Abstract
Background: Bile duct injury (BDI) is one of the most serious complications of cholecystectomy associated with substantial risk of morbidity and mortality. Although surgical techniques have evolved, bile duct injuries continue to occur with notable frequency.
Aim: To evaluate the demographic profile, presentation, classification, management, and outcomes of patients with BDI following laparoscopic cholecystectomy.
Methods: A dual center prospective study was conducted from June 2022 to June 2024 at Jawaharlal Nehru Medical College, Aligarh and Sir Ganga Ram Hospital, New Delhi. Sixty patients with post laparoscopic cholecystectomy BDI were included. Data were collected on demographic profile, clinical features at presentation, Strasberg–Bismuth classification, management, post operative complications and overall outcome at six months.
Results: The mean age was 38.1 years with female predominance (F:M ratio 2.3:1). Common symptoms were abdominal pain (81.7%) and jaundice (73.3%). Injuries were most frequently Strasberg class E4 (25%) and E2 (23.3%), followed by class A (23.3%). Hepaticojejunostomy was performed in 75% of patients, ERCP with sphincterotomy in 16.7% (two failures) and 8.3% were managed conservatively. At six months, 93.3% of patients improved, while overall mortality occurred in 6.7% (n=4). Early postoperative symptoms including pain and icterus showed steady resolution, and most patients had satisfactory recovery.
Conclusion: BDI continues to challenge surgeons in the laparoscopic era, with complex injuries often managed at specialized centers. Hepaticojejunostomy remains the cornerstone of management for high-grade injuries, while ERCP offers effective minimally invasive approach for biliary leaks. Early recognition, accurate classification, and specialized multidisciplinary care are critical for optimizing outcomes and minimizing long-term complications.
Keywords
Bile duct Injury, Cholecystectomy, Strasberg classification, Hepaticojejunostomy, ERCP
Introduction
Post-cholecystectomy bile duct injury (BDI) remains a critical postoperative complication because of its considerable morbidity and mortality [1,2]. The incidence of BDI is closely linked to the surgeon's experience and expertise. BDI is notably higher following laparoscopic cholecystectomy (LC) compared to open cholecystectomy (OC), with rates of 0.4–0.6% for LC versus 0.1–0.2% for OC [3,4]. which has significantly reduced owing to advancements in surgical technique and laparoscopic experience [5]. The classification of bile duct injuries using the Bismuth-Strasberg system based on the location within the biliary tract, aid in diagnosis and planning further management. Morbidities resulting from bile duct injury, such as biliary fistula, jaundice, and bile duct stenosis, not only affect patients' long-term prognosis but also impose substantial medical burdens, significantly impacting quality of life [6].
Preventing bile duct injury (BDI) is crucial step from the surgeon's perspective. Effective prevention strategies involve a deep understanding of how BDIs occur, recognizing the critical view of safety, and making appropriate patient selections [7–9].
Early identification of BDI is vital in reducing major morbidity, especially in patients exhibiting an unusual postoperative course after cholecystectomy. Various diagnostic tools, include intraoperative cholangiogram, intraoperative ultrasound or indocyanine green fluorescence cholangiography and postoperative imaging modalities such as Endoscopic Retrograde Cholangiopancreatography (ERCP), Magnetic Resonance Cholangiopancreatography (MRCP), Contrast enhanced CT, and Percutaneous Transhepatic Cholangiography (PTC) are used to detect BDIs.
Despite advancements in surgical safety and diagnostic modalities, bile duct injury continues to carry significant long-term consequences. Outcomes largely depend on the timing of recognition, the extent of ductal damage and the expertise of the surgical team. Delayed or inappropriate management may lead to recurrent cholangitis, secondary biliary cirrhosis, portal hypertension, and even liver failure. Thus, timely recognition and specialized surgical reconstruction can restore satisfactory biliary drainage and improve prognosis. This study underscores the importance of early detection and multidisciplinary management in optimizing patient survival and quality of life.
The primary objectives were to analyze the demographic profile of patients with BDI, evaluate the clinical spectrum of presentations such as abdominal pain, abdominal distension, jaundice, and bile leak through drain, classify injuries according to the Strasberg–Bismuth classification and assess the treatment modalities employed.
The secondary objective was to study postoperative complications and overall outcome following repair of BDIs up to six months after the procedure, including bile leak or fistula, cholangitis, stricture/stenosis and mortality.
Material and Methods
This prospective dual-centric study was conducted over a period of two years from June 2022 to June 2024. A total of 60 patients who sustained bile duct injury (BDI) following cholecystectomy were included in the study. Ethical clearance was granted by the institutional board and written informed consent was obtained from all patients after explaining the voluntary nature of participation and strict confidentiality of patient data. Patients aged more than 14 years with bile duct injuries related to cholecystectomy who provided informed consent were enrolled in the study and patients with bleeding diathesis and bile duct injury not related to cholecystectomy were excluded.
Clinical features such as abdominal pain, distension, jaundice, bile leak, and fever at the time of presentation were recorded. Complete blood count (CBC), renal function tests, serum electrolytes and imaging studies such as ultrasound, MRCP were done in all the patients and CT scan, ERCP, PTC and per operative cholangiogram were done as indicated.
|
S. No. |
Procedure |
No. of Cases (n=60) |
|
1 |
Ultrasound Whole Abdomen |
60 (100 %) |
|
2 |
MRCP |
60 (100%) |
|
3 |
CECT Whole Abdomen |
18 (30%) |
|
4 |
PTC |
2 (3.3%) |
|
5 |
Per-Operative Cholangiogram |
5 (8.3%) |
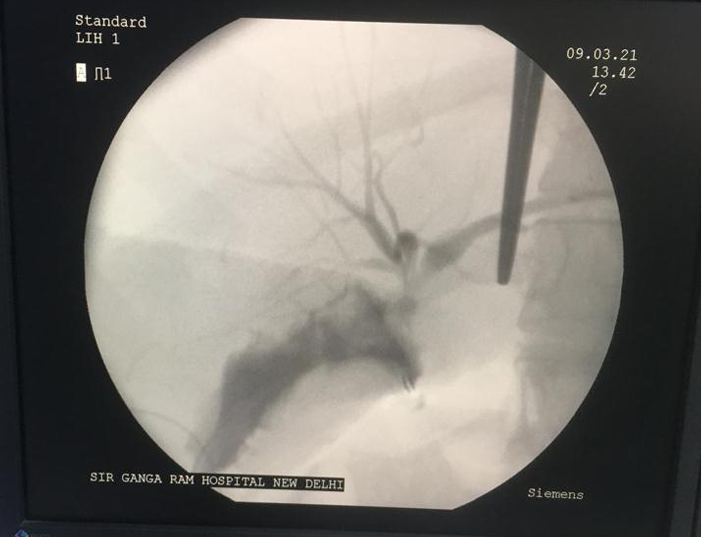
Figure 1. Illustration showing intraoperative cholangiogram delineating the anatomy.

Figure 2. Illustration showing magnetic resonance cholangiopancreatography delineating type E4 biliary structure. a. Coronal T2 weighted,
b. 3d maximum intensity projection, c. Axial T2 weighted.
Management principles
1. Infection Control, limiting inflammation
- Parenteral antibiotics
- Percutaneous drainage of periportal fluid collections
2. Clear and thorough delineation of entire biliary anatomy
- Magnetic resonance cholangiopancreatography within 3–7 days if the patient was stable and bile leak was suspected soon after surgery (within few days); wait 7–10 days with ongoing sepsis, peritonitis. If no ongoing bile leak, injury suspected or missed intraoperatively then done 2–3 weeks of the index surgery [10,11].
- Percutaneous transhepatic cholangiography (especially when MRCP is inconclusive)
- Endoscopic retrograde cholangiopancreatography (especially if cystic duct stump leak is suspected).
3. Reestablishment of biliary-enteric continuity
- Tension-free, mucosa-to-mucosa anastomosis
- Roux-en-Y hepaticojejunostomy
- Long-term trans anastomotic stents if bifurcation or higher is involved.
Injury classification
Bile duct injuries will be classified according to the Strasberg Bismuth classification system [10]. This system categorizes bile duct injuries based on their anatomical location relative to the biliary confluence:
- Type A: Leak from the cystic duct or small ducts in the gallbladder or liver bed.
- Type B: Occlusion of an aberrant right hepatic duct.
- Type C: Transection of an aberrant right hepatic duct with leakage.
- Type D: Injury to the lateral bile duct involving less than 50% of its circumference.
- Type E: CBD injury with circumference involving more the 50 % of its circumference and strictures in the hepatic ducts, further divided based on the proximal extent (E1, E2, E3, E4, E5).
- E1 (distal): Injury to CBD ≥2 cm from confluence.
- E2 (proximal): Injury to CBD <2 cm from confluence.
- E3: Injury at confluence with intact confluence.
- E4: Injury at confluence with obliteration of confluence.
- E5: Type C with concomitant CHD injury.
Intervention according to type of injury [10–12]
|
Type of Injury |
Intervention |
|
Type A |
ERCP with sphincterotomy, Hepaticojejunostomy, Conservative |
|
Type B |
Surgical (Segmental Drainage, Hepaticojejunostomy) |
|
Type C |
Surgical (Segmental Drainage, Hepaticojejunostomy) |
|
Type D |
ERCP with sphincterotomy + Stent (if Partial), Hepaticojejunostomy (if major) |
|
Type E |
Hepaticojejunostomy |
Data collection and analysis
Data were collected prospectively using a structured proforma, which included demographic details, clinical presentation, type and classification of bile duct injury, treatment modality, and postoperative outcomes. Patients were followed for a period of six months to document complications. Data were entered into Microsoft Excel and analyzed using SPSS software (version 28). Continuous variables were expressed as mean ± standard deviation (SD), while categorical variables were presented as frequencies and percentages. Comparative analysis between categorical variables was performed using the Chi-square test or Fisher’s exact test as appropriate, and continuous variables were compared using the student’s t-test. A p-value of <0.05 was considered statistically significant.
Results
Patient demographics and pre-operative data
Total of 60 patients with bile duct injury (BDI) following cholecystectomy were included in the study. The mean age of the study population was 38.13 ± 11.96 years. The largest proportion of patients was observed in the 31–40 years age group (22 cases, 36.7%), followed by the 21–30 years group (17 cases, 28.3%). Regarding sex distribution, females predominated with 42 cases (70.0%), whereas males accounted for 18 cases (30.0%), giving a female-to-male ratio of 2.33:1. The combined age and sex distribution is presented in Table 1.
|
Age Group (years) |
Male (n=18, 30%) |
Female (n=42, 70%) |
p-value |
|
≤ 20 |
1 (1.7%) |
0 (0%) |
0.300 |
|
21–30 |
6 (10.0%) |
11 (18.3%) |
0.755 |
|
31–40 |
5 (8.3%) |
17 (28.3%) |
0.396 |
|
41–50 |
3 (5.0%) |
5 (8.3%) |
0.686 |
|
51–60 |
2 (3.3%) |
7 (11.7%) |
0.710 |
|
61–70 |
1 (1.7%) |
2 (3.3%) |
1.00 |
Clinical features
Out of 60 cases pain in abdomen in 49 cases (81.7%) and icterus in 44 cases (73.3%) were the most frequent presenting symptom. Abdominal distension was present in 32 cases (53.3%), fever in 33 cases (55.0%) and significant drain output in 30 cases (50%) respectively as shown in Table 2.
|
S. No |
Primary Clinical Feature |
Cases (n=60) |
P value |
|
1 |
Pain in Abdomen |
49 (81.7%) |
<0.001 |
|
2 |
Abdominal Distension |
32 (53.3% |
<0.001 |
|
3 |
Icterus |
44 (73.3%) |
<0.001 |
|
4 |
Drain output |
30 (50.0%) |
<0.001 |
|
5 |
Fever |
33 (55.0%) |
<0.001 |
Classification of bile duct injury
The most common categories are A and E2, each accounting for 23.3% of the cases, while E4 is the most prevalent classification, representing 25.0% of the total. Categories C and D each have 3.3% respectively, indicating minimal representation. E1 and E3 include 8.3% and 11.7% of the cases, respectively, and E5 has the smallest proportion at 1.7%. Class B had no patient as depicted in Table 3.
|
S. No. |
Classification |
Cases (n=60) |
p-value |
|
1 |
A |
14 (23.3%) |
0.017 |
|
2 |
C |
2 (3.3%) |
0.029 |
|
3 |
D |
2 (3.3%) |
0.029 |
|
4 |
E1 |
5 (8.3%) |
0.434 |
|
5 |
E2 |
14 (23.3%) |
0.017 |
|
6 |
E3 |
7 (11.7%) |
1.0 |
|
7 |
E4 |
15 (25.0%) |
0.009 |
|
8 |
E5 |
1 (1.7%) |
0.005 |
Distribution of interventions
Various interventions were carried out in the study population. Most patients (45 cases, 75%) underwent hepaticojejunostomy. ERCP with sphincterotomy was performed in 10 cases (16.7%) with failed ERCP in 2 patients (3.3%) and 5 cases (8.33%) were managed conservatively as mentioned in Table 4.
|
S. No. |
Intervention |
Cases (n=60) |
p-value |
|
1 |
Hepaticojejunostomy |
45 (75.0%) |
<0.001 |
|
2 |
ERCP with Sphincterotomy |
10 (16.7%) |
0.006 |
|
3 |
Conservative Management |
5 (8.3%) |
<0.001 |
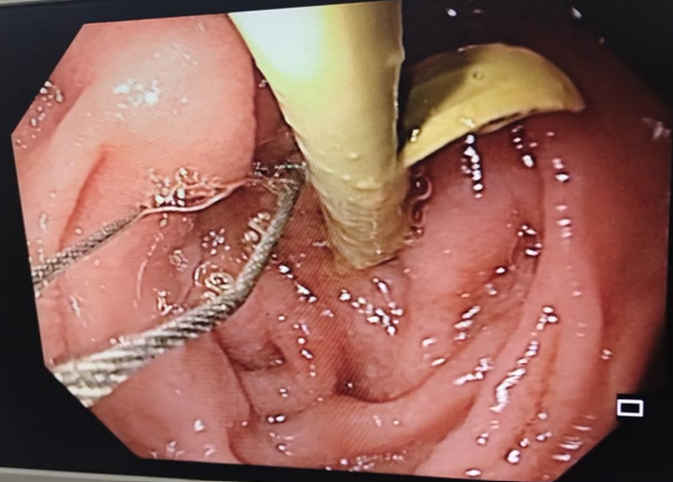
Figure 3. Illustration showing endoscopic retrograde cholangiopancreatography with common bile duct stent in-situ.
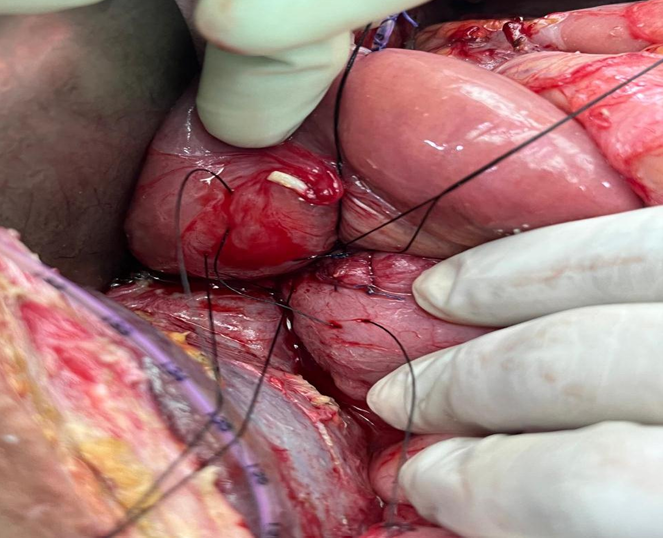
Figure 4. Illustration showing Roux-en y Hepatico-Jejunostomy with stay sutures using silk-2-0 round body.
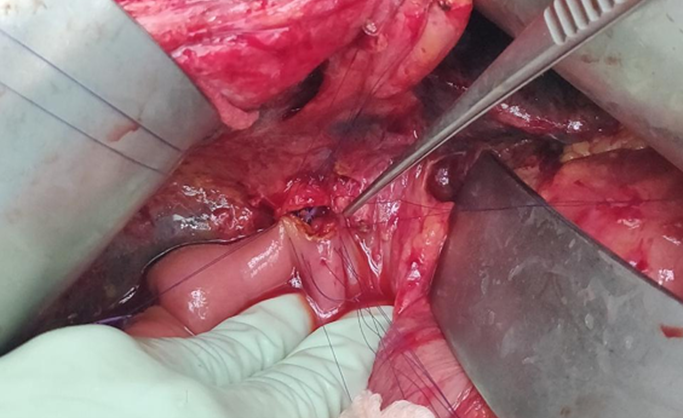
Figure 5. Illustration showing Roux-en y Hepatico-Jejunostomy anastomosis done using Vicryl 3-0 round body.
Distribution of interventions based on BDI classification
The most common intervention was hepaticojejunostomy, performed in 75.0% of cases, predominantly for class E4 (25.0%), E2 (23.3%) and E3 (11.7%). ERCP with sphincterotomy was used in 16.7% of cases, mainly for class C (11.7%). Conservative management was employed in 8.3% of cases, with the majority in classification A (8.3%) as shown in Table 5.
|
Classification |
Hepaticojejunostomy |
ERCP with Sphincterotomy |
Conservative Management |
Total |
p-value |
Fisher Exact p value |
|
Cases (n=45) |
Cases (n=10) |
Cases (n=5) |
Cases (n=60) |
|
|
|
|
A |
2 (3.3%) |
7 (11.7%) |
5 (8.3%) |
14 (23.3%) |
<0.001 |
<0.001 |
|
C |
1 (1.7%) |
1 (1.7%) |
0 (0.0%) |
2 (3.3%) |
0.422 |
0.441 |
|
D |
0 (0.0%) |
2 (3.3%) |
0 (0.0%) |
2 (3.3%) |
0.006 |
0.059 |
|
E1 |
5 (8.3%) |
0 (0.0%) |
0 (0.0%) |
5 (8.3%) |
0.403 |
0.318 |
|
E2 |
14 (23.3%) |
0 (0.0%) |
0 (0.0%) |
14 (23.3%) |
0.048 |
0.013 |
|
E3 |
7 (11.7%) |
0 (0.0%) |
0 (0.0%) |
7 (1.7%) |
- |
- |
|
E4 |
15 (25.0%) |
0 (0.0%) |
0 (0.0%) |
15 (25.0%) |
- |
- |
|
E5 |
1 (1.7%) |
0 (0.0%) |
0 (0.0%) |
1 (1.7%) |
- |
- |
Temporal distribution of cases on the basis of time of injury and time of intervention
In our study majority intervention occurred after 6 weeks in 58% (32 cases) between 2–6 weeks in 38% (21 cases) and within 2 weeks in 4% (2 cases) (Table 6).
|
S. No. |
Duration From Injury (weeks) |
No. of Cases (n=55) |
(%) |
p-value |
|
1 |
<2 weeks |
2 |
3.6% |
<0.001 |
|
2 |
2–6 weeks |
21 |
38.0% |
0.475 |
|
3 |
>6 weeks |
32 |
58.0% |
<0.001 |
Follow up and outcomes (Table 7)
|
Parameter |
Pre-intervention (Mean ± SD) |
Post-intervention (Mean ± SD) |
t-value |
p-value |
Interpretation |
|
TLC (cells/μL) |
11,575.25 ± 5,374.88 |
8,963.28 ± 2,819.43 |
3.853 |
< 0.001 |
Significant reduction |
|
Total Bilirubin (mg/dL) |
5.22 ± 6.50 |
2.17 ± 1.93 |
4.164 |
< 0.001 |
Significant reduction |
|
Total Bilirubin (with icterus) |
6.72 ± 6.70 |
2.55 ± 2.10 |
— |
0.002 / 0.013* |
Significant reduction |
|
Direct Bilirubin (mg/dL) |
4.42 ± 5.97 |
1.66 ± 1.42 |
3.796 |
< 0.001 |
Significant reduction |
|
Direct Bilirubin (with icterus) |
5.83 ± 6.24 |
1.99 ± 1.50 |
3.180 |
0.002 |
Significant reduction |
|
Alkaline Phosphatase (U/L) |
486.72 ± 502.32 |
332.62 ± 285.43 |
2.349 |
0.023 |
Significant reduction |
|
ALP (with icterus) |
530.68 ± 534.51 |
350.05 ± 297.80 |
— |
— |
Significant reduction |
|
ALP (without icterus) |
357.50 ± 320.26 |
279.00 ± 246.34 |
— |
— |
Reduction (non-significant trend) |
TLC count
Leucocyte count decreased significantly following intervention from 11,575.25 ± 5,374.88 to 8,963.28 ± 2,819.43 cells/μL (t=3.853, p<0.001).
Total bilirubin
Total bilirubin (TB) levels decreased significantly after intervention from 5.22 ± 6.50 mg/dL, to 2.17 ± 1.93 mg/dl. (t=4.164, p-value <0.001).
Total bilirubin levels in patients with icterus
Total bilirubin (TB) levels significantly decreased in patients with icterus, from 6.72 ± 6.70 mg/dL to 2.55 ± 2.10 mg/dL (p-value =0.002 pre, 0.013 post).
Direct bilirubin
The mean DB level before the intervention was 4.42 ± 5.97 mg/dL, which decreased significantly to 1.66 ± 1.42 mg/dL post-intervention (t= 3.796, p=0.001).
Direct bilirubin levels in patients with icterus
For patients with icterus, the mean DB level significantly decreased from 5.83 ± 6.24 mg/dL before intervention to 1.99 ± 1.50 mg/dL after intervention. (t= 3.180 and a p<0.002).
Alkaline phosphatase (ALP)
The mean ALP level before the intervention was 486.72 ± 502.32 U/L, which decreased to 332.62 ± 285.43 U/L. (t= 2.349, p< 0.023).
Alkaline phosphatase (alp) in patients with icterus
For patients with icterus, the pre-intervention ALP mean was 530.68 ± 534.51, which decreased to 350.05 ± 297.80. In contrast, patients without icterus had a pre intervention ALP mean of 357.50 ± 320.26, reducing to 279.00 ± 246.34.
Outcome according to Strasberg-Bismuth classification
Our study revealed significant variation in outcomes across different classifications. The majority of patients classified as A (23.3%) and E2 (23.3%) showed improvement, with no mortality reported in these groups. Classifications C, D, and E1 had limited cases, with only one mortality in E5 and no other outcomes reported. The E4 classification had a considerable number of patients improving (18.3%) but also reported three mortalities (5.0%) (Table 8).
|
Classification |
Improved (n=56) |
Mortality (n=4) |
P-value |
|
A |
14 (23.3%) |
0 (0.0%) |
0.564 |
|
C |
2 (3.3%) |
0 (0.0%) |
1.0 |
|
D |
2 (3.3%) |
0 (0.0%) |
1.0 |
|
E1 |
5 (8.3%) |
0 (0.0%) |
1.0 |
|
E2 |
14 (23.3%) |
0 (0.0%) |
0.564 |
|
E3 |
7 (11.7%) |
0 (0.0%) |
1.0 |
|
E4 |
12 (20.0%) |
3 (5.0%) |
0.044 |
|
E5 |
0 (0.0%) |
1 (1.7%) |
0.066 |
Overall outcome
Table 9 presents the outcomes for the study population, with 93.3% of cases showing improvement. Only 5% of cases required referral to a higher center, while 6.7% resulted in mortality.
|
S. No. |
Outcome |
No. of Cases |
p-value |
|
1 |
Improved |
56 (93.33%) |
<0.001 |
|
2 |
Mortality |
4 (6.66%) |
<0.001 |
|
Case No. |
Age / Sex |
Strasberg–Bismuth Classification |
Timing of Repair (post-injury) |
Preoperative Findings |
Type of Intervention |
Postoperative Course / Complications |
Probable Cause of Mortality |
|
1 |
45 /F |
E4 |
Late (>6 weeks) |
Obstructive jaundice, cholangitis |
Hepaticojejunostomy |
Persistent bile leak, sepsis, multiorgan failure |
Postoperative sepsis due to anastomotic leak |
|
2 |
52 /M |
E5 |
Early (<2 weeks) |
Bile peritonitis, high bilirubin |
Hepaticojejunostomy + stenting |
Uncontrolled infection, septic shock |
Repair performed during sepsis leading to septic shock |
|
3 |
60 /F |
E4 |
Delayed (3–4 weeks) |
Elevated bilirubin, hepatic dysfunction |
Hepaticojejunostomy |
Post-op bleeding, transfusion, hepatic failure |
Liver failure secondary to prolonged cholestasis |
|
4 |
40 /M |
E4 |
Late (>6 weeks) |
No sepsis, previous ERCP attempt |
Revision Hepaticojejunostomy |
Bile leak, secondary peritonitis |
Anastomotic leak with bile peritonitis |
|
Outcome / Complication |
No. of Patients (n) |
Percentage (%) |
Remarks / Clinical Course |
|
Improved Outcome |
56 |
93.3% |
Uneventful recovery with progressive normalization of liver function tests and resolution of jaundice. |
|
Bile Leak / External Fistula |
5 |
8.3% |
Minor controlled bile leak through drain in 3 cases; 2 required re-exploration. All resolved with conservative management except one mortality due to sepsis. |
|
Cholangitis |
6 |
10.0% |
Managed conservatively with IV antibiotics and biliary drainage; no residual stricture at 6 months. |
|
Stricture / Anastomotic Stenosis |
4 |
6.7% |
Diagnosed on imaging during follow-up (MRCP/ERCP); 2 managed with balloon dilatation, 2 required re-operation. |
|
Biliary Peritonitis |
3 |
5.0% |
Following anastomotic leak; all required re-exploration; contributed to 2 mortalities. |
|
Wound Infection / Superficial SSI |
7 |
11.7% |
Responded to local care and antibiotics; no long-term sequelae. |
|
Intra-abdominal Abscess |
2 |
3.3% |
Managed by percutaneous drainage under USG guidance. |
|
Mortality |
4 |
6.7% |
Causes included sepsis due to bile leak (n = 2), hepatic failure (n = 1), and biliary peritonitis (n = 1). |
|
Total Patients Followed Up |
60 |
100.0% |
Minimum follow-up: 6 months. No recurrence or late stricture in remaining cases. |
Discussion
In our study overall improvement was observed in 93% of cases, underscoring the effectiveness of current surgical strategies with 6.7% mortality rate. Our observations contribute to understanding intervention efficacy and emerging trends in the management of bile duct injuries.
Age distribution
In our study the mean age of study population was 38.13 years. The majority of cases, 22 cases (36.7%) were in the 31–40 years range, followed by 17 (28.3%) cases in the 21–30 years range. Our findings are in concordance with the study conducted by Zidan et al. [13] which showed mean age 37.97 years. Similarly to our study, Çavuşoğlu et al. [14], study showed mean age of bile duct injury patients to be 51.1 years. Ma et al. [15] in their study also showed similar age predilection with mean age of 49.9 years.
Sex distribution
The sex distribution in our study reveals that 42 (70%) out of 60 cases were females and 18 (30%) were males with female to male ratio 2.33:1. Study conducted by Ray et al. [16] showed similar results with 179 (78.5%) patients out of 261 being females and (21.5%) 49 patients being males. Jain et al. [17] conducted systemic review whose results are in concordance with our study—it showed 94 (73.4%) patients out of 128 patients were females and 34 (26.6%) were males. Geers [18] showed that 13 (61.9%) out of 21 patients of bile duct injury were females and 8 patients (38%) were males. These findings are also similar to our results.
Clinical features
In our study, 49 (81.7%) patients out of 60 had abdominal pain as the most prevalent symptom, icterus was present in 44 (73.3%) patients and fever in 33 (55%) cases. Abdominal distension was present in 32 (53.3%) patients while bile leak was present in 30 (50%) patients. Carannante [19] showed patients of bile duct injury presented with similar clinical features, pain in abdomen was present in 81 (93.1%) out of 87 cases, fever was present in 65 (74.7%) and jaundice was present in 59 (67.8%) participants. Bile leak was present in 75 patients (92%) out of 81 patients. Pandit et al. [20] showed jaundice was present in 5 patients (29.4%) out of 18 patients of BDIs. Ahmad et al. [21] showed out of 32 patients of BDIs, 20 patients (64%) had jaundice, 19 patients (59%) had bile leak, 24 patients (75%) had abdominal pain, 15 patients (47%) had fever, and 14 patients (45%) had abdominal distension. Similar trends were observed in our study.
PTC procedure outcome
Percutaneous Transhepatic Cholangiography (PTC) was performed in 2 patients out of 60 patients (3.3%). This reflects the general trend in literature, where PTC is often reserved for more complex or challenging cases that are not amenable to ERCP. Stilling et al. [22] suggests that PTC is typically used as a secondary option, particularly in cases where ERCP is not feasible or has failed. In their study 6.04% of patients underwent PTC. Our limited use of PTC aligns with the experiences from Pottakkat et al. [23] where PTC was used in specific clinical scenarios, often involving more intricate or high-risk procedures. They observed that 5.2% underwent PTC. This low usage rate suggests that PTC is primarily a fallback option, utilized when other less invasive methods are insufficient. The preference for less invasive techniques, such as ERCP, is likely due to their lower complication rates and the ability to manage a wider range of BDI-related issues without the need for more invasive procedures.
Per-operative cholangiogram
Per operative cholangiogram was performed in 5 (8.3%) patients out of 60 in our study. This selective application is consistent with recommendations by Pesce et al. [24] and Giger et al. [25] who discussed the tailored use of intraoperative imaging techniques based on the specific type and severity of the bile duct injury. In their study, 8% of patients also underwent per operative cholangiogram. The infrequent use of per operative cholangiogram also reflects a broader trend in surgical practice, that it was performed when there was difficulty in delineating anatomy per operatively at the time of bile duct injury repair.
Bile duct injury classification
In our study we utilized the Strasberg classification system to categorize bile duct injuries, reveals most common class was type E4, it was observed in 15 (25.0%) patients out of 60. Type A and type E2 were second most common classes, each having 14 (23.3%) patients. Class E3 has 7 (11.7%) patients, Class E1 has 5 (8.3%) patients, and Class C and D have two patients each (3.3% in each class). Class E5 has 1 (1.7%) patient. There was no case of class B reported in our study. In the study by Pandit et al. (2020) [20], type A injury was present in 9 (50%) out of 18 patients, type D was present in 1 (5.5%), type E1 injury was present in 5 patients (27.8%), type E2 injury was present in 1 (5.5%) and 2 (11.1%) patients showed type E3 injuries. Similarly, Malla et al. [26] showed that out of 35 cases of BDIs, type A injuries were present in 27 cases (77.14%), type E1 in 3 cases (8.57%), type E2 injuries in 3 cases (8.57%) and type E3 was present in 2 cases (5.71%). Ray et al. [16] showed that out of 228 patients, type E1 injuries were present in 13 patients (5.7%), type E2 injury were present in 68 patients (29.82%), type E3 injuries were present in 108 patients (47.36%), type E4 injuries were present in 28 patients (12.28%) and type E5 injuries were present in 11 patients (4.82%). This pattern parallels findings of our study except for higher incidence of E4 injuries in our study. This may be because of the fact that our institute is a tertiary referral center so the patients of Type A injury may have been managed at primary or secondary level but only more complex injuries like E4 are being referred.
Intervention
Hepaticojejunostomy
In our study, 45 patients out of 60 patients (75%) underwent hepaticojejunostomy. Zidan et al. [13] showed 17 (48.6%) out 35 BDIs patients underwent hepaticojejunostomy. Çavuşoğlu et al. [14] showed that 27 (32.6%) out of 83 patients of BDIs underwent hepaticojejunostomy. Vu et al. [27] showed that hepaticojejunostomy was performed in 12 (42.9%) out of 28 patients of BDIs. This predominance likely reflects referral bias, as complex E4 injuries are typically managed in tertiary centers.
ERCP with sphincterotomy
In our study, ERCP with sphincterotomy was performed in 10 (16.6%) cases out of 60 patients. ERCP failed in 2 patients (3.3%). This corroborates with the findings of the study done by Vu et al. [27] that showed ERCP with stenting was done in 6 patients (21.4%) out of 28 patients.
Conservative management
Five (8.3%) patients out of 60 patients were managed conservatively. Vu et al. [27] showed similar results where conservative management was done in two patients (7.1%) out of 28 patients. Carannante et al. [19] also showed that 19 (10.5%) out of 180 patients of BDIs were managed conservatively. These findings are consistent with our study.
Outcomes
Our study demonstrated an overall improvement rate of 93%, reflecting the effectiveness of current surgical management strategies, while the observed mortality rate was 6.7%. This aligns with findings from Schmidt et al. [28] who reported high success rates for hepaticojejunostomy. However, the mortality rate highlights challenges and potential complications associated with severe bile duct injuries. Our study's outcomes are consistent with Barrett et al. [29] who reported varying morbidity rates but reflected on the overall effectiveness of interventions. The mortality rate in our study reflects the inherent difficulties in managing severe cases.
Follow-up assessments
Postoperative morbidity primarily involved wound infection (~12%), cholangitis (10%) and controlled bile leak (8%). Biliary strictures developed in 4 patients (6.7%) during follow-up, two of whom underwent successful balloon dilatation, and two required surgical revision. Intra-abdominal abscesses occurred in 3.3% of cases and were managed by USG guided drainage. These percentages in our study correspond with previously reported ranges by de Reuver et al. [11], Schreuder et al. [30] and Ahmad et al. [31]. The resolution of symptoms underscores the success of the treatment strategies employed, consistent with the follow-up outcomes reported by Pottakkat et al. [21], which emphasized the importance of ongoing assessment, meticulous surgical reconstruction, infection control, and structured follow-up are crucial in improving long-term outcomes and minimizing late biliary complications in patients undergoing repair of bile duct injuries.
Conclusion
This study identified key trends across demographic, clinical, and procedural outcomes among patients with bile-duct injury: 1. Majority of patients were females with Female to male ratio was 2.33:1. 2. Abdominal pain was the most predominant presenting complaint 49 (81.7%). 3. Most common type of bile duct injury was Strasberg class E4 in 15 (25%) cases. 4. Hepaticojejunostomy done in 45 (75%) cases was the most common intervention, leading to an overall improvement in the majority of cases. 5. Mortality was limited to 4 patients (6.7%) out of 60 cases. 6. During follow up, symptoms like pain, distension and jaundice are resolved, indicating effectiveness of the interventions. 7. Follow-up data highlights the continued resolution and improved overall outcome thus affirming the overall success and safety of the interventions. Future studies should focus on multicenter prospective data, optimal timing of repair, evaluation of standardized and minimally invasive management strategies, and long-term follow-up assessing late biliary complications and quality-of-life outcomes.
Strengths and Limitations
This prospective dual-center study reduces recall bias and reflects real-world referral patterns of complex bile duct injuries. Use of standardized Strasberg–Bismuth classification, structured multidisciplinary management, objective biochemical outcome measures, and complete six-month follow-up strengthen clinical validity. However, the small sample size and tertiary-care setting introduce referral bias and limit generalizability. The short follow-up may not capture late biliary complications, and the absence of a comparative control group restricts inference regarding optimal timing and technique of repair.
References
2. Strasberg SM, Hertl M, Soper NJ. An analysis of the problem of biliary injury during laparoscopic cholecystectomy. J Am Coll Surg. 1995;180(1):101–25.
3. Connor S, Garden OJ. Bile duct injury in the era of laparoscopic cholecystectomy. Br J Surg. 2006;93(2):158–68.
4. Flum DR, Cheadle A, Prela C, Dellinger EP, Chan L. Bile duct injury during cholecystectomy and survival in Medicare beneficiaries. JAMA. 2003;290(16):2168–73.
5. Archer SB, Brown DW, Smith CD, Branum GD, Hunter JG. Bile duct injury during laparoscopic cholecystectomy: Results of a national survey. Ann Surg. 2001;234(4):549–58.
6. Stewart L, Way LW. Bile duct injuries during laparoscopic cholecystectomy. Factors that influence the results of treatment. Arch Surg. 1995;130(10):1123–8.
7. Strasberg SM, Brunt LM. The critical view of safety: A means of avoiding bile duct injury during laparoscopic cholecystectomy. J Am Coll Surg. 2010;211(1):132–8.
8. Gupta V, Jain G. Safe laparoscopic cholecystectomy: Adoption of universal culture of safety in cholecystectomy. World J Gastrointest Surg. 2019;11(2):62–84.
9. Booij KA, de Reuver PR, Yap K, van Dieren S, van Delden OM, Rauws EA, Busch OR, van Gulik TM. Morbidity and mortality after bile duct injury: 27-year experience in a tertiary referral center. Ann Surg. 2018;268(1):143–50.
10. Strasberg SM, Hertl M, Soper NJ. An analysis of the problem of biliary injury during laparoscopic cholecystectomy. J Am Coll Surg. 1995 Jan;180(1):101–25.
11. de Reuver PR, Grossmann I, Busch ORC, Obertop H, van Gulik TM, Gouma DJ. Referral pattern and timing of repair are risk factors for complications after reconstructive surgery for bile duct injury. Ann Surg. 2007;245(5):763–70.
12. de’Angelis N, Catena F, Memeo R, Coccolini F, Martínez-Pérez A, Romeo O, et al. 2020 WSES guidelines for the detection and management of bile duct injury during cholecystectomy. World J Emerg Surg. 2021;16(1):30.
13. Zidan MHE, Abdelhady M, Elrazek AE, et al. Surgical management and outcomes of post-cholecystectomy bile duct injury: A tertiary center experience. Ann Hepatobiliary Pancreat Surg. 2024;28(1):42–9.
14. Çavuşoğlu SD, Doğan U, Eray IC, et al. Bile duct injuries following cholecystectomy: Clinical presentation, management, and long-term outcomes. Turk J Surg. 2020;36(3):276–2.
15. Ma D, Yang F, Jin C, et al. Bile duct injury after laparoscopic cholecystectomy: Clinical features, treatment, and long-term outcomes. Surg Endosc. 2021;35(8):4440–8.
16. Ray S, Sanyal S, Das S, Jana K, Das AK, Khamrui S. Outcomes of surgery for post-cholecystectomy bile duct injuries: an audit from a tertiary referral centre. J Visc Surg. 2020 Feb;157(1):3–11.
17. Jain D, Malage S, Singh A, Ghosh N, Rahul R, Sharma S, et al. Post Cholecystectomy Bile Duct Injury in an Acute Setting: Categorization, Triaging, and Management Algorithm. Cureus. 2024 Mar 8;16(3):e55828.
18. Geers J, Jaekers J, Topal H, Collignon A, Topal B. Bile duct injury in laparoscopic cholecystectomy with a posterior infundibular approach. Int J Hepatobiliary Pancreat Dis. 2022;12(2):13–21.
19. Carannante F, Mazzotta E, Miacci V, Bianco G, Mascianà G, D'Agostino F, et al. Identification and management of subvesical bile duct leakage after laparoscopic cholecystectomy: A systematic review. Asian J Surg. 2023 Oct;46(10):4161–8.
20. Pandit N, Sharma A, et al. Current scenario of post-cholecystectomy bile leak and bile duct injury at a tertiary care referral centre of Nepal. Minim Invasive Surg. 2020 Apr; 2020:4382307.
21. Ahmad U, Jan Y, Uzair M. Clinical presentation, types and treatment outcomes of bile duct injuries (BDI) in laparoscopic cholecystectomy. TPMJ. 2020;27(2):293–9.
22. Stilling NM, Fristrup C, Wettergren A, Ugianskis A, Nygaard J, Holte K, et al. Long-term outcome after early repair of iatrogenic bile duct injury. HPB (Oxford). 2015 May;17(5):394–400.
23. Pottakkat B, Vijayahari R, Prakash A, Singh RK, Behari A, Kumar A, et al. Incidence, pattern and management of bile duct injuries during cholecystectomy: experience from a single centre. Dig Surg. 2010; 27:375–9.
24. Pesce A, Fabbri N, Bonazza L, Feo C. The role of fluorescent cholangiography to improve operative safety in different severity degrees of acute cholecystitis during emergency laparoscopic cholecystectomy: a prospective cohort study. Int J Surg. 2024; 110:7775–81.
25. Giger U, Ouaissi M, Schmitz SH, Krähenbühl S, Krähenbühl L. Bile duct injury and use of cholangiography during laparoscopic cholecystectomy. Br J Surg. 2011;98(3):391–6.
26. Malla BR, Rajbhandari N, Karmacharya R. Management of bile duct injury following cholecystectomy. J Nepal Health Res Counc. 2020;18(2):214–18.
27. Vu HQ, Quach DT, Nguyen BH, Le ATQ, Le NQ, Pham HM, et al. Clinical presentation, management and outcomes of bile duct injuries after laparoscopic cholecystectomy: a 15-year single-center experience in Vietnam. Front Surg. 2023 Oct 11; 10:1280383.
28. Barrett M, Asbun HJ, Chien H-L, Brunt LM, Telem DA. Bile duct injury and morbidity following cholecystectomy: a need for improvement. Surg Endosc. 2018 Apr;32(4):1683–8.
29. Schmidt SC, Langrehr JM, Hintze RE, Neuhaus P. Long-term results and risk factors influencing outcome of major bile duct injuries following cholecystectomy. Br J Surg. 2005 Jan;92(1):76–82.
30. Schreuder AM, Busch OR, Besselink MG, Ignatavicius P, Gulbinas A, Barauskas G, et al. Long-Term Impact of Iatrogenic Bile Duct Injury. Dig Surg. 2020;37(1):10–21.
31. Ahmad S, Alzahrani NA, Al-Ghamdi S, Al-Mulhim A, Alqahtani S, Alessa M, et al. Surgical management and outcomes of bile duct injuries following cholecystectomy: a tertiary center experience. World J Surg. 2023;47(1):128–37.