Abstract
Background: Hepatitis B virus (HBV) infection remains a public health burden resulting in over 50% of cases of hepatocellular carcinoma (HCC) worldwide. Despite successful HBV suppression with antiviral therapy, there is persistent risk for HCC development in HBV patients and lack of long-term longitudinal assessment.
Aim: Assess clinical outcomes after HCC diagnosis in antiviral-treated compared to antiviral-naïve patients.
Methods: A retrospective case series was performed observing patients for a period up to 24 years treated at a single tertiary medical center. Selected patients include those diagnosed with chronic hepatitis B (CHB) and HBV-related HCC (HBV-HCC). They were identified as being antiviral-treated or antiviral-naïve at the time of their HCC diagnosis. All patients were treated with nucleos(t)ide analog (NA) therapy after their initial HCC diagnosis. The primary endpoint for this study was death. Clinical characteristics, cumulative patient survival, and equality of survival distribution was assessed between the two groups.
Results: A total of 26 patients were identified where 13 were antiviraltreated and 13 were antiviral-naïve at the time of their first HCC diagnosis. 92.3% and 53.8% of antiviral-treated and antiviral-naïve patients, respectively were males. Patients in the antiviral-treated cohort were successfully treated with NA therapy for a median of 8 years prior to their first HCC diagnosis. After their first HBV-HCC event, death was observed more frequently among the antiviral-treated cohort at 46.2% as opposed to 15.4% in the antiviral-naïve cohort. All patients who died during the observation period were male. Of those surviving in the antiviral-treated cohort, 3 patients achieved liver transplantation. HBV-HCC patients previously treated with anti-HBV therapy had poorer survival rates than those naïve to therapy (p=0.008, log rank test=7.057).
Conclusion: Poorer survival was observed among antiviral-treated patients with breakthrough HBV-HCC compared to antiviral-naïve HBV-HCC patients. Early referral for liver transplantation is warranted for antiviral treated HBV-HCC patients.
Keywords
Chronic hepatitis B, Hepatocellular Carcinoma, HBV related HCC, Antiviral therapy, Hepatocarcinogenesis, HBV integration, Gender Disparity, Survival
Core Tip
Hepatitis B virus (HBV) accounts for over 50% of cases of hepatocellular carcinoma (HCC) worldwide. Although nucleos(t)ide analog (NA) therapy reduces risk for HCC, several studies have shown persistent risk for HCC despite antiviral therapy. The clinical outcomes of patients reaching breakthrough HCC has not been observed. Longitudinal observations up to a period of 24 years at our center have shown poorer survival outcomes in patients successfully treated with antiviral therapy, as opposed to those naïve to antiviral therapy. Proposed theories for this disparity include HBV integration with host DNA, the role of androgens, and altered host immune responses.
Introduction
Hepatitis B virus (HBV) infection is a public health problem, accounting for more than 257 million cases of chronic infection and a major cause of hepatocellular carcinoma (HCC) worldwide [1]. With the vaccination and the advent of nucleos(t)ide analogues (NAs) as antiviral therapy, chronic HBV infection currently accounts for approximately 50% of HCC cases worldwide, a significant decrease from >80% in the 1980’s [2-5]. The reduced incidence of HBV-related HCC (HBV-HCC) with NAs with lamivudine, entecavir, and tenofovir disoproxil fumarate is well documented [6-9]. On the other hand, several investigations, including large multicenter studies, have demonstrated that despite successful viral suppression, there remains a persistent risk for HCC while anti- HBV therapy [10-16].
However, although these studies demonstrated that a persistent risk for HBV-HCC remains despite successful antiHBV therapy, there have been no longitudinal observations showing the clinical outcome and survival of these patients who develop breakthrough HCC despite viral suppression. In effort to address this knowledge gap, the case series described here observed survival outcomes up period of 24 years between patients who developed HBV-HCC despite successful treatment with NA therapy (antiviral-treated) and patients who developed HBV-HCC without prior NA therapy (antiviral-naïve)
Materials and Methods
Study population
The study was a retrospective case series at a single tertiary medical center. Patients included in this study were observed for a period up to 24 years, with the earliest starting in 1996. Inclusion criteria were patients diagnosed with chronic hepatitis B (CHB) who developed HBV-HCC with active follow-up at our center upon chart review. Patients who were identified as antiviral-treated patients have had successful viral suppression with undetectable HBV DNA in serum. After diagnosis of their initial HCC, all patients received either surgical resection or loco-regional therapies, such as percutaneous ethanol injection (PEI), radiofrequency ablation (RFA), microwave ablation (MWA), or radioembolization. Furthermore, all patients were treated with NA therapy after HCC diagnosis. The primary endpoint observed in this study was death.
Statistical analysis
Statistics were performed using SPSS 27. The categorical data was analyzed with descriptive statistics. This was expressed with percentages along with ranges and median values. The Kaplan-Meier method was used to estimate overall survival curve, and the log rank test was adopted to evaluate the difference between groups.
Results
This case series included a total of 26 patients diagnosed with HBV-HCC. Thirteen patients were on NA therapy at their first diagnosis of HCC (Table 1 – antiviral-treated). Conversely, the other thirteen were naïve to antiviral therapy at the time of their first HCC diagnosis (Table 2 – antiviral-naïve). Antiviral experience patients had no detectable HBV DNA in serum at time of HCC diagnosis, whereas antiviral-naïve patients had varying levels of HBV DNA. Antiviral therapy used for antiviral treated patients Table 1 prior to HCC diagnosis included lamivudine (LAM) + tenofovir disoproxil fumarate (TDF) (patient #1-4, 8, 10, 12), TDF (patient #5-6, 9, 13), entecavir (ETV) (patient #11), and ETV + TDF (patient #7). The NA therapy was continued after diagnosis of HCC while treatment for the newly diagnosed HCC was initiated.
| Pt | Age (yrs) and sex at HCC Dx | Date of HCC Dx | FHx of HBV | Initial HCC size (cm) | AFP at HCC Dx (ng/mL) |
Anti-viral therapy | Tumor ablation* | HBV DNA at HCC Dx |
Yrs on anti-HBV Rx | Yrs of HBV DNA (-) | Status | Survival (yrs) |
| 1 | 63 M | 7/2007 | neg | 1.1 Rt | 2.4 | LAM + TDF | TACE (2007, 2010, 2011, 2014) |
UD | 9 | 3 | Alive (transplanted) | 12 |
| 2 | 70 M | 8/2007 | neg | 1.0 Rt | 8.3 | LAM + TDF | TACE (2007) TACE (2015) |
UD | 11 | 11 | Alive (terminal) | 13 |
| 3 | 54 F | 9/2010 | pos | 2.8 Rt | 6.8 | LAM + TDF | TACE (2010, 2012) | UD | 9 | 5 | Alive (transplanted) | 10 |
| 4 | 55 M | 1/2011 | pos | 2.8 Rt | 2.1 | LAM + TDF | TACE (2011) | UD | 10 | 5 | Dead | 2 |
| 5 | 57 M | 6/2013 | pos | 2.5 Lt | 377 | TDF | TACE (2014) | UD | 9 | 8 | Dead | 2 |
| 6 | 73 M | 7/2013 | pos | 1.6 Rt | 76.8 | TDF | TACE (2013, 2014) MWA (2015) |
UD | 17 | 10 | Dead | 2 |
| 7 | 54 M | 6/2014 | neg | 2.2 Rt | 90.1 | ETV + TDF | TACE (2014) MWA (2015, 2016) TARE (2020) |
UD | 17 | 6 | Dead | 5 |
| 8 | 74 M | 10/2014 | pos | 3.4 Rt | 1.2 | LAM + TDF | MWA (2014) TACE (2015) |
UD | 18 | 10 | Dead | 1 |
| 9 | 62 M | 4/2015 | pos | 3.4 Rt | 334 | TDF | TACE (2015) MWA (2015) |
UD | 15 | 12 | Alive | 6 |
| 10 | 64 M | 8/2017 | pos | 2.0 Rt | 9.0 | LAM + TDF | OSH ablation | UD | 19 | 8 | Alive (transplanted) | 3 |
| 11 | 60 M | 10/2017 | neg | 4.5 Rt | 9.1 | ETV | OSH ablation | UD | 17 | 10 | Dead | 2 |
| 12 | 57 M | 6/2019 | pos | 2.3 Rt | 9.5 | LAM + TDF | Lap-MWA (2019) | UD | 11 | 10 | Alive (metastasis, chemotherapy) | 1 |
| 13 | 61 M | 10/2019 | pos | 3.0 Lt | 5.9 | TDF | Resection (2019) OSH ablation (2021) |
UD | 14 | 10 | Alive (Transplant listed) | 1 |
|
F: Female; M: Male; Lt : Left; Rt: Right; FHx: Family History; Dx: Diagnosis; UD: Undetectable; yrs: Years; LAM: Lamivudine (150mg daily); TDF: Tenofovir Disoproxil Fumarate (300mg daily); ETV: Entecavir (1mg daily); TACE: Transarterial Chemoembolization; MWA: Microwave Ablation; TARE: Transarterial Chemoembolization; OSH Ablation: Outside Hospital Ablation; Lap-MWA: Laparoscopic Microwave Ablation *For list of HCC recurrences please refer to Figure 2. |
||||||||||||
All patients previously treated with NA therapy were identified as Child-Pugh (C-P) class A cirrhosis, except for patient #3.
Among patients naïve to antiviral therapy Table 2 at the time of HCC diagnosis, all patients were C-P class A, with the exception of patient #6, 13 who were not cirrhotic. As it has been clearly established in prior studies with favorable outcomes, antiviral naïve patients diagnosed with HCC underwent locoregional therapy along with initiation of anti-HBV therapy [17-23]. Antiviral-naïve patients NA therapies were TDF (patient #1, 4-10, 13), LAM (patient #3), LAM+TDF (patient #2, 11), or ETV+TDF (patient #12). Additionally, all patients had an initial single tumor size ≤ 5cm, except for patient #3 in the antiviralnaïve group with a 9 cm tumor.
| Pts | Age (yrs) and sex at HCC Dx | Date of HCC Dx | FHx of HBV | Initial HCC size (cm) | AFP at HCC Dx (ng/mL) |
Anti-viral ther- apy after HCC diagnosis | Tumor ablation* | HBV DNA at HCC Dx (IU/mL) | Status | Survival (yrs) |
| 1 | 63 F | 10/2000 | neg | 2.5 Rt | 6.7 | TDF | RFA (2000) TACE + MWA (2005) OSH ablation (2018) |
1.3x105 | Alive | 20 |
| 2 | 60 M | 9/2004 | pos | 3.4 Rt | 91.5 | LAM + TDF | TACE + RFA (2004) TACE (2014) | 98 | Dead | 15 |
| 3 | 64 F | 11/2004 | neg | 9.0 Rt | 7,981 | LAM | Resection (2004) | 641 | Alive | 16 |
| 4 | 57 M | 6/2005 | pos | 3.2 Rt | 3,066 | TDF | RFA + Resection (2005) | 2157 | Alive | 15 |
| 5 | 67 M | 1/2006 | neg | 1.0 Rt | 12.5 | LAM + TDF | RFA (2006) MWA (2014) |
2.0x106 | Alive | 14 |
| 6 | 20 F | 12/2007 | pos | 2.8 Rt | 11,944 | TDF | PCEI + RFA (2007) RFA (2008) TACE (2009) |
255 | Alive | 13 |
| 7 | 53 M | 3/2009 | pos | 1.9 Lt | 26.6 | TDF | TACE (2010) TACE + MWA (2017) |
164 | Alive | 10 |
| 8 | 66 M | 7/2010 | pos | 1.4 Rt | 3.9 | TDF | TACE (2010) TARE + TACE (2016) |
2745 | Dead | 7 |
| 9 | 55 F | 9/2010 | pos | 1.8 Rt | 5.1 | TDF | TACE (2010) | Neg (TDF started 1 month before) |
Alive | 10 |
| 10 | 51 M | 3/2009 | pos | 4.0 Rt | 42.8 | TDF | TACE (2009) MWA + TACE (2014) |
2745 | Alive | 10 |
| 11 | 56 M | 10/2011 | unk | 1.1 Rt | 5.0 | LAM + TDF | TACE (2011) Lap-RFA (2012) |
positive | Alive | 9 |
| 12 | 65 F | 2/2016 | pos | 2.8 Lt | 3.5 | ETV | MWA (2016) Lap-MWA (2017) |
Neg (TDF on 1 month) |
Alive | 4 |
| 13 | 47 F | 11/2017 | neg | 5.0 Lt | 17,735 | TDF | Resection (2017) | 2.4x106 | Alive | 3 |
|
TDF: Tenofovir Disoproxil Fumarate; F: Female; M: Male; Lt: Left; RT: Right; Dx: Diagnosis; FHx: Family History; yrs: Years; UNK: Unknown; LAM: Lamivudine (150mg daily); TDF: Tenofovir Disoproxil Fumarate (300mg daily); ETV: Entecavir (1mg daily); RFA: Radiofrequency Ablation; OSH ablation: Outside Hospital Ablation; TACE: Transarterial Chemoembolization; MWA: Microwave Ablation; TARE: Transarterial Radioembolization; PCEI: Percutaneous Ethanol Injection; Lap-MWA: Laparaoscopic Microwave Ablation; Lap-RFA: Laparoscopic Radiofrequency Ablation. *For list of HCC recurrences please refer to Figure 3. |
||||||||||
At the time of their first HCC diagnosis, patients in each group were of similar ages with a median of 61 and 57 in the antiviral-treated and antiviral-naïve groups respectively Table 3. Patients in the antiviral-treated group were predominantly male with only 1 female (92.3%), whereas 7 were male among the 13 (53.8%) in the antiviral-naïve group. Positive family history of HBV was present in 69.2% of antiviral-treated patients and was noted in 53.8% of treatment-naïve patients (although patient #11 had an unknown family history).
| Antiviral Treated (n=13) | Antiviral Naïve (n=13) | P-Value | |
| Age at first HCC diagnosis, median (IQRa, range)b | 61 (11, 54-74) | 57 (13, 20-67) | 0.431 |
| Male (n, %) | 12 (92.3%) | 7 (53.8%) | 0.077 |
| Family history of HBV (n, %) | 9 (69.2%) | 7 (61.1%) | 0.680 |
| Tumor size, median (IQR, range)b | 2.5 (1.4, 1.0-4.5) | 2.8 (2.1, 1.0-9.0) | 0.695 |
| AFP (ng/mL) at diagnosis, median (IQR, range)b | 9.0(79.3, 1.2-377) | 26.6 (5,518, 3.5-17,735) | 0.239 |
| Years of successful NA therapy prior to HCC diagnosis (median, range) | 8 (3-12) | Not applicable | - |
| Death during observation period (n, %) | 6 (46.2%) | 2 (15.4%) | 0.089 |
| aIQR =interquartile range bIndependent-Sample Median |
|||
Figure 1 demonstrates the years of successful antiviral treatment (HBV DNA undetectable) of the 13 patients who developed HCC while on therapy. The median number of years of successful NA therapy prior to HCC diagnosis for these patients was 8 years, with patient #1 having the shortest duration of NA therapy of 3 years prior to HCC diagnosis, and patient #9 the longest years of successful NA therapy of 12 years.
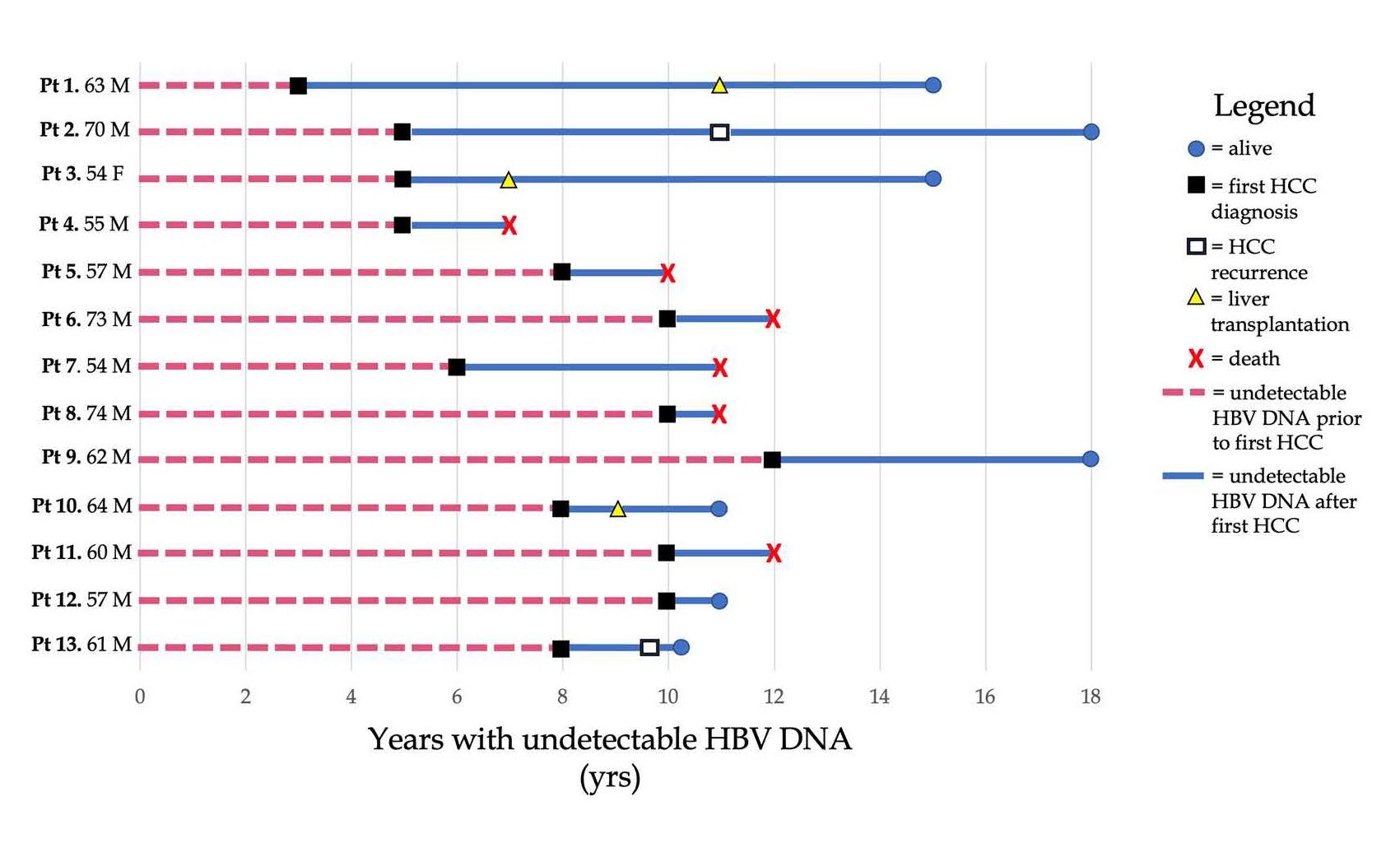
Figure 1. Years of undetectable HBV DNA prior to HCC diagnosis for anti-viral treated patients.
Figure 2 is modified from Figure 1 to display the survival from the time of HCC diagnosis in antiviral-treated patients. As demonstrated in Figure 2, the survival of patients who developed HCC while on successful antiviral therapy carried poor survival. Six of the thirteen patients (46.2%) died during the observed period, with 5 of 6 patients dying less than 3 years after HCC diagnosis. Only three patients in this cohort reached liver transplantation and survived (patients #1, #3, and #10).
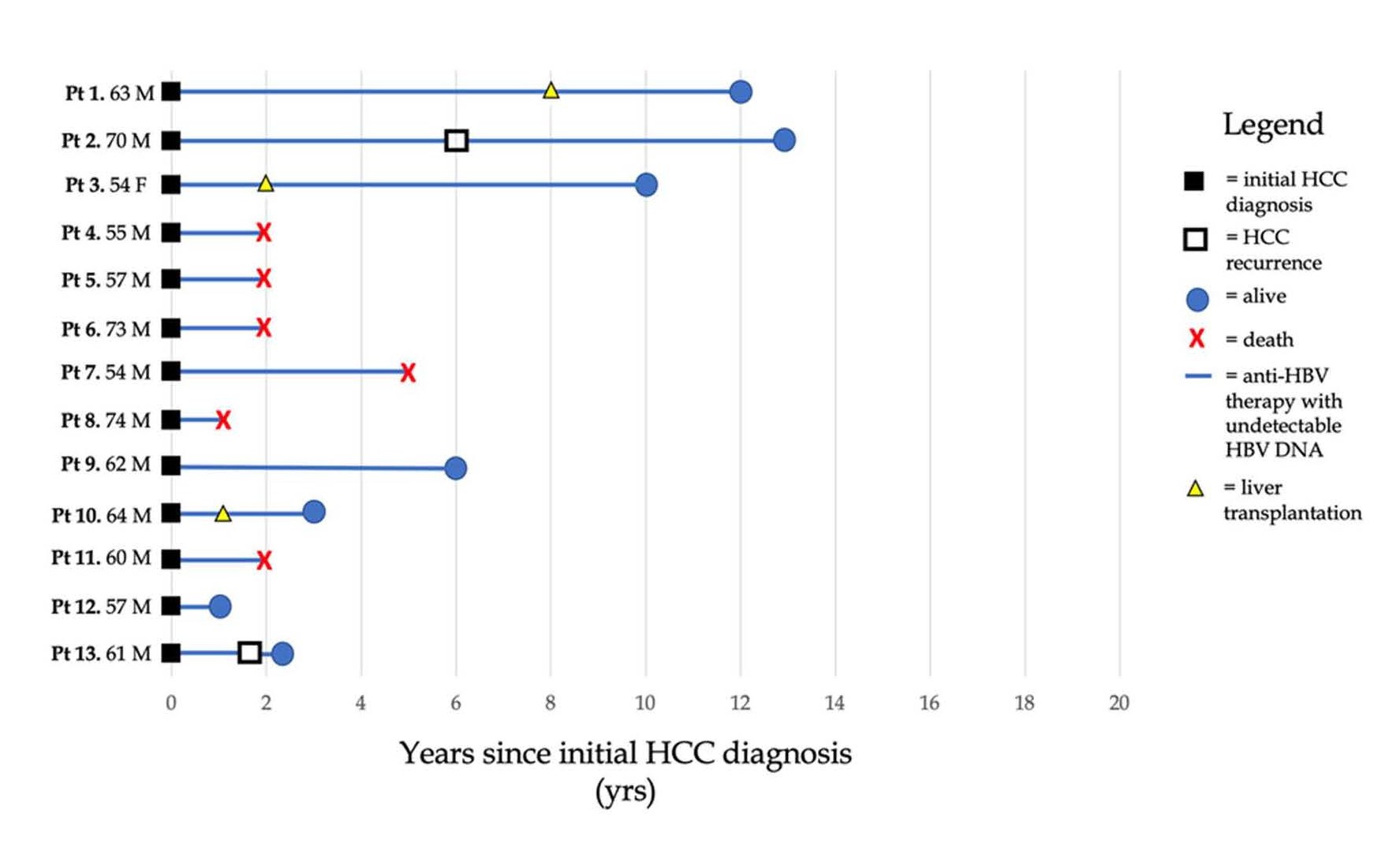
Figure 2. Years of survival of patients who developed HCC despite successful anti-viral therapy.
Figure 3 illustrates the length of survival of patients who were treatment naïve before the first diagnosis of HCC. These patients have lower mortality with only 2 of 13 Patients (15.4%) dying during the observation period.
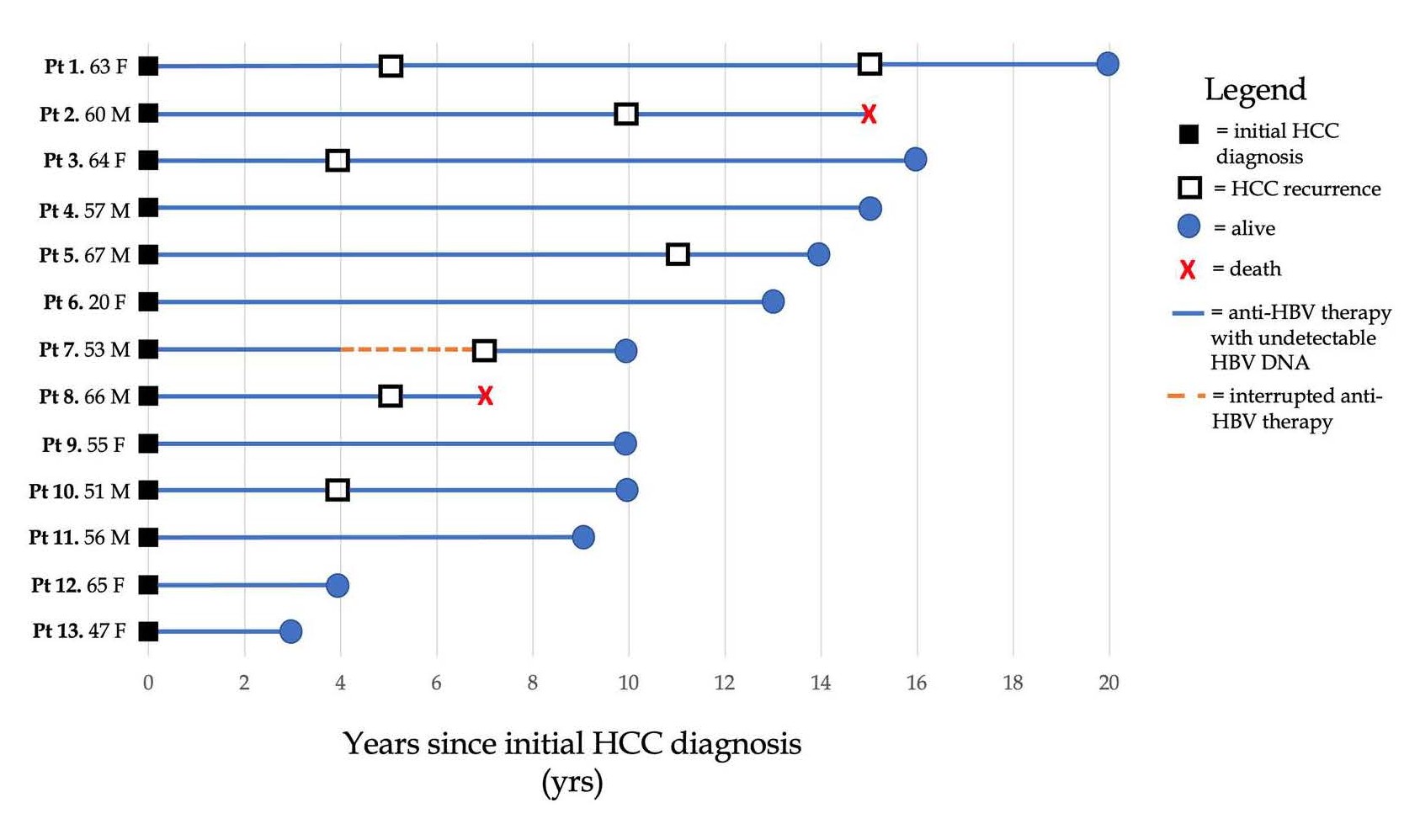
Figure 3. Lengths of survival for patients diagnosed with HCC: Patients naïve to anti-HBV therapy prior to first HCC diagnosis.
It is clear that there is a stark survival disparity between the antiviral-treated and naïve groups. Apart from three posttransplantation patients (#1, #3, #10), most antiviral-treated patients, 46.2% (6 of 13) died early, especially 5 of the 6 within 3 years after HCC diagnosis. In contrast, patients naïve to antiviral therapy had lower mortality with 15.4% of patients (2 of 13) dying during the observation period. Of note, all patients were started or continued antiviral therapy after HCC diagnosis and remained with undetectable HBV DNA levels, except for patient #7 who had a brief three-year period of interrupted antiviral therapy in the setting of compliance. The rates of death were 46.2% and 15.4% in the antiviral-treated and antiviral-naïve (X2=2.89, p=0.089), respectively. The rates of overall survival were lower in patients previously treated with antiviral therapy at the time of their HCC diagnosis than those naïve to antiviral therapy (X2=7.057, p=0.008) Figure 4.
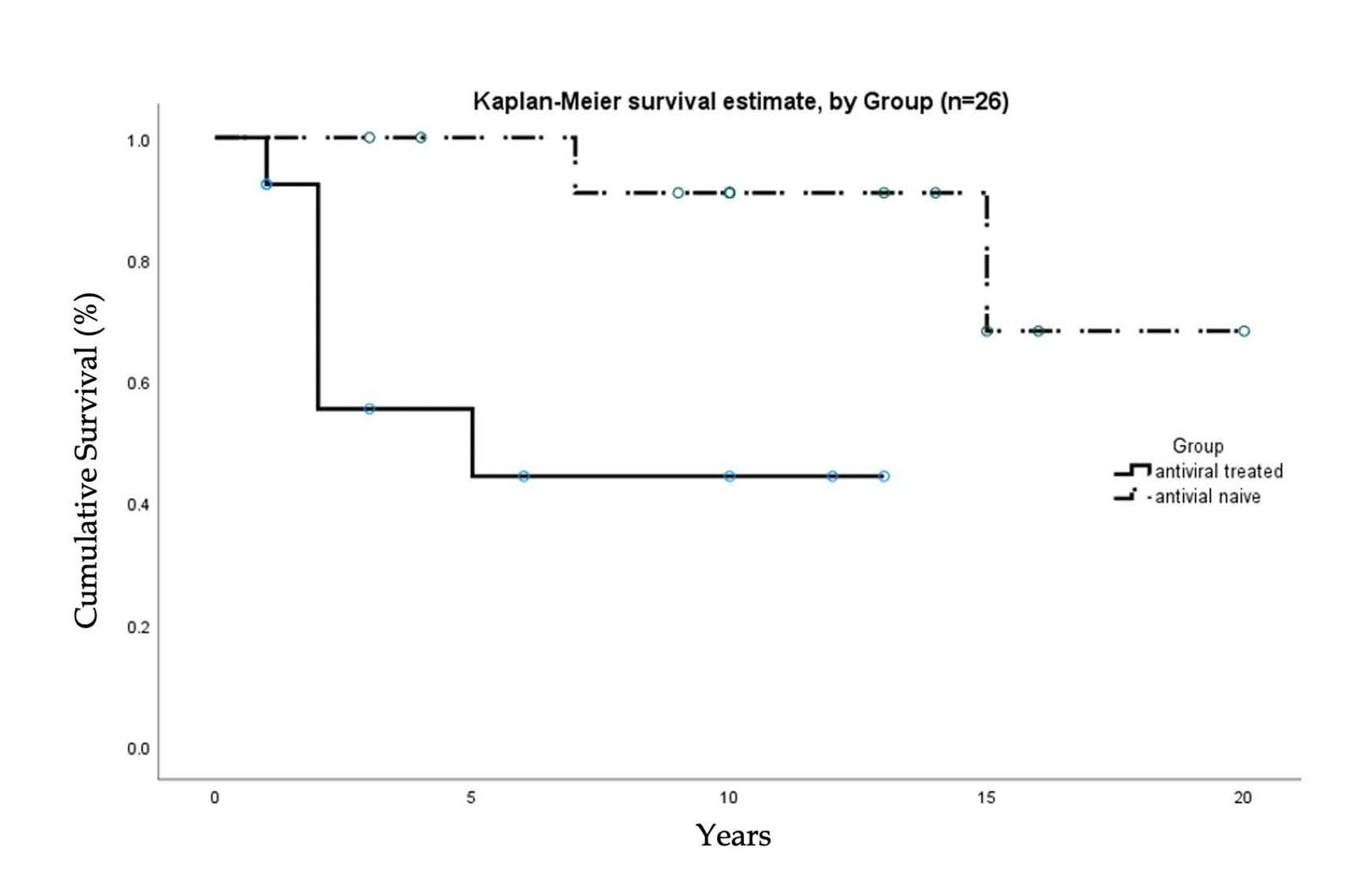
Figure 4. Kaplan-Meier curve of cumulative survival in antiviral treated and antiviral naïve patients.
As shown in Figure 3, among the antiviral-naïve patients, 7 of 13 patients developed the second new or recurrent HCC during their clinical course. With repeated local tumor ablation and continued antiviral therapy they survived. Patient #1 developed recurrence at the treated site (right lobe) 5 years after the first HCC, and 10 years later, a 1 cm new tumor appeared in the other lobe. On both occasions, the patient received local ablations and continued antiviral therapy. She survived over 20 years after the first HCC.
Discussion
It has been well-established that although antiviral therapy improves survival in patients with HBV infection, there remains the persistent risk for HCC. Our case series provides an opportunity to demonstrate that patients who develop HCC while on successful antiviral therapy carry poorer prognosis compared to those naïve to antiviral therapy prior to the development of HCC. It is unclear why those with longterm successful antiviral therapy were observed with worse survival/prognosis upon HCC diagnosis.
One mechanism that can potentially contribute to worse survival in patients receiving long-term antiviral therapy is integration of HBV DNA into the host genome. Halting HBV replication at the reverse transcription phase of the viral life cycle for prolonged period may increase priming the HBVinfected hepatocytes for enhanced turnover of HBV DNA integration events which are known to cause insertional mutagenesis and genomic instability [24]. While HBV DNA can integrate randomly into the host genome, over the course of chronic HBV infection there is an increased potential for integration to occur at critical HCC driver genes giving rise to clonally-expanded aggressive malignant HBV-infected hepatocytes. Thus, despite successful suppression of viral replication with long-term anti-viral therapy, integration can still occur and potentially contribute to the survival disparity seen in this cohort. Additionally, HBV integration can produce chimeric HBV antigens potentially priming immune responses and exacerbating immune dysfunction [25]. With the continuous halting of HBV DNA transcription due to successful antiviral therapy, accumulation of unfinished viral products including several transcribed mRNAs may occur. This may increase integration between HBV DNA and host DNA. Upon HCC development in the presence of continuous suppression of viral replication, cancerous cells may be primed/evolved in a more vicious and malignant manner. It remains to be further explored the HBV integration sites between the two cohorts.
Furthermore, HBV DNA integration events in the TERT promoter have been shown to render TERT transcription responsive to sex hormones enhanced by the androgen receptor, a new mechanism proposed for the male dominance of HBV-HCCs [26]. Interestingly in this study, we predominantly see the male gender in patients previously treated with antiviral therapy compared to those naïve to antiviral therapy (92.3% vs. 53.8%). Male patients have been known to have a generally poorer prognosis than females in HCC [27]. This is likely in part to the role androgens have in promoting HBVHCC [28].
Another potential mechanism for our findings may include altered host immune responses to HBV-HCC in patients previously treated with antiviral therapy. Infection with CHB is known to exhaust host HBV-specific T-cells and increase expression of inhibitory checkpoint molecules such as PD-1 and CTLA-4 [29]. Luo et. al. demonstrated that in CHB patients, antiviral therapy restored these HBV-specific immune responses, and subsequently suppressed HBV replication [30]. However, it is unclear if this immune reconstitution may inadvertently contribute to the progression to HCC in certain individuals due to dysfunctional inflammatory responses causing DNA damage, genomic instability, etc.
Conclusion
Our longitudinal period of observation approaching 20 years allowed an opportunity to observe the difference in survival between antiviral-treated and antiviral-naïve patients who develop their first HBV-HCC.
These findings provide a unique opportunity for discussion and investigation into this disparity. As shown in prior studies of favorable outcomes with concomitant anti-HBV therapy, patients who are naïve to antiviral treatment and subsequently develop HCC may benefit from initial treatment with loco-regional therapy along with initiation of anti-HBV therapy. While the etiology for our findings remains unclear, these observations suggest that for patients who develop HCC despite successful long-term anti-HBV therapy, the best management would be early referral for liver transplantation. Our observation encourages further investigation of the possible causes and improvement of outcomes in patients who develop HCC despite successful viral suppression.
Author Contributions
D Garrido contributed to the data analysis and writing of the manuscript. P Block contributed to the writing and editing of the manuscript. S Lin contributed to the interpretation of findings of the study. D Halegoua-DeMarzio contributed to the editing of the manuscript. HW Hann conceived the idea for the manuscript and assisted in writing and editing.
Conflict of Interest
HW Hann: Serves the National Advisory Board of The Gilead Sciences. Receives grant from Gilead and Assembly Biosciences. All other authors declared that there are no conflicts of interest.
References
2. Perz JF, Armstrong GL, Farrington LA, Hutin YJ, Bell BP. The contributions of hepatitis B virus and hepatitis C virus infections to cirrhosis and primary liver cancer worldwide. Journal of Hepatology. 2006 Oct 1;45(4):529-38.
3. Jemal A, Bray F, Center MM, Ferlay J, Ward E, Forman D.Global cancer statistics. CA: A Cancer Journal for Clinicians. 2011 Mar;61(2):69-90.
4. El-Serag HB. Hepatocellular carcinoma: recent trends in the United States. Gastroenterology. 2004 Nov 1;127(5):S27-34.
5. Ha J, Yan M, Aguilar M, Bhuket T, Tana MM, Liu B, et al. Race/ ethnicity-specific disparities in cancer incidence, burden of disease, and overall survival among patients with hepatocellular carcinoma in the United States. Cancer. 2016 Aug 15;122(16):2512-23.
6. Liaw YF, Sung JJ, Chow WC, Farrell G, Lee CZ, Yuen H, et al. Lamivudine for patients with chronic hepatitis B and advanced liver disease. New England Journal of Medicine. 2004 Oct 7;351(15):1521- 31.
7. Eun JR, Lee HJ, Kim TN, Lee KS. Risk assessment for the development of hepatocellular carcinoma: according to on-treatment viral response during long-term lamivudine therapy in hepatitis B virusrelated liver disease. Journal of Hepatology. 2010 Jul 1;53(1):118-25.
8. Hosaka T, Suzuki F, Kobayashi M, Seko Y, Kawamura Y, Sezaki H, et al. Long-term entecavir treatment reduces hepatocellular carcinoma incidence in patients with hepatitis B virus infection. Hepatology. 2013 Jul;58(1):98-107.
9. Kim WR, Berg T, Loomba R, Schall RA, Dinh P, Yee LJ, et al. 43 long term tenofovir disoproxil fumarate (tdf) therapy and the risk of hepatocellular carcinoma. Journal of Hepatology. 2013(58):S19.
10. Papatheodoridis GV, Manolakopoulos S, Touloumi G, Vourli G, Raptopoulou-Gigi M, Vafiadis-Zoumbouli I, et al. Virological suppression does not prevent the development of hepatocellular carcinoma in HBeAg-negative chronic hepatitis B patients with cirrhosis receiving oral antiviral (s) starting with lamivudine monotherapy: results of the nationwide HEPNET. Greece cohort study. Gut. 2011 Aug 1;60(8):1109-16.
11. Papatheodoridis GV, Lampertico P, Manolakopoulos S, Lok A. Incidence of hepatocellular carcinoma in chronic hepatitis B patients receiving nucleos (t) ide therapy: a systematic review. Journal of Hepatology. 2010 Aug 1;53(2):348-56.
12. Vlachogiannakos J, Papatheodoridis G. Hepatocellular carcinoma in chronic hepatitis B patients under antiviral therapy. World Journal of Gastroenterology: WJG. 2013 Dec 21;19(47):8822-30.
13. Dargan A, Wong SY, Coben R, Conn M, Dimarino AJ, Hann HW. Persistent risk for hepatocellular carcinoma after more than a decade of successful hepatitis B virus suppression. Minerva Gastroenterologica e Dietologica. 2017 Mar;63(1):74-6.
14. Yoo J, Hann HW, Coben R, Conn M, DiMarino AJ. Update treatment for HBV infection and persistent risk for hepatocellular carcinoma: prospect for an HBV cure. Diseases. 2018 Jun;6(2):27.
15. Shinn BJ, Kristler C, Roth C, Hann HW. Need For HBV Cure: Persistent Risk For Subsequent New And Recurrent HCC Even After A Decade Of Successful Anti-HBV Therapy And Initial Tumor Ablation. Arch Cancer Res. 2018; 6: 1–6.
16. Shinn BJ, Martin A, Coben RM, Conn MI, Prieto J, Kroop H, et al. Persistent risk for new, subsequent new and recurrent hepatocellular carcinoma despite successful anti-hepatitis B virus therapy and tumor ablation: The need for hepatitis B virus cure. World Journal of Hepatology. 2019 Jan 27;11(1):65-73.
17. Piao CY, Fujioka SI, Iwasaki Y, Fujio K, Kaneyoshi T, Araki Y, et al. Lamivudine treatment in patients with HBV-related hepatocellular carcinoma--using an untreated, matched control cohort. Acta Medica Okayama. 2005;59(5):217-24.
18. Kuzuya T, Katano Y, Kumada T, Toyoda H, Nakano I, Hirooka Y, et al. Efficacy of antiviral therapy with lamivudine after initial treatment for hepatitis B virus-related hepatocellular carcinoma. Journal of Gastroenterology and Hepatology. 2007 Nov;22(11):1929-35.
19. Kubo S, Tanaka H, Takemura S, Yamamoto S, Hai S, Ichikawa T, Kodai S, et al. Effects of lamivudine on outcome after liver resection for hepatocellular carcinoma in patients with active replication of hepatitis B virus. Hepatology Research. 2007 Feb;37(2):94-100.
20. Kim BK, Park JY, Kim DY, Kim JK, Kim KS, Choi JS, et al. Persistent hepatitis B viral replication affects recurrence of hepatocellular carcinoma after curative resection. Liver International. 2008 Mar;28(3):393-401.
21. Hann HW, Bergin D, Coben R, DiMarino AJ. Prevention of new hepatocellular carcinoma with concomitant antiviral therapy in chronic hepatitis B patients whose initial tumor was successfully ablated. International Journal of Cancer. 2011 Feb 1;128(3):739-42.
22. Hann HW, Coben R, Brown D, Needleman L, Rosato E, Min A, et al. A long-term study of the effects of antiviral therapy on survival of patients with HBV-associated hepatocellular carcinoma (HCC) following local tumor ablation. Cancer Medicine. 2014 Apr;3(2):390-6.
23. Hui VW, Chan SL, Wong VW, Liang LY, Yip TC, Lai JC, et al. Increasing antiviral treatment uptake improves survival in patients with HBV-related HCC. JHEP Reports. 2020 Dec 1;2(6):100152.
24. Lin SY, Zhang A, Lian J, Wang J, Chang TT, Lin YJ, et al. Recurrent HBV Integration Targets as Potential Drivers in Hepatocellular Carcinoma. Cells. 2021 Jun;10(6):1294.
25. Rivino L, Le Bert N, Gill US, Kunasegaran K, Cheng Y, Tan DZ, et al. Hepatitis B virus–specific T cells associate with viral control upon nucleos (t) ide-analogue therapy discontinuation. The Journal of Clinical Investigation. 2018 Feb 1;128(2):668-81.
26. Li CL, Li CY, Lin YY, Ho MC, Chen DS, Yeh SH, et al. Androgen Receptor Enhances Hepatic TERT Transcription after Hepatitis B Virus Integration or Point Mutation in Promoter Region [J]. Hepatology. 2018;69: 498-512.
27. Tangkijvanich P, Mahachai V, Suwangool P, Poovorawan Y. Gender difference in clinicopathologic features and survival of patients with hepatocellular carcinoma. World Journal of Gastroenterology: WJG. 2004 Jun 1;10(11):1547-1550.
28. Montella M, D’Arena G, Crispo A, Capunzo M, Nocerino F, Grimaldi M, et al. Role of sex hormones in the development and progression of hepatitis B virus-associated hepatocellular carcinoma. International Journal of Endocrinology. 2015 Sep 27;2015:854530.
29. Ferrari C. HBV and the immune response. Liver International. 2015 Jan;35:121-8.
30. Luo G, Feng X, Huang Y, Yi T, Wang D, Guo X, et al. Effects of antiviral therapy on the cellular immune response in patients with chronic hepatitis B. Molecular Medicine Reports. 2015 Feb 1;11(2):1284-91.