Abstract
Background: Metastatic pancreatic ductal adenocarcinoma (mPDAC) remains one of the most lethal solid tumors, with poor survival despite modern chemotherapy. Traditional efficacy metrics such as objective response rate (ORR) and RECIST-defined progression-free survival (PFS) may incompletely capture the biologic effects of immunotherapy, particularly therapies designed to induce durable systemic immune surveillance rather than immediate cytoreduction.
Observation: In patients receiving more than five doses of Saltikva (orally administered attenuated Salmonella enterica Typhimurium expressing human IL-2) in combination with FOLFIRINOX, only 4 of 20 developed new metastatic lesions, while 16 (80%) progressed through enlargement of pre-existing metastatic disease without radiographic evidence of de novo metastatic spread.
Hypothesis: This pattern suggests possible immune-mediated suppression of micrometastatic dissemination and may represent evidence of functional immune memory rather than transient immune activation.
Conclusion: Freedom from new metastatic disease may serve as a clinically meaningful endpoint for microbial immunotherapies and could represent a stronger indicator of biologic efficacy than ORR alone.
Keywords
Cancer immunology, Immunotherapy, Tumor immunology
Introduction
Pancreatic ductal adenocarcinoma (PDAC) remains one of the most lethal malignancies worldwide, with more than 500,000 new cases diagnosed annually and a steadily rising incidence projected to approach 1 million cases globally by 2050 [1]. Owing to the absence of effective early detection strategies, approximately 40–50% of patients present with metastatic (stage IV) disease, representing more than 200,000 newly diagnosed metastatic cases each year. For these patients, current first-line standard-of-care (SOC) therapy consists of multi-agent chemotherapy with either FOLFIRINOX/NALIRIFOX or gemcitabine plus nab-paclitaxel (GEM/nabP) [2,3]. Despite decades of clinical investigation, outcomes remain poor. A recent meta-analysis of seven first-line trials including 2,581 patients demonstrated median progression-free survival (mPFS) of only 7.3–7.4 months and median overall survival (mOS) of 11.1–11.7 months for FOLFIRINOX and NALIRIFOX, while GEM/nabP produced an mPFS of 5.7 months and mOS of 10.4 months [4]. Numerous studies evaluating targeted therapies, immune checkpoint inhibitors, and novel combination regimens have failed to produce consistent survival improvements beyond these benchmarks, underscoring the profound immune resistance, dense stromal barriers, and highly immunosuppressive tumor microenvironment that characterize metastatic PDAC [5]. These limitations highlight the urgent need for fundamentally different therapeutic strategies capable of overcoming these biologic barriers.
Microbial-based cancer therapeutics have emerged as a promising new therapeutic category because of their intrinsic tumor-targeting properties and ability to stimulate durable antitumor immune responses [6,7]. Saltikva (Salmonella-IL2) is an orally administered, attenuated strain of Salmonella enterica serovar Typhimurium genetically engineered to express the human interleukin-2 (IL-2) gene [8]. This live biotherapeutic platform is designed to preferentially localize within the tumor microenvironment, where it delivers sustained local IL-2 production while minimizing the systemic toxicity associated with intravenous cytokine therapy [9]. Preclinical studies have demonstrated significant antitumor activity across multiple solid tumor models, including metastatic colorectal cancer, pancreatic cancer, neuroblastoma, osteosarcoma, and breast cancer, with evidence of both direct tumor cytotoxicity and enhanced immune activation [8–15]. In a large-animal translational study in companion dogs with pulmonary metastatic osteosarcoma, Salmonella-IL2 combined with doxorubicin produced a 22% complete response rate and significantly prolonged disease-free survival compared with doxorubicin alone [16]. A Phase I single-dose dose-escalation trial in patients with metastatic gastrointestinal cancers further demonstrated favorable tolerability without dose-limiting toxicities up to 1010 CFU and showed significant increases in circulating NK and NKT cell populations following administration, supporting both safety and biologic activity [17].
Building on these findings, a completed Phase II non-randomized clinical trial evaluated adjunctive oral Saltikva in patients with stage IV metastatic PDAC receiving SOC chemotherapy [18,19]. Thirty-four patients received Saltikva in combination with either modified FOLFIRINOX (n=26) or GEM/nabP (n=8), with outcomes compared to institutional historical controls treated with identical chemotherapy regimens between 2016 and 2020. Among patients receiving Saltikva plus FOLFIRINOX who completed at least five doses (n=20), median progression-free survival reached 15.0 months compared with 5.8 months in historical controls (HR 0.30, p<0.0001), while median overall survival improved to 20.3 months versus 11.5 months (HR 0.59, p=0.07). Objective response rates approached 70%, representing one of the highest reported response rates in first-line metastatic PDAC. Importantly, across the Phase II and Expanded Access cohorts, no serious adverse events were attributed to Saltikva; all observed serious adverse events were attributed to standard chemotherapy, supporting a strong safety profile. These outcomes compare favorably to those reported in a recent Phase III trial of the KRAS inhibitor Daraxonrasib in patients with metastatic PDAC, where the objective response rate was 47% and median overall survival was 13 months, further highlighting the potential clinical significance of Saltikva as a novel first-line therapeutic strategy [20]. These findings suggest that oral microbial immunotherapy may define a new therapeutic approach in metastatic PDAC by combining standard cytotoxic therapy with durable, tumor-localized immune activation.
Methods
A Health Canada and IRB-approved, non-randomized Phase II trial evaluated Saltikva in patients with stage IV pancreatic ductal adenocarcinoma treated at the Segal Cancer Centre, Jewish General Hospital, McGill University. Patients received first-line standard-of-care chemotherapy with either modified FOLFIRINOX (n=26) or gemcitabine/nab-paclitaxel (n=8) in combination with orally administered Saltikva, an attenuated Salmonella enterica Typhimurium engineered to express human IL-2. Saltikva was administered orally at 109 CFU every two weeks following gastric acid neutralization; in the FOLFIRINOX arm, dosing occurred three days after each chemotherapy cycle. Four additional patients meeting identical eligibility criteria were treated through an Expanded Access Program and included in the FOLFIRINOX cohort.
Eligible patients were adults with histologically confirmed metastatic PDAC, measurable distant metastatic disease by RECIST 1.1, and ECOG performance status ≤1 [21]. Patients receiving other investigational agents or with brain metastases were excluded. Primary endpoints were progression-free survival (PFS) and overall survival (OS), with radiologic progression determined by blinded radiologists using RECIST 1.1 criteria. Secondary endpoints included objective response rate, biomarker responses, and safety.
Because the focus of this analysis was metastatic progression patterns, each patient’s serial CT imaging was specifically reviewed to distinguish progression due to enlargement of pre-existing metastatic lesions from progression caused by development of de novo metastatic disease. Particular attention was given to patients receiving at least five doses of Saltikva, as this subgroup demonstrated the strongest survival benefit and provided the clearest opportunity to assess whether treatment was associated with suppression of new metastatic spread.
Outcomes were compared with institutional historical controls consisting of patients treated at the same center between 2016 and 2020 with FOLFIRINOX alone (n=37) or gemcitabine/nab-paclitaxel alone (n=31). This method of comparing to the same site historical controls is an accepted method when there is a rare disease especially, in a single site, signal seeking phase II trial [24,25]. These patients were managed by the same oncology team, and radiographic response was assessed using identical RECIST 1.1 criteria by radiologists blinded to outcomes, providing a consistent comparator for survival and metastatic progression patterns.
Survival distributions were estimated using Kaplan-Meier methodology with log-rank testing and Cox proportional hazards regression. Adverse events were graded using CTCAE v5.0, and all serious adverse events were reviewed for attribution to chemotherapy or Saltikva [22,23]. Patients alive at the March 1, 2025 data cutoff were censored at last follow-up.
RESULTS: Clinical Activity and Efficacy: Saltikva + FOLFIRINOX
The strongest clinical benefit was observed in patients receiving more than five doses of Saltikva plus FOLFIRINOX (n=20). In this group, median progression-free survival (mPFS) improved significantly to 15.0 months compared with 5.8 months in FOLFIRINOX-only historical controls (HR 0.30, p<0.001), while median overall survival (mOS) increased to 20.3 months versus 11.5 months (HR 0.59, p<0.05). These findings were supported by Kaplan-Meier and kernel density analyses demonstrating a clear rightward shift in both PFS and OS curves, consistent with a reduced risk of progression and death.
Importantly, while all patients ultimately experienced disease progression, only 4 of 20 (20%) developed de novo metastatic lesions. The remaining 16 (80%) patients progressed through enlargement of pre-existing metastatic disease without formation of new metastases, suggesting a potential immune memory effect associated with sustained Saltikva exposure (Figure 1). Similar survival trends were observed across sensitivity analyses including compliant patients with and without Expanded Access Program enrollment, supporting the consistency of this therapeutic signal.
The Wilson score method was the statistical approach used to calculate confidence intervals for binomial proportions. Unlike the standard normal approximation, the Wilson method performs better with small sample sizes and proportions close to 0 or 1, producing more accurate and stable confidence intervals. Thus, 16/20 patients without new metastatic disease = 80% (95% Wilson CI: approximately 58%–92%). Furthermore, 4/20 patients with new metastatic disease = 20% (95% Wilson CI: approximately 8%–42%) The p-value (p = 0.0137) comes from a two-sided exact binomial test comparing the observed 80% rate against a null hypothesis of 50%. This suggests the observed predominance of progression of existing metastases over development of new metastases is unlikely due to random chance alone within this cohort.
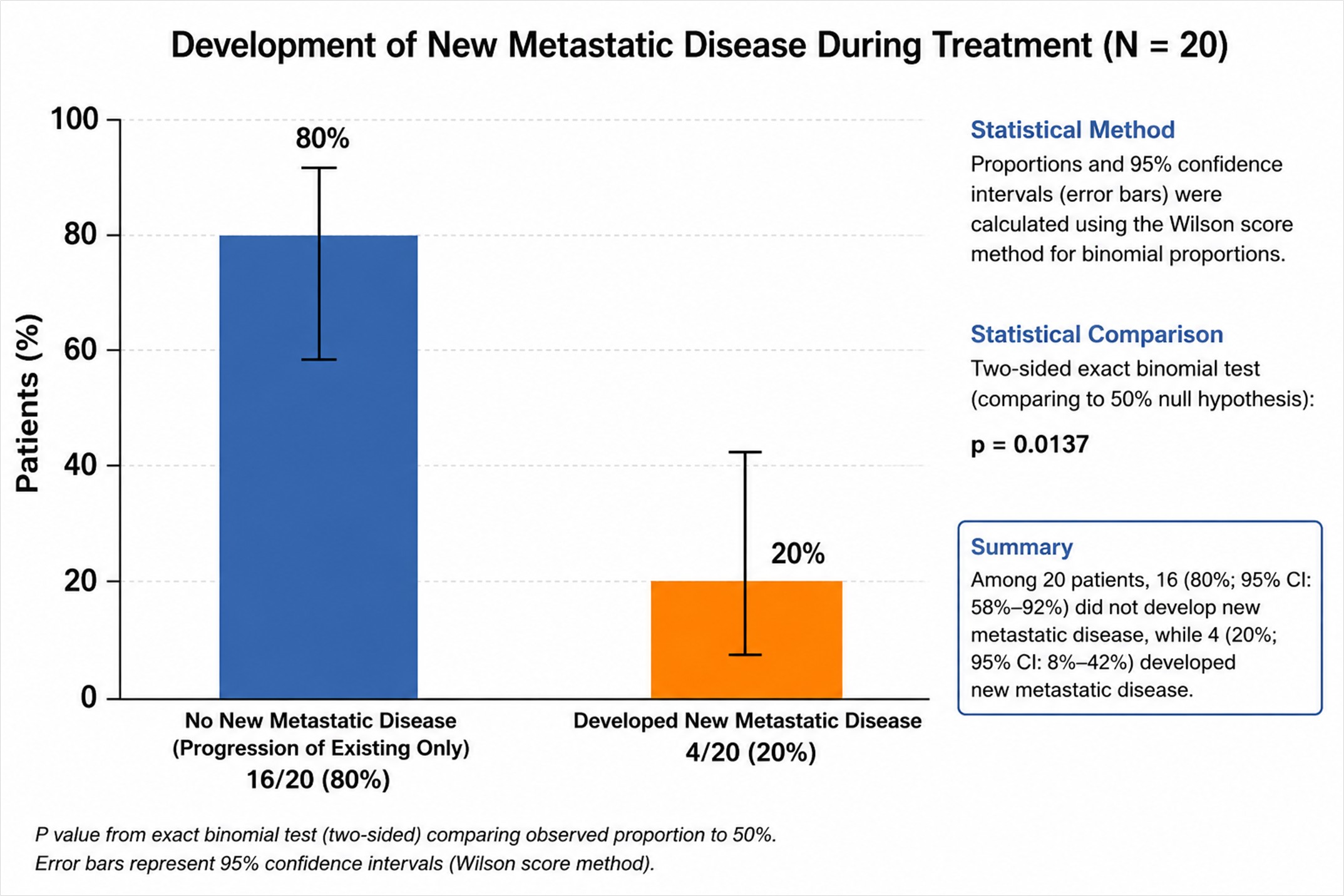
Figure 1. Development of new metastatic disease during treatment. Among 20 evaluable patients, 16 (80%; 95% CI: 58%–92%) demonstrated progression of pre-existing metastases without development of new metastatic disease, whereas 4 patients (20%; 95% CI: 8%–42%) developed additional metastatic lesions. Error bars represent Wilson score 95% confidence intervals. Two-sided exact binomial test: p = 0.0137.
Discussion
Metastatic pancreatic ductal adenocarcinoma remains one of the most lethal solid tumors, with standard first-line chemotherapy producing median progression-free survival of approximately 6 months and median overall survival of approximately 11 months [26]. Even recent therapeutic advances remain modest. Revolution Medicines’ Daraxonrasib has shown important activity in mPDAC, including a 47% objective response rate in first-line monotherapy and, in the pretreated Phase III RASolute 302 trial, median overall survival of 13.2 months versus 6.7 months with standard chemotherapy [20].
In comparison, patients in this study who received more than five doses of Saltikva plus FOLFIRINOX (n=20) demonstrated median progression-free survival of 15.0 months versus 5.8 months in FOLFIRINOX-only controls, and median overall survival of 20.3 months versus 11.5 months, with an objective response rate of 70%. Although this was not a head-to-head comparison, these findings compare favorably with the most active emerging therapies in mPDAC.
Most importantly, the distinctive finding in this cohort was not only prolonged survival, but altered metastatic behavior. Although all patients ultimately progressed, only 4 of 20 developed de novo metastatic lesions; the remaining 16 (80%) progressed through growth of pre-existing disease without new metastatic sites. This pattern suggests that Saltikva may induce immune surveillance capable of suppressing metastatic seeding. This hypothesis is supported by preclinical colorectal cancer liver metastasis models in which mice treated with a single oral dose of Saltikva were later rechallenged by direct portal vein injection of tumor cells. In that model, 100% of rechallenged mice survived and none developed recurrent tumors, consistent with durable antitumor immune memory rather than transient cytotoxic activity [11,12].
Conclusion
The absence of new metastatic disease in the most heavily treated Saltikva patients may represent one of the most important biologic signals in this Phase II Clinical Trial in patients with stage 4 metastatic pancreatic cancer. For microbial immunotherapy, prevention of metastatic dissemination may be a more meaningful measure of success than tumor shrinkage alone. This observation supports the hypothesis that Saltikva may induce durable immune memory. A future planned randomized Phase III clinical trial will thoroughly investigate this potential through prospective evaluation incorporating detailed immune profiling and assessment of metastatic progression patterns.
Acknowledgements
This clinical trial and the extensive amount of research and support to developed Salmonella-IL2 would not have been possible without the support of many. The concept of bacterial based cancer therapy and specifically Salmonella-IL2 requires a paradigm shift in one’s thinking and belief on how cancer should be treated. Specifically, research support from the NIH’s R-2CA131194 which funded the preliminary data that ultimately led to this clinical trial. In addition, support from Weist Family Foundation, the A. S. Leonard Endowed Chair at the University of Minnesota, the A.S. Leonard Cancer Research Foundation, and Project Stealth at the University of Minnesota created by Max Duckler, Judy Kessel, Jerrold Gershone and a host of extremely dedicated individuals at StoneArch Creative. Lastly, the selfless commitment by the Data Safety and Monitoring Committee that oversaw this clinical trial, specifically, Max Duckler, Dr. Jimmy Levine, Dr Steven Robinson, and Dr. Chris Moertel.
This phase II clinical trial study was sponsored by Salspera, Inc; Gerald Batist MD served as the principal investigator of this phase II clinical trial.
Conflicts of Interest Disclosure
Dr. Daniel Saltzman is a Professor of Surgery and Pediatrics and the Chief of Pediatric Surgery at the University of Minnesota. The therapeutic technology that is the subject of this manuscript was developed in his laboratory. Dr. Saltzman is also the co-founder and chief medical officer of Salspera. Salspera is a biotechnology company centered around bacterial based immunotherapeutics and hold the patents for Salmonella-IL2. This conflict has been extensively disclosed and is managed by the Office of Conflict Administration at the University of Minnesota.
Dr. Eddie Moradian is the co-founder and CEO of Salspera.
Mr. Jordan Moradian is a content expert in biostatistics and is a consultant for Salspera.
References
2. Mizrahi JD, Surana R, Valle JW, Shroff RT. Pancreatic cancer. Lancet. 2020 Jun 27;395(10242):2008–20.
3. Klein-Brill A, Amar-Farkash S, Lawrence G, Collisson EA, Aran D. Comparison of FOLFIRINOX vs Gemcitabine Plus Nab-Paclitaxel as First-Line Chemotherapy for Metastatic Pancreatic Ductal Adenocarcinoma. JAMA Netw Open. 2022 Jun 1;5(6):e2216199.
4. Nichetti F, Rota S, Ambrosini P, Pircher C, Gusmaroli E, Droz Dit Busset M, et al. NALIRIFOX, FOLFIRINOX, and Gemcitabine with Nab-Paclitaxel as First-Line Chemotherapy for Metastatic Pancreatic Cancer: A Systematic Review and Meta-Analysis. JAMA Netw Open. 2024;7(1):e2350756.
5. Cereda V, D'Andrea MR. Pancreatic cancer: failures and hopes-a review of new promising treatment approaches. Explor Target Antitumor Ther. 2025 Mar 18;6:1002299.
6. Forbes NS, Coffin RS, Deng L, Evgin L, Fiering S, Giacalone M, et al. White paper on microbial anti-cancer therapy and prevention. J Immunother Cancer. 2018 Aug 6;6(1):78.
7. Duong MT, Qin Y, You SH, Min JJ. Bacteria-cancer interactions: bacteria-based cancer therapy. Exp Mol Med. 2019 Dec 11;51(12):1–15.
8. Saltzman DA, Heise CP, Hasz DE, Zebede M, Kelly SM, Curtiss R 3rd, et al. Attenuated Salmonella typhimurium containing interleukin-2 decreases MC-38 hepatic metastases: a novel anti-tumor agent. Cancer Biother Radiopharm. 1996 Apr;11(2):145–53.
9. Saltzman DA, Katsanis E, Heise CP, Hasz DE, Vigdorovich V, Kelly SM, et al. Antitumor mechanisms of attenuated Salmonella typhimurium containing the gene for human interleukin-2: a novel antitumor agent? J Pediatr Surg. 1997 Feb;32(2):301–6.
10. Saltzman DA, Katsanis E, Heise CP, Hasz DE, Kelly SM, Curtiss R 3rd, et al. Patterns of hepatic and splenic colonization by an attenuated strain of Salmonella typhimurium containing the gene for human interleukin-2: a novel anti-tumor agent. Cancer Biother Radiopharm. 1997 Feb;12(1):37–45.
11. Soto LJ, Sorenson BS, Nelson BW, Leonard AS, Saltzman DA. Generation of immunity to hepatic metastases by attenuated Salmonella typhimurium. Ann Surg Onc. 2004;11(2)suppl: S107.
12. Soto LJ 3rd, Sorenson BS, Kim AS, Feltis BA, Leonard AS, Saltzman DA. Attenuated Salmonella typhimurium prevents the establishment of unresectable hepatic metastases and improves survival in a murine model. J Pediatr Surg. 2003 Jul;38(7):1075–9.
13. Soto LJ 3rd, Sorenson BS, Nelson BW, Solis SJ, Leonard AS, Saltzman DA. Preferential proliferation of attenuated Salmonella typhimurium within neuroblastoma. J Pediatr Surg. 2004 Jun;39(6):937–40.
14. Barnett SJ, Soto LJ 3rd, Sorenson BS, Nelson BW, Leonard AS, Saltzman DA. Attenuated Salmonella typhimurium invades and decreases tumor burden in neuroblastoma. J Pediatr Surg. 2005 Jun;40(6):993–7.
15. Sorenson BS, Banton KL, Frykman NL, Leonard AS, Saltzman DA. Attenuated Salmonella typhimurium with IL-2 gene reduces pulmonary metastases in murine osteosarcoma. Clin Orthop Relat Res. 2008 Jun;466(6):1285–91.
16. Fritz SE, Henson MS, Greengard E, Winter AL, Stuebner KM, Yoon U, et al. A phase I clinical study to evaluate safety of orally administered, genetically engineered Salmonella enterica serovar Typhimurium for canine osteosarcoma. Vet Med Sci. 2016 Jun 6;2(3):179–90.
17. Gniadek TJ, Augustin L, Schottel J, Leonard A, Saltzman D, Greeno E, et al. A Phase I, Dose Escalation, Single Dose Trial of Oral Attenuated Salmonella typhimurium Containing Human IL-2 in Patients With Metastatic Gastrointestinal Cancers. J Immunother. 2020 Sep;43(7):217–21.
18. Saltzman D, Kavan P, Augustin L, Schottel J, Lee JT, Moradian J, et al. Influence of salmonella-IL2 in combination with FOLFIRINOX on overall and progression-free survival in stage IV metastatic pancreatic cancer. J Clin Oncol. 2025 may; 43:2571.
19. Batist G, Kavan P, Augustin L, Schottel J, Moradian J, Lee JT, et al. A phase 2 study of orally administered live biotherapeutic salmonella-IL2 with FOLFIRINOX for stage IV pancreatic cancer. Cancer Immunol Immunother. 2026 Jan 27;75(2):60.
20. Revolution Medicines. Daraxonrasib demonstrates unprecedented overall survival benefit in RASolute 302 Phase 3 trial in previously treated patients with KRAS G12C-positive non-small cell lung cancer [Internet]. Redwood City (CA): Revolution Medicines; 2025. Available from: https://ir.revmed.com/news-releases/news-release-details/daraxonrasib-demonstrates-unprecedented-overall-survival-benefit
21. Eisenhauer EA, Therasse P, Bogaerts J, Schwartz LH, Sargent D, Ford R, et al. New response evaluation criteria in solid tumours: revised RECIST guideline (version 1.1). Eur J Cancer. 2009 Jan;45(2):228–47.
22. https://ctep.cancer.gov/protocoldevelopment/electronic_applications/docs/aeguidelines.pdf
23. World Medical Association. WMA Declaration of Helsinki – ethical principles for medical research involving human subjects [Internet]. Ferney-Voltaire: World Medical Association. Available from: https://www.wma.net/policies-post/wma-declaration-of-helsinki/
24. Marion JD, Althouse AD. The Use of Historical Controls in Clinical Trials. JAMA. 2023 Oct 17;330(15):1484–5.