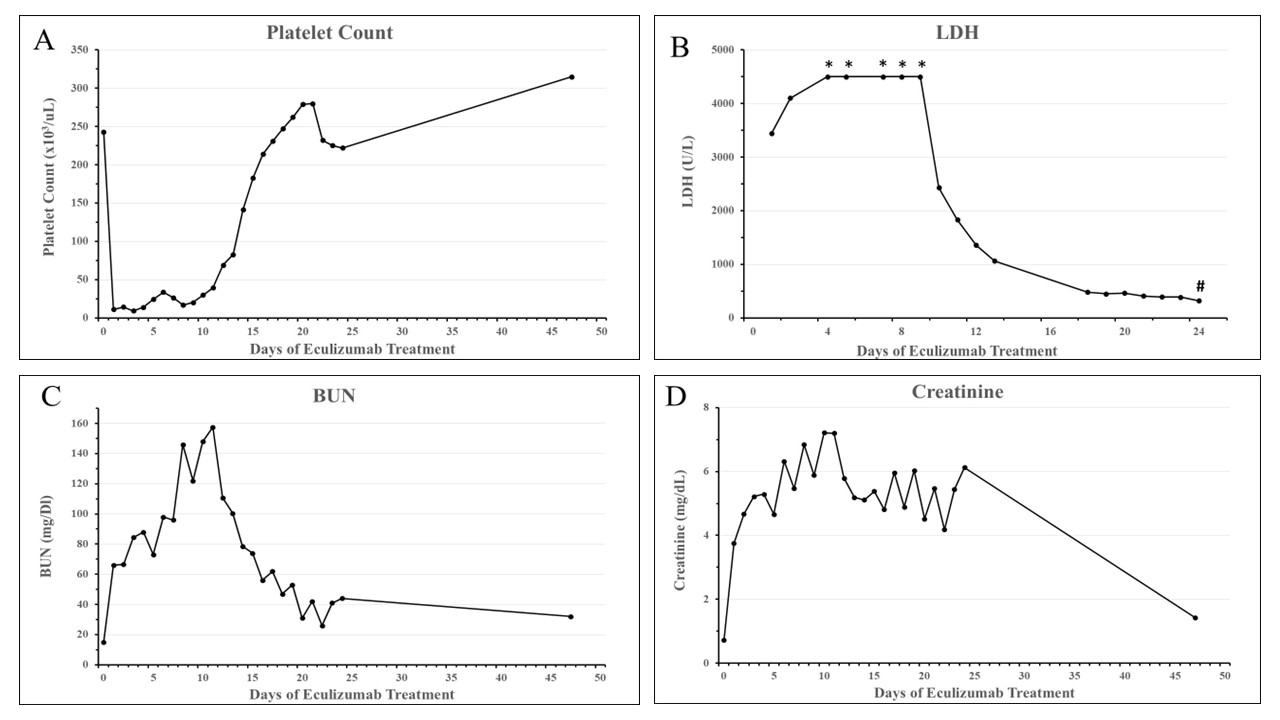
Figure 1. Rapid improvement of hematological parameters and renal function by early intervention with eculizumab. The patient was hospitalized on Day 0, eculizumab 900 mg weekly IV started on Day 3, and the patient was discharged on Day 24. An outpatient follow-up visit was performed on Day 47. A) Platelet count. B) Serum LDH. Day 0 value of LDH was not available. * Day 4, 5, 7, 8, and 9 LDH values were reported as >4500 U/L. # LDH laboratory test was not performed on the follow-up visit on Day 47. C) BUN. D) Creatinine.
Discussion
aHUS is a rare, severe, and frequently relapsing TMA defined by the triad of thrombocytopenia, microangiopathic hemolytic anemia, and acute kidney injury [9]. aHUS occurs in the absence of Shiga toxin–producing Escherichia coli infection and without severe ADAMTS13 deficiency (<10%), which excludes TTP [10]. It accounts for approximately 5–10% of all hemolytic uremic syndrome cases and is associated with substantial morbidity and mortality, particularly when untreated [1].
The etiology of complement dysregulation in aHUS results from either inherited or acquired defects of the complement system [11,12]. Renal pathology is marked by TMA involving the glomerular capillaries, often with additional thrombotic occlusions affecting arterioles and interlobular arteries. These lesions arise from uncontrolled activation of the alternative complement pathway, leading to excessive complement deposition and endothelial injury with a strong predilection for the renal microvasculature [13]. Diagnostic differentiation of aHUS remains challenging because the precipitating factors of aHUS may overlap with secondary etiologies, thereby obscuring the accurate diagnosis of primary aHUS [14].
Prospective clinical studies, including two pivotal trials by Legendre et al., demonstrated that eculizumab induces a rapid and sustained inhibition of complement-mediated TMA, resulting in significant long-term improvements in renal function [3–5]. Following eculizumab initiation, eGFR steadily increased, and proteinuria markedly decreased, indicating progressive renal recovery despite chronic pre-existing injury. In these trials early initiation of eculizumab was strongly associated with greater gains in eGFR throughout the treatment period (P = 0.007 in Trial 1; P<0.001 in Trial 2) [3].
In the majority of previously reported cases, eculizumab therapy was initiated only after substantial renal injury had developed, leaving most patients with persistent renal insufficiency and irreversible kidney damage [15–17]. In contrast, in our case, empiric eculizumab was initiated early while the differential diagnosis was still under evaluation. This approach aimed to promptly inhibit complement-mediated TMA and prevent progression to irreversible renal injury.
Although a comprehensive diagnostic workup conducted during the patient’s hospitalization (Days 1–15) to evaluate potential differential diagnoses and elucidate the etiology of aHUS (Table 1), the classic hematologic features, coupled with a rapid decline in eGFR and renal function, prompted the early initiation of eculizumab on Day 3. Continued eculizumab therapy resulted in rapid suppression of complement-mediated TMA, accompanied by significant improvements in platelet counts, LDH levels, and renal function (Figure 1). By the time of discharge (Day 24), laboratory parameters, including hematologic indices, liver function tests, LDH, and renal markers, had returned to or approached normal ranges and demonstrated further improvement at the outpatient follow-up on Day 47 (Table 2).
Indeed, recent studies highlight the importance of early intervention in aHUS with eculizumab therapy [7, 8,18, 19]. In a post-marketing surveillance study, multivariate analysis demonstrated an inverse relationship between the time from the most recent TMA episode to the initiation of eculizumab therapy and subsequent improvement in renal function [18]. Evidence from real-world studies similarly underscores the value of early treatment. In a retrospective study of 17 patients with aHUS, Hu et al. reported markedly superior outcomes among those who were treated with eculizumab ≤7 days of symptom onset compared with those who received delayed treatment (>7 days) [8]. Early therapy resulted in significantly higher rates of renal remission (88.9% vs. 12.5%, P = 0.003) and hematologic remission (100% vs. 12.5%, P < 0.001), as well as a substantial reduction in dialysis dependence (0% vs. 87.5%, P<0.001). Renal survival also favored early initiation (log-rank P<0.001), with notable improvements in eGFR and platelet recovery [8].
In a post-hoc analysis of pooled data from four phase 2 studies, Walle et al. demonstrated that aHUS patients treated with eculizumab within 7 days of disease onset had significantly greater 1-year gains in eGFR compared with those treated later. Sustained improvement was achieved in 81% of early-treated patients versus 47% of those treated later [7]. These findings are consistent with observations from a genotype-matched aHUS cohort, in which a shorter interval between clinical presentation and the first eculizumab dose was associated with a higher likelihood of achieving eGFR recovery >60 mL/min at 6 months [19].
The findings of the current case report are consistent with real-world clinical evidence demonstrating that early initiation of eculizumab can lead to rapid renal recovery in patients with aHUS, accompanied by normalization of hematologic parameters. Although eculizumab is the current standard-of-care therapy for aHUS, prescribers should recognize the urgency of early therapeutic intervention for this serious and life-threatening syndrome. Furthermore, early treatment initiation with eculizumab has been shown to provide substantial economic benefits by reducing hospitalization costs, ICU stays, and the need for dialysis or plasmapheresis [20]. Early intervention also improves renal survival, decreasing the risk of progression to end-stage renal disease and lowering the need for kidney transplantation, thereby reducing the economic burden for patients and the healthcare system [20,21]. aHUS is characterized by a substantial risk of relapse, particularly in patients without an identifiable precipitating factor or defined complement abnormality, necessitating structured long-term surveillance and lifelong therapeutic intervention. Ongoing management should be individualized and encompass decisions regarding duration of complement inhibition, laboratory monitoring strategies, and risk mitigation in high-risk settings such as surgery, pregnancy, and transplantation [22].
References
2. Thajudeen B, Sussman A, Bracamonte E. A case of atypical hemolytic uremic syndrome successfully treated with eculizumab. Case Rep Nephrol Urol. 2013 Dec 14;3(2):139–46.
3. Legendre CM, Licht C, Muus P, Greenbaum LA, Babu S, Bedrosian C, et al. Terminal complement inhibitor eculizumab in atypical hemolytic-uremic syndrome. N Engl J Med. 2013 Jun 6;368(23):2169–81.
4. Licht C, Greenbaum LA, Muus P, Babu S, Bedrosian CL, Cohen DJ, et al. Efficacy and safety of eculizumab in atypical hemolytic uremic syndrome from 2-year extensions of phase 2 studies. Kidney Int. 2015 May;87(5):1061–73.
5. Greenbaum LA, Fila M, Ardissino G, Al-Akash SI, Evans J, Henning P, et al. Eculizumab is a safe and effective treatment in pediatric patients with atypical hemolytic uremic syndrome. Kidney Int. 2016 Mar;89(3):701–11.
6. Tatematsu Y, Imaizumi T, Michihata N, Kato N, Kumazawa R, Matsui H, et al. Annual trends in atypical haemolytic uremic syndrome management in Japan and factors influencing early diagnosis and treatment: a retrospective study. Sci Rep. 2024 Aug 6;14(1):18265.
7. Walle JV, Delmas Y, Ardissino G, Wang J, Kincaid JF, Haller H. Improved renal recovery in patients with atypical hemolytic uremic syndrome following rapid initiation of eculizumab treatment. J Nephrol. 2017 Feb;30(1):127–34.
8. Hu Y, Zhang Y, Wang W, Li G, Chen S. Real-World effectiveness of eculizumab in atypical hemolytic uremic syndrome: a retrospective study from Western China. Front Endocrinol (Lausanne). 2025 Jun 27; 16:1568082.
9. Loirat C, Fakhouri F, Ariceta G, Besbas N, Bitzan M, Bjerre A, et al. An international consensus approach to the management of atypical hemolytic uremic syndrome in children. Pediatr Nephrol. 2016 Jan;31(1):15–39.
10. Moake JL. Thrombotic microangiopathies. N Engl J Med. 2002 Aug 22;347(8):589–600.
11. Sellier-Leclerc AL, Fremeaux-Bacchi V, Dragon-Durey MA, Macher MA, Niaudet P, Guest G, et al. Differential impact of complement mutations on clinical characteristics in atypical hemolytic uremic syndrome. J Am Soc Nephrol. 2007 Aug;18(8):2392–400.
12. Dragon-Durey MA, Sethi SK, Bagga A, Blanc C, Blouin J, Ranchin B, et al. Clinical features of anti-factor H autoantibody-associated hemolytic uremic syndrome. J Am Soc Nephrol. 2010 Dec;21(12):2180–7.
13. Davin JC, van de Kar NC. Advances and challenges in the management of complement-mediated thrombotic microangiopathies. Ther Adv Hematol. 2015 Aug;6(4):171–85.
14. Nguyen N, Le T, Tran T, Nguyen N, Chakraborty A, Vu AL, et al. post-COVID-19 vitamin B12 deficiency presenting as pseudo-thrombotic microangiopathy: a case report and review of diagnostic pitfalls. The Egyptian Journal of Internal Medicine. 2025 Sep 16;37(1):132.
15. Rafiq A, Tariq H, Abbas N, Shenoy R. Atypical hemolytic-uremic syndrome: a case report and literature review. Am J Case Rep. 2015 Feb 24; 16:109–14.
16. Garjau M, Azancot M, Ramos R, Sánchez-Corral P, Montero MA, Serón D. Early treatment with eculizumab in atypical haemolytic uraemic syndrome. Clin Kidney J. 2012 Feb;5(1):31–3.
17. Aresmouk D. Severe case of thrombotic microangiopathy with a delayed diagnosis of atypical haemolytic uraemic syndrome successfully managed with eculizumab. European Journal of Case Reports in Internal Medicine. 2015 Mar 25;2(2).
18. Maruyama S, Ikeda Y, Kaname S, Kato N, Matsumoto M, Ishikawa Y, et al. Eculizumab for adult patients with atypical haemolytic-uraemic syndrome: full dataset analysis of Japanese post-marketing surveillance. J Nephrol. 2024 Nov;37(8):2181–90.
19. Brocklebank V, Walsh PR, Smith-Jackson K, Hallam TM, Marchbank KJ, Wilson V, et al. Atypical hemolytic uremic syndrome in the era of terminal complement inhibition: an observational cohort study. Blood. 2023 Oct 19;142(16):1371–86.
20. Ryan M, Donato BMK, Irish W, Gasteyger C, L'Italien G, Laurence J. Economic Impact of Early-in-Hospital Diagnosis and Initiation of Eculizumab in Atypical Haemolytic Uraemic Syndrome. Pharmacoeconomics. 2020 Mar;38(3):307–13.
21. Donato BM, Ryan M, Irish W, Gasteyger C, L'Italien G, Laurence J. Economic Benefit of Early Inhospital Diagnosis and Treatment Initiation of Eculizumab in aHUS. Blood. 2018 Nov 29; 132:3565.
22. Afshar-Kharghan V. Long-term outcome and management of complement-mediated thrombotic microangiopathy/aHUS. Hematology Am Soc Hematol Educ Program. 2025 Dec 5;2025(1):147–53.