Abstract
Objective: To evaluate the position and angulation of impacted maxillary canines in unilateral and bilateral cleft lip and palate cases and compare them to noncleft cases.
Material and method: In this study 60 patients OPGs were taken out of which 20 (12 males, 8 females) presented with unilateral cleft lip and palate (UCLP) (Group I), 20 (15 males, 5 females) had bilateral cleft lip and palate (BCLP) (Group II) and 20 (13 males, 7 females) had no clefts (Group III). All the subjects had impacted maxillary canines (bilateral or unilateral). Cases with 2/3rd canine root completion were selected. Intruis suite R2 software was used to determine the position and angulation of the canine.
Results: A total of 63% (37) of the canines were in Sector 1, and 31% (18) were in Sector 2. In-depth of canine impaction relative to the root of the incisor maximum canines were in Grade II and Grade III at 45% (27) and 36% (22) respectively. Angulation of the canine relative to the intercondylar line was seen most in Group II (75%) and (19%) in Group I as compared to the noncleft group (Group III). No difference was seen in the position of canine impaction for buccally and palatally canines and for the unilateral and bilateral cleft groups or the noncleft and cleft groups.
Conclusions: The majority of the impacted canines had cusp tips located in sectors II and III. In almost all cases, angulation did not increase the prediction of eventual impaction, although it may have contributed slightly in Sector II.
Keywords
Impacted canine, Sector classification, Cleft palate
Introduction
A normally developed tooth that cannot erupt in the maxillary or mandibular dentition after its normal eruption age is likely to be an impacted tooth. Radiographic confirmation suggests that it will not erupt in its dental arch [1]. The most commonly impacted teeth are the mandibular third molars followed by permanent maxillary canines. Langberg quoted “no tooth is more interesting from a developmental point of view than the maxillary canine” [2]. Maxillary permanent canines are the last teeth to erupt in the anterior segment, the maxillary third molars are the last to erupt in the maxillary arch. They have a long route to travel from their bud formation until their eruption to the final position in the maxillary dentition [3]. Studying the 3-dimensional course of the eruption, Coulter and Richardson found that the permanent maxillary canine has to travel approximately 22 mm until its eruption in the dental arch [4]. Several factors during the eruption of maxillary permanent canines, such as mechanical, genetic, early loss of deciduous teeth and environmental factors, influence the eruption pathway of the canine. Thus, any disturbance in these factors may cause displacement of the developing permanent maxillary canines, resulting in its impaction.
The supporting bone of the alveolar process that holds the teeth has a major influence on the eruption of all the teeth, and its absence is a factor commonly associated with impacted teeth, especially, permanent maxillary canines. Impacted teeth are most commonly seen in syndromes such as Cleidocranial dysplasia, Gardner syndrome, Apert syndrome, Cleft lip, and palate. Most cases of impacted canines are reported in Cleft lip Palate patients [5]. A higher frequency of dental anomalies has been reported in cleft patients than in healthy patients [6]. Dental anomalies such as rotated teeth, supernumerary teeth, and impacted teeth are also frequently seen [7]. Additionally, agenesis of teeth, and peg-shaped maxillary lateral incisors have been reported in the literature [8]. The partial reduction in the space for the eruption of maxillary permanent canines might be due to the closure of the alveolus with Early Secondary Gingivo Alveoloplasty (ESGAP), as there is less bone available for the eruption of the canine. The available bone is utilized by the erupting teeth, and therefore, there is an increase in the percentage of impacted teeth [9].
The genetic factor associated with the prevalence of cleft lip and palate CLP and the higher incidence of palatally impacted canines might be due to the collapse of the palatal maxillary lateral segment [10,11].
Maxillary permanent canines that develop mesial or distal to the primary canines tend to erupt abnormally. The decision of surgically exposing the impacted maxillary canines in the arch and aligning it or just to remove the impacted canine mainly depends on radiographic findings, extent, and position of the canine [12,13].
A classification system needs to grade determine the severity of palatal impacted canines and should be based on radiographs. Highly placed canines having severely transposed roots generally have the most unfavorable prognosis [14-16]. The angulation of the canine long axis to the skeletal midline, the anteroposterior position of the canine root apex relative to the midline, the vertical position of the canine crown from the occlusal plane, and the degree of overlap of the adjacent incisor by the canine crown tip are the main four radiographic predictors of determining prognosis for the exposure of impacted permanent maxillary canines and its alignment in the arch [17,18].
Hereman et al. [19] stated that there is a great risk for canine impaction in UCLP patients when the canine position is more apical than one-third of the root of the adjacent lateral incisor. Ericson and Kurol [20] mentioned that patients with alveolar clefts have a higher risk for canine impaction than patients without clefts. The position of the impacted canines in cleft palate patients’ needs to be evaluated to assess the prognosis of the same because they are an important feature of facial aesthetics. Hence, this study was performed to compare and evaluate the angulation as well as the position of impacted permanent maxillary canines in unilateral and bilateral cleft lip and palate cases.
Material and Methods
A total of 60 CLP patients with OPG’s of the impacted maxillary permanent canines were selected by convenience sampling for the cross-sectional study. These patients had come to the hospital for treatment of cleft lip and palate. The ones which fitted in the inclusion criteria were selected for the study. Power analysis was done for calculating the sample size. The mean age was 14.01 ± 2 years, and they were of Indo-Aryan origin. A total of 3 groups were established - 20 patients had unilateral cleft lip and palate (Group I), 20 had bilateral CLP (Group II), and the third group of 20 had no clefts (Group III). Most of the patients had a skeletal Class III malocclusion due to the deficient maxilla. The median anterior cleft size was 5.3 mm ± 2.3 mm for Group I and II. Group III (control) was without any clefts. The medial wall of the cleft segment was retro positioned and displaced laterally. The anterior/incisor portion of the noncleft segment was anteriorly displaced. Cleft alveoli were turned superiorly. Nasal deformity was observed in a few patients with bilateral cleft lip and palate. No orthodontic treatment was performed before the cleft lip and palate surgery. Closure of the cleft was performed using Bardach two-flap palatoplasty, in a two-stage operation (soft palate at 3 months, then lip and hard palate at 6 months) for all cleft patients [21]. This study was presented before and approved by the Institutional Ethical Committee, and the data collection was done after obtaining informed consent for each subject taken from their parents.
Inclusion criteria
- Maxillary permanent first molars and maxillary permanent lateral incisors erupted completely,
- Impacted permanent maxillary canines,
- Secondary bone grafting is done with freeze-dried bone allografts to correct the defect (at age 11-13).
- Root formation - 2/3rd of the permanent maxillary canine was completed.
Keeping the same exposure and magnification parameters, all OPGs were taken 6 months post-secondary bone grafting (kVp ? 72, mA ? 8 exposure time 18 s & Kodak 8000C Digital and Panoramic System Cephalometer Rochester, NY, USA). A Quad Helix appliance was used for expanding the maxillary arch, and thereafter, the position of the canines was determined for the cases. The study included both buccally and palatally impacted maxillary permanent canines. For correct landmark identification, the condyles bilaterally were distinguished clearly in the OPG, and using the Intruis suite R2 software (Philips Eindhoven) and the canine region on the OPG was analyzed.
The impacted canines were evaluated by sector classification, degree of overlap of the adjacent incisor by the canine crown tip, the vertical position of the canine crown from the occlusal plane, & angulation of the canine’s long axis to the intercondylar line. The superior most point on the condyle was marked in all OPGs. A line joining both points on the condyle was used as the horizontal constructed reference line. The mesial angle formed by using the constructed horizontal and the long axis of the impacted canine was noted (Figure 1). Depending on the measurement of the angle formed, they were placed in either of the three categories, 0- 15 degrees, 15-30 degrees, ≥ 30 degrees.
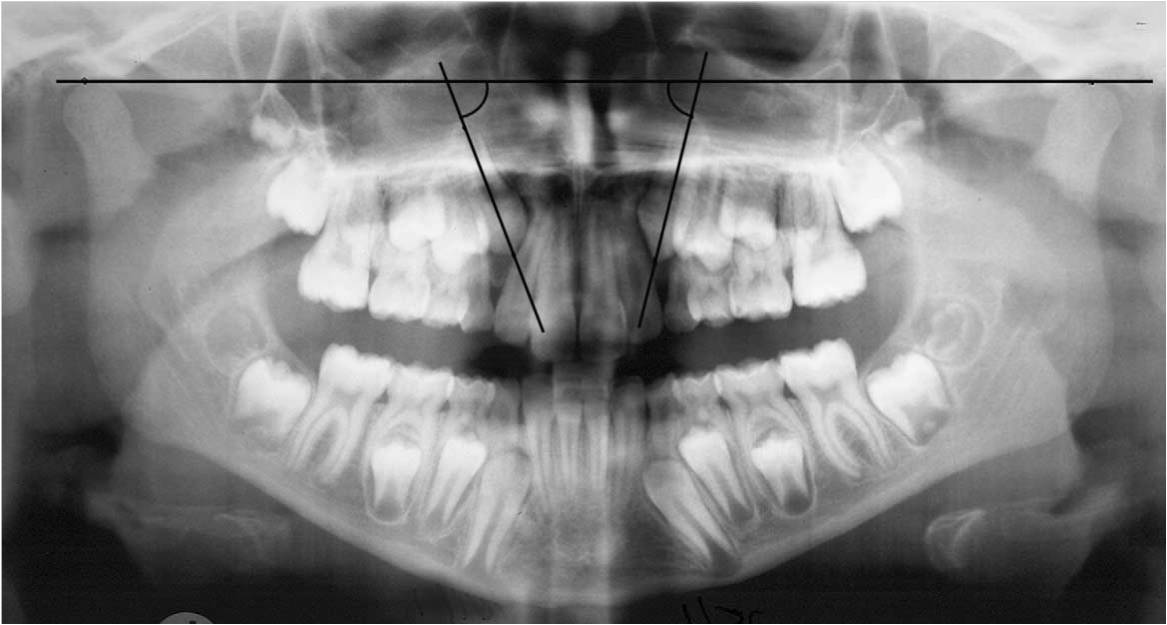
Figure 1. Angular measurement of impacted canines.
For the unerupted canines, the cusp tip was marked and located in the same manner as the sector delineation used by Ericson and Kurol (Table 1, Figure 2) [22].
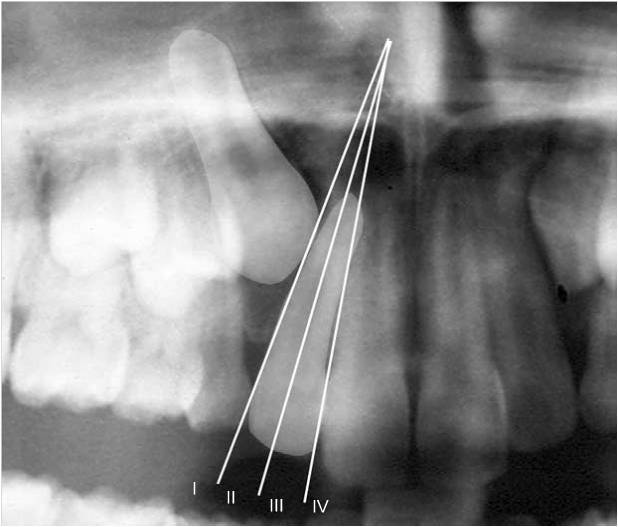
Figure 2. Modification of Ericson and Kurol’s sector classification.
|
Sector 1 |
The area distal to a line drawn which is tangent to the height of contour of lateral incisor crown and root on the distal aspect |
|
Sector 2 |
Mesial to the sector I, but distal to the bisector of lateral incisor’s long axis. |
|
Sector 3 |
Mesial to sector II, but distal to mesial heights of the contour of lateral incisor crown and root. |
|
Sector 4 |
It includes all areas mesial to sector III. |
The depth of impaction of the canine relative to the root of the incisor was measured and graded as follows (Figure 3) -
Grade I: Below the level of the cementoenamel junction (CEJ).
Grade II: Above the CEJ, but less than halfway up the root.
Grade III: More than halfway up the root, but less than the full root length.
Grade IV: Above the full length of the root
All the readings and gradings were grouped accordingly. A master chart Excel sheet with all the above readings from the obtained data was tabulated and subjected to statistics. The same examiner measured all the readings and grading, so the need for inter-examiner reliability was not required.
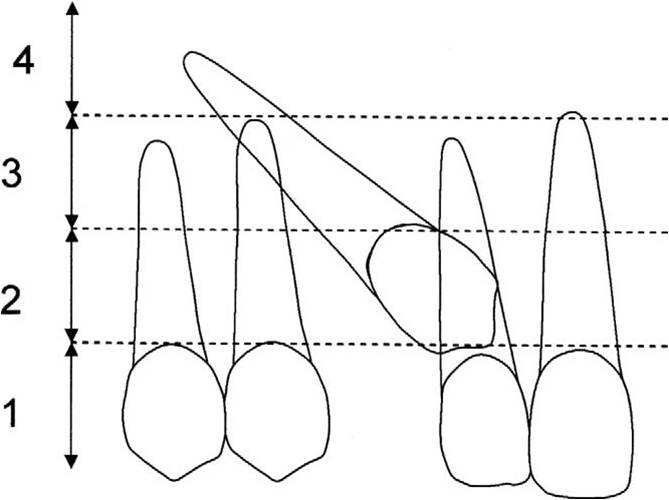
Figure 3. Depth of impaction of the canine relative to the root of the incisor.
Results
The results obtained showed that, 37 patients (63%) had their canines in Sector I, 18 patients (31%) in Sector II, and 5 (6%) in Sector III (Figure 4). Concerning the depth of canine impaction relative to the root of lateral incisors, most of the canines were Grade II (33), 56%, followed by Grade III (21), 36% with 8% in Grade I and 0% in Grae IV (Figure 5). Group II (BCLP) recorded the highest readings for angulation of the canine relative to the intercondylar line 75%, Group I recorded 19%, while Group III had 6% (Figure 6). The position of impacted canines in unilateral and bilateral cleft groups as well as between cleft and the non-cleft group remained more or less similar in each group, as there was no statistically significant difference seen. Intergroup comparisons were performed, and no statistically significant difference was seen.
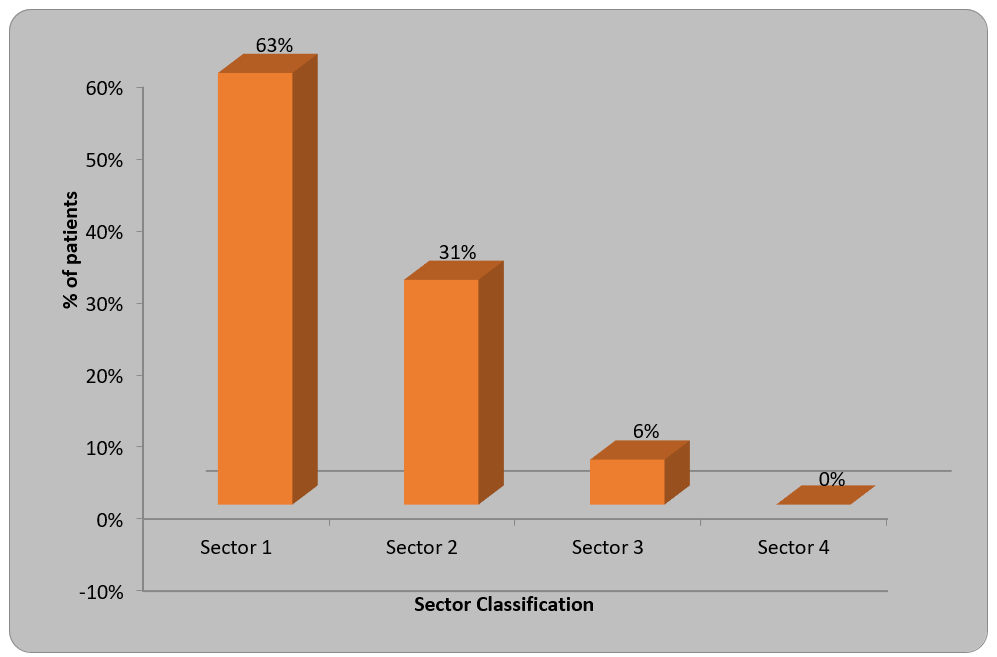
Figure 4. Sector classification to assess the position of the canine.
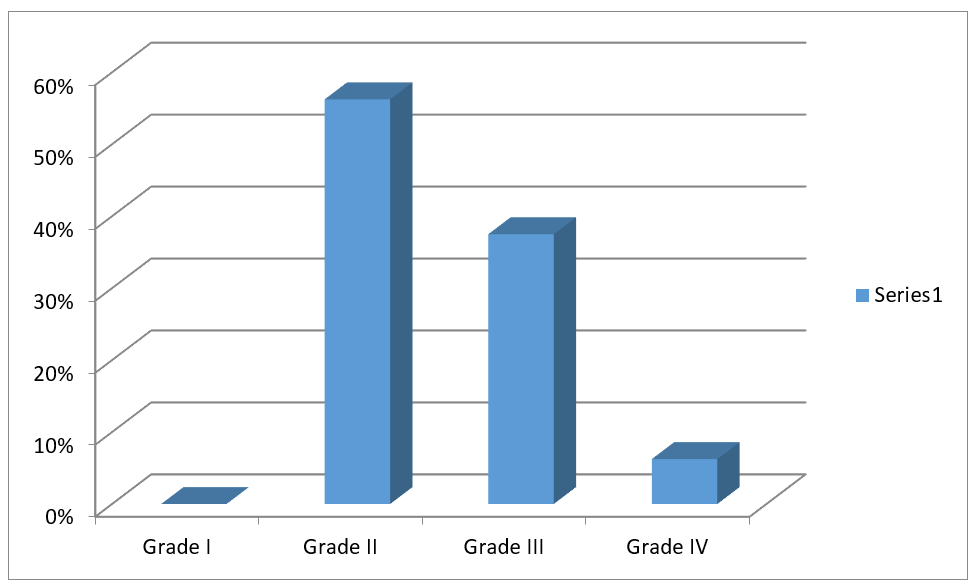
Figure 5. Depth of impaction of canine relative to the root of incisor was measured.
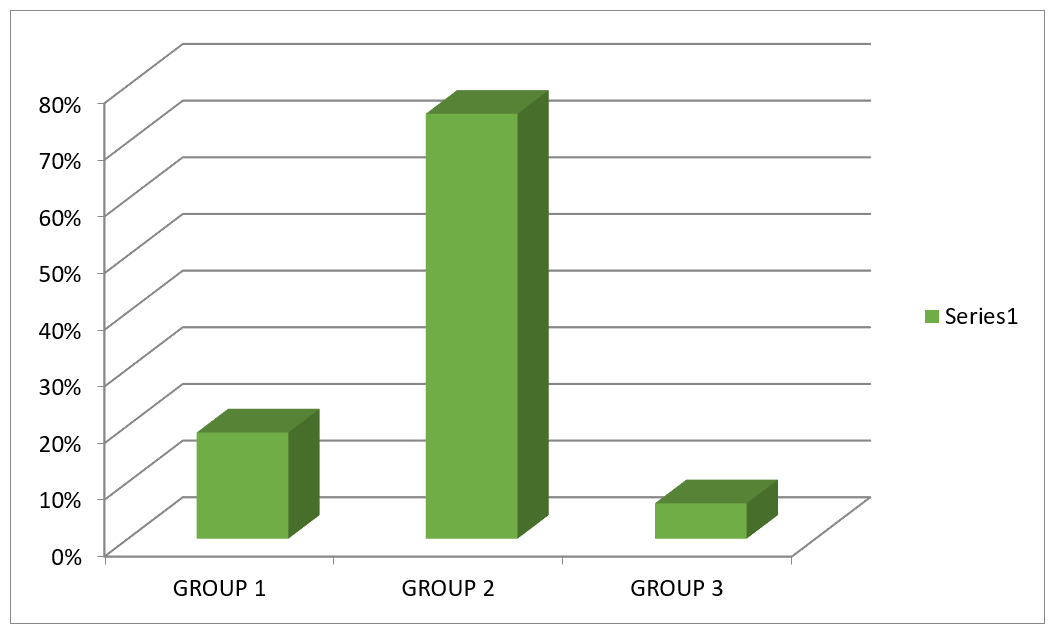
Figure 6. Angular measurement of impacted canines.
Discussion
Cleft lip and palate (CLP) are a known congenital deformity associated with skeletal and dental abnormalities [23,24]. Along with skeletal deformities, numerous dental anomalies, such as congenitally missing teeth, supernumerary teeth, hypodontia, hyperdontia, transpositions, impaction, and deformities in enamel formation are also observed [25-28]. Thirty-seven out of 60 (63%) patients showed impacted canines in sector I, 18 (31%) were seen in sector II, and 5 (6%) in sector III. In 30 patients, the canines were present in the area distal to a line tangent to distal heights of the contour of lateral incisor crown and root, in 20 patients, it was distal to the bisector of the lateral incisor’s long axis, and in 10 patients, it was distal to mesial heights of the contour of lateral incisor crown and root.
Studies documented by Vichi and Franchi stated that if lateral incisors are congenitally missing, there is an increased risk of maxillary permanent canines being impacted. Moreover, agenesis, microdontic form, and the mesial position of the lateral incisors related to the cleft area are also found to be associated with malposition of the permanent maxillary canine [29]. Powers and Short [30] studied angulations as a predictor and reported that if the tooth is angulated 31° or more to the skeletal midline, there are increased chances of impaction after deciduous canine extraction. In our study, the angulation of the canine relative to the intercondylar line was assessed, as many patients had a deviated skeletal midline due to CLP. The angulation of the canine relative to the intercondylar line was maximum in Group II (75%), and Group I had (19%) of the sample size. Therefore, most of the cleft cases had 15-30 degrees of canine angulation, which can be favorably brought in occlusion [31-33].
Ericson and Kurol [20] stated that the chances of canine erupting normally are 91% if the cusp tip of the impacted maxillary canine does not cross the dental midline of the adjacent lateral incisor. Chances of canine erupting normally drop to 64% if the cusp tip crosses the midline of the lateral incisor. The findings revealed that the deeper the cusp tip from the occlusal plane, the greater the chance of tooth impaction and the greater the amount of time required to bring in to normal occlusion. In our study, the maximum percentage of canine impaction evaluating the depth of canine impaction relative to the root of the incisor was found in grade II - 56% (33) and grade III 36% (22). To conclude this, there is a 56% chance of bringing the impacted canine in occlusion, if it is presented above the CEJ but less than halfway up the root by surgical exposure and orthodontic treatment in CLP cases.
Emergence of three-dimensional imaging techniques and improvements over conventional radiological imaging has helped clinicians worldwide. Accuracy in routine diagnosis has been seen not only in the head and neck region but also in other areas of the body where radiation hygiene is much more important [33]. Need for special attention to limit radiation exposure in younger patients, e.g., those with cleft lip and palate, should be considered. This is in contrast to the objective of obtaining precise and detailed imaging in the region of the osseous cleft defect, the teeth, and the tooth germs, especially in orthodontic planning and other surgical operations such as osteoplasty. Some limitations of the study were that larger sample sizes may be able to confirm these above findings along with the role of angulation in predicting maxillary canine impaction. Accurate measurement of position and angulation is beneficial in determining the proximity of the root of the adjacent incisor and premolar. This can be valuable in determining the ease of uncovering and bonding the canine along with determining the force vector that can be used to move the tooth into the arch with a lesser chance of adjacent root resorption and prognosis.
Conclusions
- In this study, 63% of the impacted canines had cusp tips located in sector I and 31% in sector II.
- If the cusp tip is located in sector III, the prediction of eventual impaction is high, based on sector alone.
- In almost all cases, angulation did not increase the prediction of eventual impaction, although it may contribute slightly in sector II.
- Despite promising results, the outcomes of this study should be taken as suggestive only and certainly not absolute.
References
2. Langberg BJ, Peck S. Adequacy of maxillary dental arch width in patients with palatally displaced canines. Am J Orthod Dentofacial Orthop 2000; 118: 220-23.
3. Parenti SI, Gatto MR, Gracco A, Bonetti GA. Reliability of different methods for measuring the inclination of the maxillary canines on panoramic radiographs. Orthod Craniofac Res 2013; 16:177-8.
4. Coulter J, Richardson A. Normal eruption of the maxillary canine quantified in three dimensions. European Journal of orthodontics. 1997 Apr 1;19(2):171-83.
5. Shapira Y, Kuftinec MM. Early diagnosis and interception of potential maxillary canine impaction. The Journal of the American Dental Association. 1998 Oct 1;129(10):1450-4.
6. Holz IS, Carvalho RM, Lauris JR, Lindauer SJ, Garib DG. Permanent canine eruption into the alveolar cleft region after secondary alveolar bone grafting: are there prediction factors for impaction?. American Journal of Orthodontics and Dentofacial Orthopedics. 2018 Nov 1;154(5):657-63.
7. Jordon RE, Kraus BS, Neptune CM. Dental abnormalities associated with cleft lip and/or palate. Plastic and Reconstructive Surgery. 1966 Aug 1;38(2):172.
8. Schroeder DC, Green LJ. Frequency of dental trait anomalies in cleft, sibling, and noncleft groups. Journal of dental research. 1975 Jul;54(4):802-7.
9. Olin WH. Dental anomalies in cleft lip and palate patients. The Angle Orthodontist. 1964 Apr;34(2):119-23.
10. Westerlund A, Sjöström M, Björnström L, Ransjö M. What factors are associated with impacted canines in cleft patients?. Journal of Oral and Maxillofacial Surgery. 2014 Nov 1;72(11):2109-14.
11. Kraus BS, Jordan RE, Pruzansky S. Dental abnormalities in the deciduous and permanent dentitions of individuals with cleft lip and palate. Journal of Dental Research. 1966 Nov;45(6):1736-46.
12. Dempf R, Teltzrow T, Kramer FJ, Hausamen JE. Alveolar bone grafting in patients with complete clefts: a comparative study between secondary and tertiary bone grafting. The Cleft Palate-craniofacial Journal. 2002 Jan;39(1):18-25.
13. Hogan L, Shand JM, Heggie AA, Kilpatrick N. Canine eruption into grafted alveolar clefts: a retrospective study. Australian Dental Journal. 2003 Jun;48(2):119-24.
14. Suzuki A, Watanabe M, Nakano M, Takahama Y. Maxillary lateral incisors of subjects with cleft lip and/or palate: Part 2. The Cleft Palate-craniofacial Journal. 1992 Jul;29(4):380-4.
15. Shapira Y, Lubit E, Kuftinec MM. Hypodontia in children with various types of clefts. The Angle Orthodontist. 2000 Feb;70(1):16-21.
16. Aizenbud D, Camasuvi S, Peled M, Brin I. Congenitally missing teeth in the Israeli cleft population. The Cleft Palate-craniofacial Journal. 2005 May;42(3):314-7.
17. Oberoi S, Gill P, Chigurupati R, Hoffman WY, Hatcher DC, Vargervik K. Three-dimensional assessment of the eruption path of the canine in individuals with bone-grafted alveolar clefts using cone beam computed tomography. The Cleft Palate-craniofacial Journal. 2010 Sep;47(5):507-12.
18. Hereman V, Cadenas De Llano-Pérula M, Willems G, Coucke W, Wyatt J, Verdonck A. Associated parameters of canine impaction in patients with unilateral cleft lip and palate after secondary alveolar bone grafting: a retrospective study. European Journal of Orthodontics. 2018 Nov 30;40(6):575-82.
19. Russell KA, McLeod CE. Canine eruption in patients with complete cleft lip and palate. The Cleft Palate-Craniofacial Journal. 2008 Jan;45(1):73-80.
20. Ericson S, Kurol J. Radiographic examination of ectopically erupting maxillary canines. American Journal of Orthodontics and Dentofacial Orthopedics. 1987 Jun 1;91(6):483-92.
21. Bardach J. Two-flap palatoplasty: Bardach's technique. Operative techniques in plastic and reconstructive surgery. 1995 Nov 1;2(4):211-4.
22. Tortora C, Meazzini MC, Garattini G, Brusati R. Prevalence of abnormalities in dental structure, position, and eruption pattern in a population of unilateral and bilateral cleft lip and palate patients. The Cleft Palate-Craniofacial Journal. 2008 Mar;45(2):154-62.
23. Paulin G, Åstrand P, Rosenquist JB, Bartholdson L. Intermediate bone grafting of alveolar clefts. Journal of Cranio-Maxillofacial Surgery. 1988 Jan 1;16:2-7.
24. Matsui K, Echigo S, Kimizuka S, Takahashi M, Chiba M. Clinical study on eruption of permanent canines after secondary alveolar bone grafting. The Cleft Palate-craniofacial Journal. 2005 May;42(3):309-13.
25. Amanat N, Langdon JD. Secondary alveolar bone grafting in clefts of the lip and palate. Journal of Cranio-Maxillofacial Surgery. 1991 Jan 1;19(1):7-14.
26. McCanny CM, Roberts-Harry DP. A comparison of two different bone-harvesting techniques for secondary alveolar bone grafting in patients with cleft lip and palate. The Cleft Palate-craniofacial Journal. 1998 Sep;35(5):442-6.
27. Russell KA, McLeod CE. Canine eruption in patients with complete cleft lip and palate. The Cleft Palate-Craniofacial Journal. 2008 Jan;45(1):73-80.
28. Vichi M, Franchi L. Abnormalities of the maxillary incisors in children with cleft lip and palate. ASDC Journal of Dentistry for Children. 1995 Nov 1;62(6):412-7.
29. Power SM, Short MB. An investigation into the response of palatally displaced canines to the removal of deciduous canines and an assessment of factors contributing to favourable eruption. British Journal of Orthodontics. 1993 Aug;20(3):215-23.
30. Van der Meij AJ, Baart JA, Prahl-Andersen B, Valk J, Kostense PJ, Tuinzing DB. Bone volume after secondary bone grafting in unilateral and bilateral clefts determined by computed tomography scans. Oral Surgery, Oral Medicine, Oral Pathology, Oral Radiology, and Endodontology. 2001 Aug 1;92(2):136-41.
31. Jia Y, Fu M, Ma L. The comparison of two-dimensional and three-dimensional methods in the evaluation of the secondary alveolar bone grafting. Zhonghua kou Qiang yi xue za zhi= Zhonghua Kouqiang Yixue Zazhi= Chinese Journal of Stomatology. 2002 May 1;37(3):194-6.
32. Dado DV, Rosenstein SW, Alder ME, Kernahan DA. Long-term assessment of early alveolar bone grafts using three-dimensional computer-assisted tomography: a pilot study. Plastic and Reconstructive Surgery. 1997 Jun 1;99(7):1840-5.