Abstract
Myopathies constitute a heterogeneous group of disorders defined by impaired skeletal muscle functions that originate from structural, metabolic, genetic, or inflammatory abnormalities. At the biochemical level, these conditions are characterized by significant disruptions in essential processes, including energy metabolism, calcium homeostasis, and redox balance. For instance, defects in pathways such as glycolysis, fatty acid oxidation, and mitochondrial oxidative phosphorylation severely restrict ATP production, resulting in muscle fatigue, while the concurrent elevation of reactive oxygen species (ROS) triggers oxidative damage and accelerates disease progression. Recent advances in molecular biology have considerably deepened our understanding of the genetic and biochemical mechanisms that drive myopathies, consequently facilitating the development of targeted therapeutic interventions. Current interventions, ranging from antioxidant therapy and metabolic supplementation to gene therapy and enzyme replacement, strive to restore cellular function and decelerate the clinical course. This commentary examines the biochemical foundations of myopathies and critically evaluates emerging strategies for their effective remediation.
Keywords
Myopathy, Oxidative stress, Mitochondrial dysfunction, Calcium homeostasis, Gene therapy, Apoptosis, Necrosis, Autophagy
Introduction
Myopathies represent a highly heterogeneous group of skeletal muscle disorders characterized clinically by debilitating muscle weakness, exertional fatigue, and diminished physical capacity [1,2]. These conditions emerge from diverse etiologies, encompassing genetic mutations, metabolic derangements, inflammatory cascades, and exposure to specific pharmacological agents or toxins. Unlike neuropathic disorders, which stem from lesions within the nervous system, myopathies originate intrinsically within the muscle fibers, leading to direct structural and functional impairment [3,4]. Normal skeletal muscle function is biochemically dependent on the precise, coordinated regulation of multiple cellular processes, notably energy production, calcium signaling, and redox homeostasis [5–7]. To sustain contractile activity, skeletal muscle demands a relentless supply of ATP, synthesized via interconnected pathways such as glycolysis, fatty acid oxidation, and mitochondrial oxidative phosphorylation. The disruption of these bioenergetic pathways directly triggers energy deficiency, compromised contraction, and heightened vulnerability to load-induced muscle damage [8,9]. Furthermore, the loss of intracellular calcium regulation and the unregulated productions of reactive oxygen species (ROS) significantly drive the degenerative process.
Biochemical Classification and Pathophysiology
Clinically, myopathies are broadly classified into inherited (primary) and acquired (secondary) etiologies. Genetic variants such as muscular dystrophies, congenital myopathies, and metabolic myopathies are driven by discrete molecular anomalies that affect structural integrity, energy metabolism, or contractile mechanics, ultimately triggering systemic muscle wasting and functional decline [10,11]. For instance, Duchenne and Becker muscular dystrophies are intrinsically linked to mutations in the dystrophin gene, which potentially lead to a deficiency in the dystrophin protein and subsequent muscle wasting [12,13]. Conversely, metabolic myopathies emerge from specific enzymatic defects within bioenergetic cascades, including glycogen storage diseases, fatty acid oxidation disorders, and mitochondrial myopathies [14]. Acquired myopathies predominantly result from immune-mediated tissue damage, endocrine dysfunction, or infectious insults that compromise muscle metabolism and integrity [15,16].
The underlying pathophysiology of these myopathies is fundamentally linked to localized biochemical failures. Proteostasis imbalance and the dysfunction of structural proteins, like dystrophin, compromise sarcolemma stability, rendering fibers highly susceptible to contraction-induced injury [17,18]. Energy metabolism defects severely limit ATP availability by impairing glycogenolysis and disrupting fatty acid oxidation, thereby starving the muscle during prolonged exertion [19,20]. Compounding these energy deficits is a marked elevation in oxidative stress, where excessive ROS accumulation inflicts lipid peroxidation, protein oxidation, and DNA damage, thereby overwhelming intrinsic antioxidant defenses and exacerbating cellular injury [21]. Concurrently, the dysregulation of calcium homeostasis via sarcoplasmic reticulum dysfunction, promotes pathological intracellular calcium accumulation, which aberrantly activates destructive proteases and accelerates muscle fiber necrosis [22–24].
Molecular and Genetic Architectures
The pathogenic mechanisms of myopathies are basically rooted in genetic mutations that weaken muscle fiber architecture and metabolic capacity [25]. These abnormalities can manifest in both nuclear and mitochondrial genomes across varying inheritance patterns. Beyond primary sequence mutations, disease pathogenesis is heavily influenced by transcriptional and translational defects, including altered mRNA stability, aberrant splicing events, and translational inefficiencies that yield truncated or non-functional proteins [26,27]. RNA processing errors, such as alternative splicing defects, are now recognized as central to the etiology of several myopathies involving sarcomeric and cytoskeletal networks [28,29].
Epigenetic modifications also exert profound regulatory control over muscle cell expression profiles. Dysregulated DNA methylation, aberrant histone modifications, and chromatin remodeling can severely impair the transcriptional networks governing muscle differentiation, regeneration, and metabolic adaptation, thereby propelling disease progression under stress conditions [30,31]. Additionally, mitochondrial genetics is crucial, as mutations in mitochondrial DNA disrupt the cell's energy production, leading to decreased ATP synthesis and increased cellular damage from oxidative stress [32]. Because skeletal muscle possesses massive bioenergetic demands, these mitochondrial defects clearly highlight the interplay between genomic integrity and bioenergetics in myopathic disease.
Cell Death Pathways: Apoptosis, Necrosis, and Autophagy
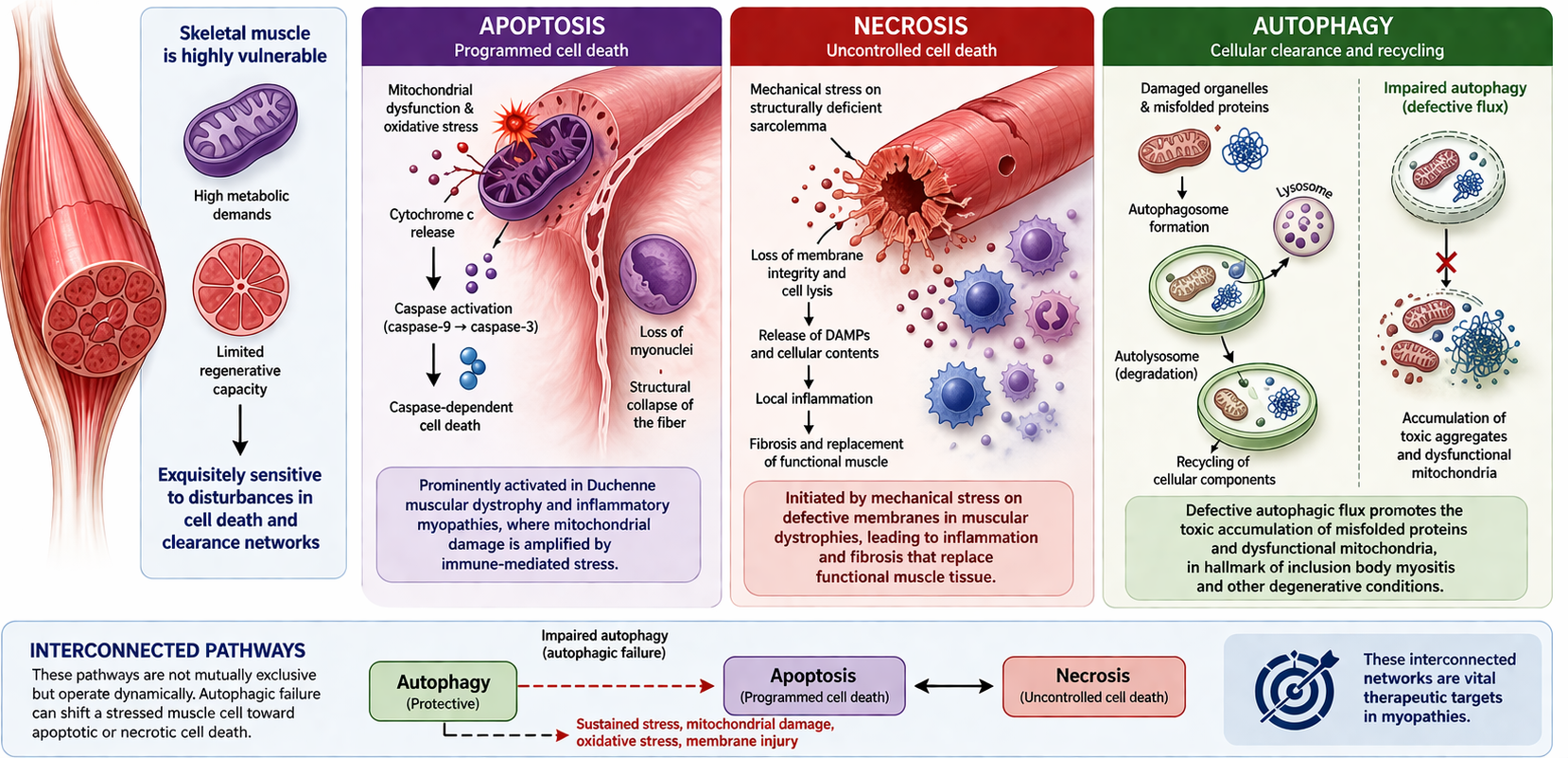
Skeletal muscle degeneration in myopathies stems from the dysregulation of interconnected cell death and clearance pathways [33]. Because skeletal muscle possesses high metabolic requirements and limited regenerative capacity, it is exquisitely sensitive to disturbances in these networks. Apoptosis, which is heavily driven by intrinsic mitochondrial dysfunction and oxidative stress, triggers caspase-dependent cell death, thereby inducing the loss of myonuclei and the structural collapse of individual fibers. This apoptotic signaling is prominently activated in Duchenne muscular dystrophy and inflammatory myopathies, where mitochondrial damage is amplified by immune-mediated stress (Figure 1) [34].
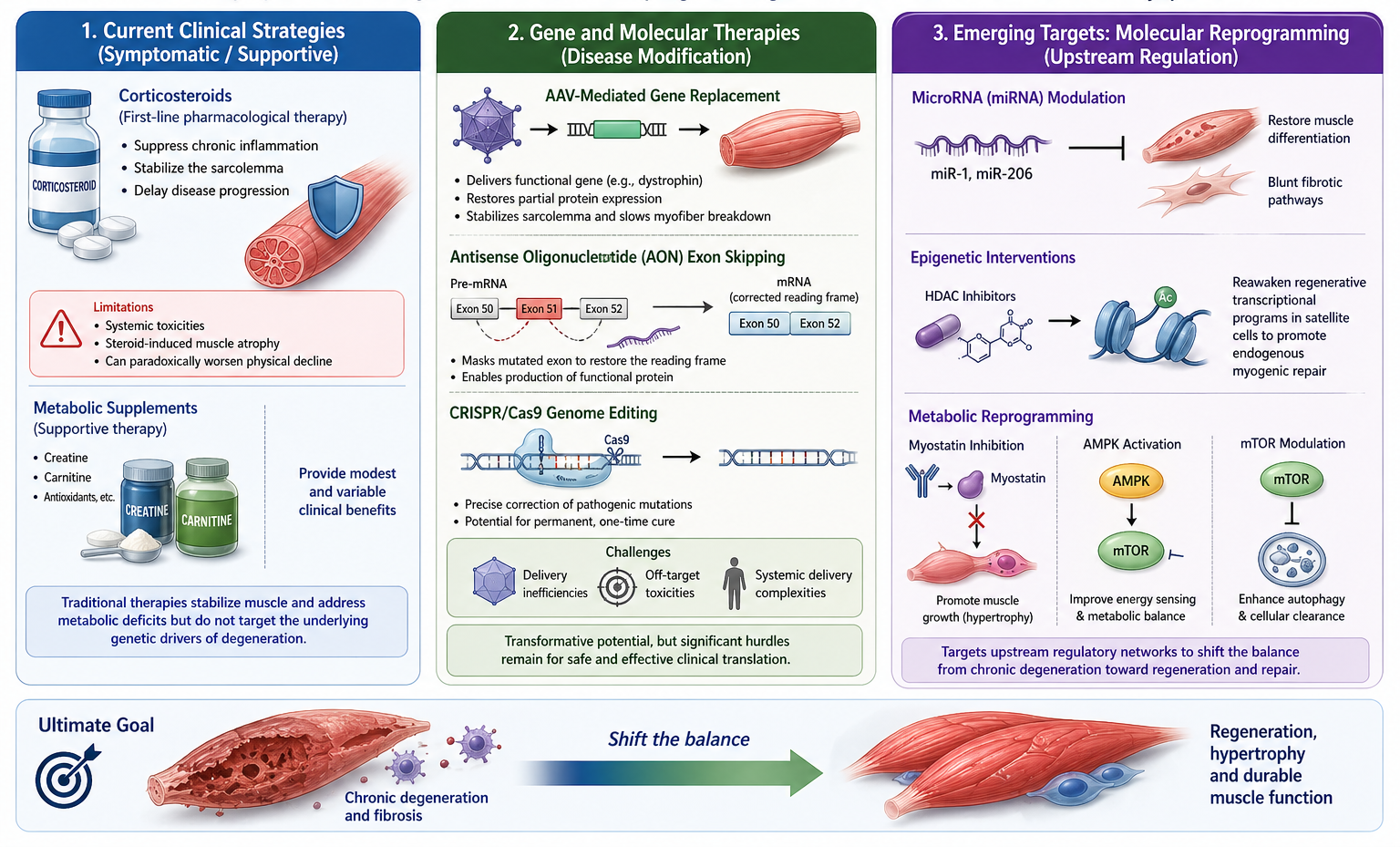
Figure 1. Interconnected cell death and clearance networks in myopathic skeletal muscle.
Conversely, necrosis represents an uncontrolled, cytolytic cell death pathway characterized by the rupture of the sarcolemma [35,36]. In muscular dystrophies, mechanical stress placed on structurally deficient membranes initiates necrosis, inciting a cascade of local inflammation and subsequent fibrosis that ultimately replaces functional muscle tissue. Furthermore, impaired autophagy, a process responsible for the degradation and recycling of damaged organelles, contributes significantly to cellular toxicity. Defective autophagic flux promotes the toxic accumulation of misfolded proteins and dysfunctional mitochondria, a hallmark of inclusion body myositis and other degenerative conditions [37]. Importantly, these pathways are not mutually exclusive but operate dynamically; autophagic failure can readily shift a stressed muscle cell toward apoptotic or necrotic cell death, making these interconnected networks vital therapeutic targets.
Current Remediation Strategies and Emerging Targets
Existing clinical practices for muscular myopathies focus on biochemical remediation that are aimed at stabilizing muscle architecture while attempting to correct underlying metabolic deficits. Corticosteroids remain the cornerstone of traditional pharmacological intervention, due to their ability to delay the progression of disease by suppressing chronic inflammation and stabilizing the sarcolemma [38,39]. However, their long-term utility is significantly undermined by systemic toxicities, most notably steroid-induced muscle atrophy, which can paradoxically exacerbate physical decline. Consequently, current literature categorizes these traditional therapies, including metabolic supplements like creatine and carnitine as primarily symptomatic or supportive, as they often yield modest and variable clinical outcomes without addressing the primary genetic drivers of degeneration.
The most transformative advancements in management currently reside within the realm of gene and molecular therapy. Adeno-associated virus (AAV)-mediated gene replacement and antisense oligonucleotide-driven exon skipping have demonstrated the capacity to restore partial protein expression, such as dystrophin, thereby stabilizing the sarcolemma and slowing myofiber breakdown [40,41]. Furthermore, CRISPR/Cas9 genome editing holds the ultimate promise of permanent mutational correction at the genomic level [43]. While these technologies represent a shift toward definitive disease modification, their clinical application remains challenged by delivery inefficiencies, potential off-target toxicities, and the complexities of achieving systemic therapeutic reach.
Consequently, the field is rapidly transitioning toward the molecular reprogramming of muscle tissue, targeting upstream regulatory networks to counteract downstream pathology. MicroRNA (miRNA) modulation, specifically targeting muscle-specific transcripts like miR-1 and miR-206, has shown the ability to restore differentiation and blunt fibrotic pathways [44]. Parallel epigenetic interventions, such as histone deacetylase (HDAC) inhibitors, seek to reawaken regenerative transcriptional programs within satellite cells to promote endogenous myogenic repair. By manipulating major metabolic nodes such as inhibiting myostatin or modulating the AMPK/mTOR axis, researchers aim to shift the cellular phenotype from a state of chronic degeneration toward one of hypertrophy and enhanced autophagic clearance (Figure 2) [45].
Precision Medicine and Global Disparities
The integration of these advanced therapeutics is the cornerstone of Precision Medicine, a model that designs targeted interventions based on an individual's unique genetic and metabolic architecture. Because shared biological pathways (e.g., calcium dysregulation) can arise from vastly different genetic mutations, generalized treatments often yield suboptimal efficacy or unintended toxicity. By utilizing multi-omics platforms and artificial intelligence, precision medicine allows for précised stratification of disease and optimized pharmacogenomic responses [46,47].
However, the rapid acceleration of these high-cost, highly technical interventions poses a severe risk of widening global health disparities. While well-resourced healthcare systems readily integrate viral vector therapies and NGS diagnostics, low- and middle-income regions, particularly across Africa face profound structural barriers, including insufficient diagnostic infrastructure and prohibitive costs [48]. Without deliberate international policy frameworks focusing on capacity building, equitable pricing, and technology transfer, the gains of genomic medicine will remain inaccessible to a vast portion of the global population, thereby reinforcing existing inequities [49]. Global accessibility therefore must be embedded as a core scientific objective during the early phases of therapeutic research.
Conclusion
Myopathies constitute a multifaceted array of skeletal muscle disorders driven by intersecting genetic, metabolic, and cellular disturbances. The inexorable progression of muscle dysfunction is biochemically rooted to the disruption of energy metabolism, excessive oxidative stress, and the critical failure of calcium homeostasis. While molecular biology has unravelled the complex pathogenic mechanisms and ushered in an era of precision therapeutics that range from gene editing to epigenetic reprogramming, significant technical and systemic challenges remain. Moving forward, the successful remediation of myopathies will demand an integrated, multi-omics approaches that move beyond single-target therapies. Equally critical is the necessity to harmonize these sophisticated scientific advancements with equitable global healthcare frameworks, ensuring that precision medicine delivers transformative clinical benefits to all affected populations, regardless of geographic or socioeconomic boundaries.
References
2. Campuzano-Donoso M, Reytor-González C, Toral-Noristz M, González Y, Simancas-Racines D. Molecular Bases of Myopathies and Their Impact on Clinical Practice: Advances and Future Perspectives. Int J Mol Sci. 2026 Jan 30;27(3):1392.
3. Ziemian M, Szmydtka J, Snoch W, Milner S, Wojciechowski S, Dłuszczakowska A, et al. Integrative Approaches to Myopathies and Muscular Dystrophies: Molecular Mechanisms, Diagnostics, and Future Therapies. Int J Mol Sci. 2025 Aug 18;26(16):7972.
4. McDonald CM. Clinical approach to the diagnostic evaluation of hereditary and acquired neuromuscular diseases. Phys Med Rehabil Clin N Am. 2012 Aug;23(3):495–563.
5. Mukund K, Subramaniam S. Skeletal muscle: A review of molecular structure and function, in health and disease. Wiley Interdiscip Rev Syst Biol Med. 2020 Jan;12(1):e1462.
6. Zumbaugh MD, Johnson SE, Shi TH, Gerrard DE. Molecular and biochemical regulation of skeletal muscle metabolism. J Anim Sci. 2022 Aug 1;100(8):skac035.
7. Gehlert S, Bloch W, Suhr F. Ca2+-dependent regulations and signaling in skeletal muscle: from electro-mechanical coupling to adaptation. Int J Mol Sci. 2015 Jan 5;16(1):1066–95.
8. Kuznetsov AV, Margreiter R, Hagenbuchner J, Ausserlechner MJ. Energy metabolism in different skeletal muscles and muscle fibers: implications for injury and dietary supplementation. Pflugers Arch. 2025 Oct;477(10):1231–40.
9. Sundberg CW, Fitts RH. Bioenergetic basis of skeletal muscle fatigue. Curr Opin Physiol. 2019 Aug;10:118–27.
10. Ziemian M, Szmydtka J, Snoch W, Milner S, Wojciechowski S, Dłuszczakowska A, et al. Integrative Approaches to Myopathies and Muscular Dystrophies: Molecular Mechanisms, Diagnostics, and Future Therapies. Int J Mol Sci. 2025 Aug 18;26(16):7972.
11. Ohlendieck K, Swandulla D. Complexity of skeletal muscle degeneration: multi-systems pathophysiology and organ crosstalk in dystrophinopathy. Pflugers Arch. 2021 Dec;473(12):1813–39.
12. Le Rumeur E. Dystrophin and the two related genetic diseases, Duchenne and Becker muscular dystrophies. Bosn J Basic Med Sci. 2015 Jul 20;15(3):14–20.
13. Szwec S, Kapłucha Z, Chamberlain JS, Konieczny P. Dystrophin- and Utrophin-Based Therapeutic Approaches for Treatment of Duchenne Muscular Dystrophy: A Comparative Review. BioDrugs. 2024 Jan;38(1):95–119.
14. Shakerdi LA. Metabolic Myopathies and HyperCKemia in Adulthood: A Clinical Approach to Diagnosis and Management. J Clin Med. 2026 Mar 9;15(5):2070.
15. Yang YL, Guo L. Cell Death in Skeletal Muscle Diseases: Diverse Roles and Pathological Processes. Cells. 2026 Apr 22;15(9):744.
16. Rodolico C, Bonanno C, Pugliese A, Nicocia G, Benvenga S, Toscano A. Endocrine myopathies: clinical and histopathological features of the major forms. Acta Myol. 2020 Sep 1;39(3):130–5.
17. Dowling P, Gargan S, Swandulla D, Ohlendieck K. Proteomic profiling of impaired excitation-contraction coupling and abnormal calcium handling in muscular dystrophy. Proteomics. 2022 Dec;22(23-24):e2200003.
18. Gumerson JD, Michele DE. The dystrophin-glycoprotein complex in the prevention of muscle damage. J Biomed Biotechnol. 2011;2011:210797.
19. Alghannam AF, Ghaith MM, Alhussain MH. Regulation of Energy Substrate Metabolism in Endurance Exercise. Int J Environ Res Public Health. 2021 May 7;18(9):4963.
20. Muscella A, Stefàno E, Lunetti P, Capobianco L, Marsigliante S. The Regulation of Fat Metabolism During Aerobic Exercise. Biomolecules. 2020 Dec 21;10(12):1699.
21. Liu S, Liu J, Wang Y, Deng F, Deng Z. Oxidative Stress: Signaling Pathways, Biological Functions, and Disease. MedComm (2020). 2025 Jul 1;6(7):e70268.
22. Shi H, Shan Y, Qian K, Zhao R, Li H. Intracellular Calcium Dysregulation: The Hidden Culprit in the Diabetes-Gout Nexus. Biomedicines. 2025 Nov 2;13(11):2694.
23. Gielecińska A, Kciuk M, Kontek R. The Impact of Calcium Overload on Cellular Processes: Exploring Calcicoptosis and Its Therapeutic Potential in Cancer. Int J Mol Sci. 2024 Dec 23;25(24):13727.
24. Hyatt HW, Powers SK. Disturbances in Calcium Homeostasis Promotes Skeletal Muscle Atrophy: Lessons From Ventilator-Induced Diaphragm Wasting. Front Physiol. 2020 Dec 17;11:615351.
25. Tajsharghi H, Oldfors A. Myosinopathies: pathology and mechanisms. Acta Neuropathol. 2013 Jan;125(1):3–18.
26. Arena IG, Pugliese A, Volta S, Toscano A, Musumeci O. Molecular Genetics Overview of Primary Mitochondrial Myopathies. J Clin Med. 2022 Jan 26;11(3):632.
27. Wen H, Deng H, Li B, Chen J, Zhu J, Zhang X, et al. Mitochondrial diseases: from molecular mechanisms to therapeutic advances. Signal Transduct Target Ther. 2025 Jan 10;10(1):9.
28. Hinkle ER, Wiedner HJ, Black AJ, Giudice J. RNA processing in skeletal muscle biology and disease. Transcription. 2019 Feb;10(1):1–20.
29. Verdile V, Guizzo G, Ferrante G, Paronetto MP. RNA Targeting in Inherited Neuromuscular Disorders: Novel Therapeutic Strategies to Counteract Mis-Splicing. Cells. 2021 Oct 22;10(11):2850.
30. Nl S, Shakhatreh Z, Tahir A, Singh J, Sulaiman S, H A, et al. Epigenetic Mechanisms in the Transfer of Metabolic Disorders: A Comprehensive Review. Cureus. 2025 Mar 11;17(3):e80418.
31. Samanta S, Rajasingh S, Cao T, Dawn B, Rajasingh J. Epigenetic dysfunctional diseases and therapy for infection and inflammation. Biochim Biophys Acta Mol Basis Dis. 2017 Feb;1863(2):518–28.
32. Xu X, Pang Y, Fan X. Mitochondria in oxidative stress, inflammation and aging: from mechanisms to therapeutic advances. Signal Transduct Target Ther. 2025 Jun 11;10(1):190.
33. Xu H, Gao Z, Yao X, Sun J, Chen B. The role of cell death in the physiological and pathological processes of skeletal muscle. Front Physiol. 2025 Nov 17;16:1717233.
34. Siu PM, Alway SE. Response and adaptation of skeletal muscle to denervation stress: the role of apoptosis in muscle loss. Front Biosci (Landmark Ed). 2009 Jan 1;14(2):432–52.
35. Guo J, Yang WT, Mai FY, Liang JR, Luo J, Zhou MC, et al. Unravelling oncosis: morphological and molecular insights into a unique cell death pathway. Front Immunol. 2024 Aug 29;15:1450998.
36. Homma H, Tanaka H, Fujita K, Okazawa H. Necrosis Links Neurodegeneration and Neuroinflammation in Neurodegenerative Disease. Int J Mol Sci. 2024 Mar 24;25(7):3636.
37. Gómez-Virgilio L, Silva-Lucero MD, Flores-Morelos DS, Gallardo-Nieto J, Lopez-Toledo G, Abarca-Fernandez AM, et al. Autophagy: A Key Regulator of Homeostasis and Disease: An Overview of Molecular Mechanisms and Modulators. Cells. 2022 Jul 22;11(15):2262.
38. Postolova A, Chen JK, Chung L. Corticosteroids in Myositis and Scleroderma. Rheum Dis Clin North Am. 2016 Feb;42(1):103–18, ix.
39. Ramamoorthy S, Cidlowski JA. Corticosteroids: Mechanisms of Action in Health and Disease. Rheum Dis Clin North Am. 2016 Feb;42(1):15–31, vii.
40. Kawecka K, Theodoulides M, Hasoglu Y, Jarmin S, Kymalainen H, Le-Heron A, et al. Adeno-Associated Virus (AAV) Mediated Dystrophin Gene Transfer Studies and Exon Skipping Strategies for Duchenne Muscular Dystrophy (DMD). Curr Gene Ther. 2015;15(4):395–415.
41. Manini A, Abati E, Nuredini A, Corti S, Comi GP. Adeno-Associated Virus (AAV)-Mediated Gene Therapy for Duchenne Muscular Dystrophy: The Issue of Transgene Persistence. Front Neurol. 2022 Jan 5;12:814174.
42. Zhang Y, Nishiyama T, Olson EN, Bassel-Duby R. CRISPR/Cas correction of muscular dystrophies. Exp Cell Res. 2021 Nov 1;408(1):112844.
43. Kim HK, Lee YS, Sivaprasad U, Malhotra A, Dutta A. Muscle-specific microRNA miR-206 promotes muscle differentiation. J Cell Biol. 2006 Aug 28;174(5):677–87.
44. Brzeszczyńska J, Brzeszczyński F, Hamilton DF, McGregor R, Simpson AHRW. Role of microRNA in muscle regeneration and diseases related to muscle dysfunction in atrophy, cachexia, osteoporosis, and osteoarthritis. Bone Joint Res. 2020 Nov;9(11):798–807.
45. Yoon MS. mTOR as a Key Regulator in Maintaining Skeletal Muscle Mass. Front Physiol. 2017 Oct 17;8:788.
46. Bartoli M, Bailey RM, Meyer K, Barthélémy F. Editorial: Personalized medicine for neuromuscular disorders. Front Cell Dev Biol. 2023 Nov 16;11:1329048.
47. Khan SN, Danishuddin, Khan MWA, Guarnera L, Akhtar SMF. Multi-modal AI in precision medicine: integrating genomics, imaging, and EHR data for clinical insights. Front Artif Intell. 2026 Jan 7;8:1743921.
48. Gwaza G, Plüddemann A, McCall M, Heneghan C. Integrated Diagnosis in Africa's Low- and Middle-Income Countries: What Is It, What Works, and for Whom? A Realist Synthesis. Int J Integr Care. 2024 Sep 12;24(3):20.
49. Francisco KKY, Apuhin AEC, Maravilla NMAT, Byers MC, Karim HA, Tan MJT, et al. Personalized medicine and health equity: overcoming cost barriers and ethical challenges. Int J Equity Health. 2025 Dec 7;25(1):4.