Abstract
A patient with metastatic melanoma is treated with immunotherapy and achieved a partial response. On treatment holiday a right atrial metastasis is diagnosed radiologically. While cardiac surgery has been a historic consideration to treat this the use of dual immunotherapy with ipilimumab and nivolumab is discussed. This can provide a meaningful response and potentially increased DFS. Despite a response, other metastatic progression can still occur and close surveillance for CNS metastases may be important in this setting.
Keywords
Melanoma, Cardiac, Atrial, Metastasis, Immunotherapy, Metastatic
Introduction
It is long known that melanoma has the ability to metastasize widely. Unusual sites of metastases are seen including intra-cardiac. The literature reports cases of cardiac metastases however, most reports pre-date the more recent era of immunotherapy and targeted agent use and do not describe systemic treatment responses [1-3]. Prior to recent systemic therapy options surgery has been attempted to resect cardiac metastases [4]. This consideration would require review of a patient’s prognosis and whether ongoing symptoms were present. Surgery might be prioritized especially if a larger, obstructive lesion was present [5]. Certainly, surgical attempts for “fit” patients may be reasonable if overall survival would be on the order of a few months without this procedure. In contrast, only a few reports of utilizing immunotherapy without surgery are known. These do not provide description on long-term outcomes to help guide this selection. In one report, a patient prematurely stopped therapy due to immune-mediated side effects [6]. In another case despite side effects, anti-PD1 immunotherapy was continued and netted a partial response and stability of disease for 3 years [7]. This current report aims to provide further encouragement that systemic immunotherapy can be an effective treatment modality instead of electing immediate palliative care especially in cases where cardiac metastases are asymptomatic and where surgery is not desired or felt too risky.
Case Report
An 82-year-old man presented with a right parietal scalp melanoma in July 2014. He underwent resection of a stage T1aN0M0 lesion. Four months later satellitosis was seen and radiation to 30 Gy was administered. By March 2015 new in-transit satellite nodules were seen on the scalp. In lieu of surgery at his advanced age, radiation was again administered to 30 Gy. A new left cheek melanoma was diagnosed 2 years later in 2017. At this time staging studies showed pulmonary nodules consistent with metastatic disease. Gene mutational analysis showed BRAF wild type disease. He was treated with pembrolizumab as he did not have large volume disease (largest lesion was 1.1 cm). He attained a partial response and then stability on treatment through October 2019. At this time a LUL nodule grew to 2.2 cm (Figure 1). The patient had not yet reached a two-year treatment duration. Radiation to 48 Gy was given simultaneous to immunotherapy and pembrolizumab was continued through April 2020. At this time the irradiated LUL nodule was 1.6 cm. No new findings were seen and the patient endorsed interest in surveillance. The LUL nodule continued to show diminishing avidity on serial PET/CT scans. In March 2021 a new 1 cm RML nodule with mild PET avidity was seen. Additionally, abnormal avidity in the right atrial appendage to SUV 8.6 was reported (Figure 2). A cardiac MRI showed a filling defect in this area measuring 1.5 cm. A CTA TAVR also confirmed the filling defect in the right atrial appendage (Figures 3 and 4). No other cardiac lesions or valvular abnormalities were seen. Cardiac and Cardiothoracic Surgery consultations were obtained. Given the patient’s advanced age of 89, and in face of having had numerous metastases, it was not elected to offer surgery. Providing radiation to the right atrium was felt too risky to perform. The patient undertook reinstitution of immunotherapy. Ipilimumab/nivolumab as per new modification of lower dosed ipilimumab at 1 mg/kg and higher dosed nivolumab at 3 mg/kg was prescribed [8]. Four cycles were given and mild improvement to the right atrial metastasis was seen with new SUV 7.8 only 3 months later. At this time a prior RML nodule had increased in size to 1.4 cm having SUV 3.8. Radiation was given to the RML nodule with 50 Gy. Single agent nivolumab was continued monthly. Restaging in mid-September 2021 showed the cardiac metastasis continued to respond with SUV 5.1 and the RML nodule was stable (Figure 5). Nivolumab was continued through December 2021 (10 cycles total). At this time, he presented with delirium and hemiparesis. On evaluation, a 2 cm hemorrhagic parietal CNS lesion was seen. Discussion for stereotactic radiation to the CNS was made. Immunotherapy was held. The patient unfortunately had a decline in performance status and radiation were not given. He was admitted to rehabilitation for a few weeks and discharged home with hospice services. He had mild transient improvement and became more cognitively interactive and able to converse via telephone interview 10 months after the cardiac metastasis was diagnosed.

Figure 1. An axial PET/CT image demonstrates a new 2.2 cm left upper lobe mass with avidity as noted by arrow. This occurred after attaining a partial response to immunotherapy and stability of remaining disease at 1 ½-year treatment duration.

Figure 2. An axial PET/CT image reveals an arrow of strong avidity at right atrium of the heart (arrow) and a faint right middle lobe nodule (arrowhead). These findings developed off active therapy and amidst surveillance follow-up.
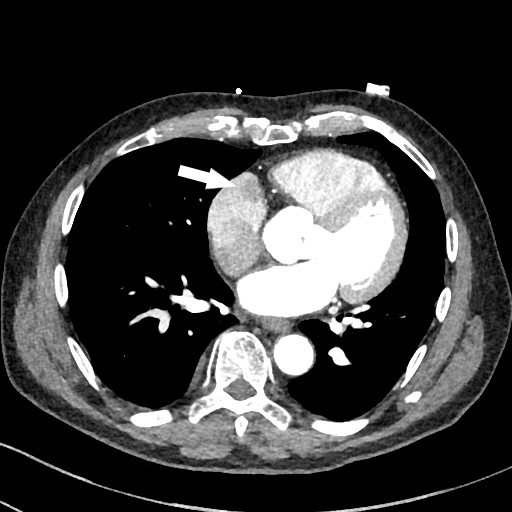
Figure 3. Cross sectional CT imaging demonstrates a mass lesion at mid right atrium (arrow) as initially noted on PET/CT.
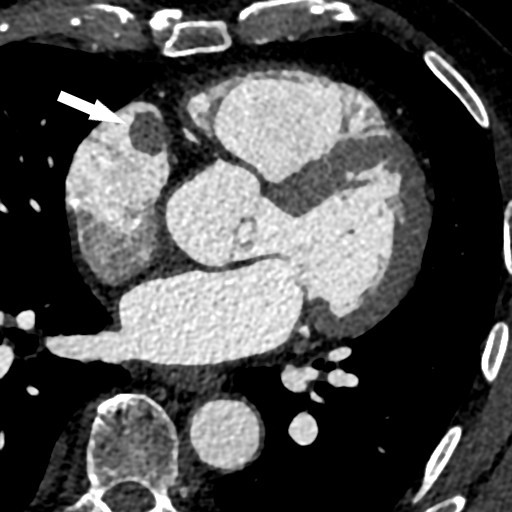
Figure 4. Axial imaging from CT TAVR shows the right atrial metastasis (arrow).
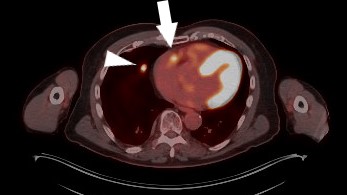
Figure 5. A follow-up axial PET/CT image after 6 months of immunotherapy shows significantly reduced PET avidity at right atrium (arrow). The right middle lobe mass has grown and was treated with XRT (an interim scan is not shown) and now demonstrates strong avidity but is stable over a 3 month period since radiation treatment (arrowhead).
Discussion
This case report demonstrates an often long-term treatment requirement and simultaneous unclear disposition for many patients with metastatic melanoma. Many patients do not attain a complete response and continued treatment to best partial response followed by surveillance is often needed. As noted treatment, holidays are considered, especially after a 2-year treatment duration, and further data regarding timing and duration of these is needed to guide therapy. Recently prolonged follow-up reporting of dual immunotherapy use from Checkmate 067 shows remarkable survivorship with upwards of 57% of patients alive at a median 6.5 years after receiving dual immunotherapy for unrespectable, advanced disease. The study’s construct pre-dates the new consideration of ipilimumab dose attenuation as per Checkmate 511 [8] and was not designed to determine which patients should be selected for dual immunotherapy rather than single agent anti-PD1 therapy [9]. In the present report dual immunotherapy was felt appropriate when metastatic relapse occurred after using anti-PD1 therapy and moreover in an unusual location. Despite ipilimumab dose attenuation, the patient showed demonstrable response on restaging PET/CT at 3 and more clearly 6 months. It was hoped he would continue to garner a response until a symptomatic CNS metastasis was unmasked. The CNS metastasis suggests it is possible that the unusual finding of an inter-cardiac metastases can be a sentinel of other, occult metastases. Despite a blood/brain barrier the long-term exposure of an intracardiac metastases could conceivably be a nidus for hematologic spread either preceding identification or during treatment. It is known that dual immunotherapy will provide a reasonable response to CNS metastases in about half of cases [10]. Unfortunately, CNS responses are not universal and prophylaxis against symptomatic, new metastases did not occur by dual immunotherapy in the presented case. Whether more diligent CNS screening would be needed for other patients with inter-cardiac metastases is unclear. Nonetheless, the patient experienced a long window of time where he remained active and asymptomatic from a cardiac metastasis and appeared to benefit from the described treatment. The patient and his family expressed gratitude for that.
Conclusion
Cardiac metastases from melanoma are rare but not unheard of. Few reports exist to guide treatment options. Surgery can be considered but may not be desirable. It is now emerging that immunotherapy, especially dual ipilimumab and nivolumab, is a feasible alternative to surgery although long-term outcomes are still unclear for the majority of such patients. In motivated subjects with advanced age or without a surgical option, the use of dual immunotherapy can be considered in lieu of palliative care.
Acknowledgements
Financial disclosure: none applicable.
Ethical disclosure: As a case report no IRB approval was necessary.
Conflicts of interest: There are no conflicts of interest.
Informed consent: None, no PHI was disclosed in this report.
Author contributions: Dr. Reuben has contributed solely and in whole to this report.
References
2. Tas F, Mudun A, Kirma C. Cardiac involvement in melanoma: a case report and review of the literature. Journal of Cancer Research and Therapeutics. 2010 Jul 1;6(3):359.
3. Kontozis L, Soteriou M, Papamichael D, Economides C, Bagdades E, Christou C, et al. Isolated right atrial metastasis of malignant melanoma mimicking a myxoma. Hellenic J Cardiol. 2011 May 1;52(3):281-4.
4. Lempereur-Legros S, Radermecker MA, Soyeur D, Limet, R. Cardiac metastasis from malignant melanoma. Rev Med Liege. 2009 Jan;64(1):8-10.
5. Noel A, Toquet C, Dewilde J. Prolonged survival after surgery for cardiac metastasis from malignant melanoma. J Cardiol Cases. 2014 Jul 19;10(4):150-52.
6. Poulsen CB, Weile KS, Schmidt H, Poulsen SH. A case report: metastasis of melanoma to the heart in an era of immunotherapy. European Heart Journal: Case Reports. 2019 Dec;3(4):1.
7. Yuki A, Takenouchi T, Takatsuka S, Ishiguro T. A case of pure red cell aplasia during nivolumab therapy for cardiac metastatic melanoma. Melanoma Research. 2017 Dec 1;27(6):635-7.
8. Lebbé C, Meyer N, Mortier L, Marquez-Rodas I, Robert C, Rutkowski P, et al. Evaluation of two dosing regimens for nivolumab in combination with ipilimumab in patients with advanced melanoma: results from the phase IIIb/IV CheckMate 511 trial. Journal of Clinical Oncology. 2019 Apr 10;37(11):867.
9. Wolchok JD, Chiarion-Sileni V, Gonzalez R, Grob JJ, Rutkowski P, Lao CD, et al. Long-term outcomes with nivolumab plus ipilimumab or nivolumab alone versus ipilimumab in patients with advanced melanoma. Journal of Clinical Oncology. 2022 Jan 10;40(2):127-37.
10. Kamath SD, Kumthekar PU. Immune checkpoint inhibitors for the treatment of central nervous system (CNS) metastatic disease. Frontiers in Oncology. 2018:414.