Abstract
Introduction: Plasma donation is generally considered a safe procedure, and most reported adverse events are related to venipuncture or transient volume loss. Arterial thrombotic events, including acute myocardial infarction, are exceedingly rare but have been described after source plasma donation performed by plasmapheresis. We report a young man without traditional cardiovascular risk factors who presented with acute ST-elevation myocardial infarction after plasma donation.
Case presentation: A 27-year-old man with eczema and intermittent cannabis use presented with chest pain approximately 12 hours after plasma donation. Electrocardiography demonstrated anterolateral ST-segment elevation, and coronary angiography showed a large proximal left anterior descending (LAD) artery thrombus with TIMI 1 flow. Aspiration thrombectomy restored TIMI 3 flow, although residual stenosis persisted. A repeat angiogram performed two days later showed persistent proximal LAD thrombus. When the patient returned several days later for completion of the evaluation, repeat angiography demonstrated a contained proximal LAD dissection without residual thrombus; based on the initial angiographic appearance and interval development after thrombectomy, this finding was considered most consistent with a procedural complication rather than the primary cause of presentation. Transthoracic echocardiography showed new severe left ventricular systolic dysfunction with an ejection fraction of 20%–25% and extensive apical akinesis.
Conclusion: Plasma donation may rarely be followed by arterial thrombosis, including ST-elevation myocardial infarction. In this case, plasma donation was considered a plausible trigger for coronary thrombosis, while cannabis use represented a potential additional contributing factor. Persistent ischemic symptoms after donation warrant prompt evaluation for acute coronary syndrome.
Keywords
Cardiovascular Therapeutics, Coronary artery disease, Coronary thrombosis, STEMI
Introduction
Plasma donation (PD) is generally safe, with reported adverse events that are most commonly limited to bruising, vasovagal episodes, puncture-site pain, and hematoma formation [1,2]. Risk factors for donation-related adverse events include low body mass index (BMI), younger age, first-time donor status, and female sex [1]. The demand for plasma-derived medicinal products has increased steadily in recent years, which has renewed interest in donor safety and the rare but potentially serious complications of source plasma donation performed by plasmapheresis [3]. Older American Red Cross hemovigilance data from 2006 reported no acute myocardial infarctions after donation [4], while more contemporary plasmavigilance data continue to show that hypotensive and phlebotomy-related events predominate [1]. Nevertheless, arterial thrombosis has been described after plasma donation. Proposed mechanisms include transient platelet activation, reductions in endogenous anticoagulant proteins, changes in coagulation factor activity, and vasospasm related to hypovolemia or citrate-associated reactions [2,5]. We report a case of acute ST-elevation myocardial infarction (STEMI) due to a proximal left anterior descending artery thrombus shortly after plasma donation.
Case Presentation
History of presenting illness
A 27-year-old man with eczema and a history of intermittent cannabis use presented from an outside hospital with left-sided, pressure-like, non-radiating chest pain that began the evening before admission. He reported that the only notable recent event was plasma donation approximately 12 hours before symptom onset; he had donated plasma several times previously without complication. He denied prior cardiac disease, stroke, venous thromboembolism, or a family history of premature coronary artery disease or thrombophilia. The frequency, route, and recency of cannabis use were not reliably documented in the available records, which is acknowledged as a limitation.
Investigations and management
At the outside hospital, the patient was hemodynamically stable, and the initial electrocardiogram (ECG) showed anterolateral ST-segment elevation concerning for STEMI. He was therefore transferred to a percutaneous coronary intervention-capable facility. Repeat ECG on arrival demonstrated ST-segment elevation in leads II, III, aVF, and V2–V6 (Figure 1). High-sensitivity troponin was elevated to 1,130 pg/mL, and the patient underwent emergent coronary angiography. Angiography demonstrated a large filling defect in the proximal left anterior descending artery (pLAD), consistent with thrombus, with TIMI 1 flow (Figure 2). Aspiration thrombectomy was partially successful, leaving residual stenosis but restoring TIMI 3 flow. The patient was treated with aspirin, ticagrelor, atorvastatin, and a tirofiban infusion for 24 hours because of the heavy thrombus burden.
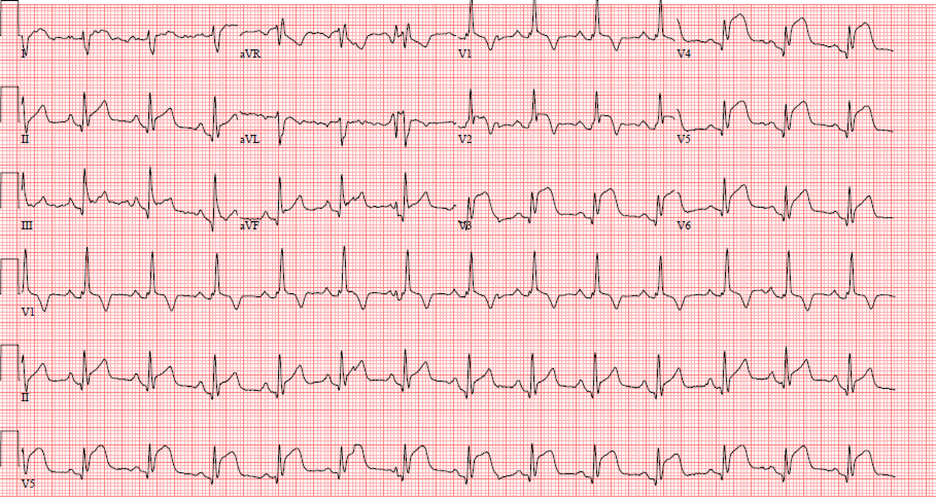
Figure 1. EKG showing ST elevations in leads II, III, aVF, V2–V6.
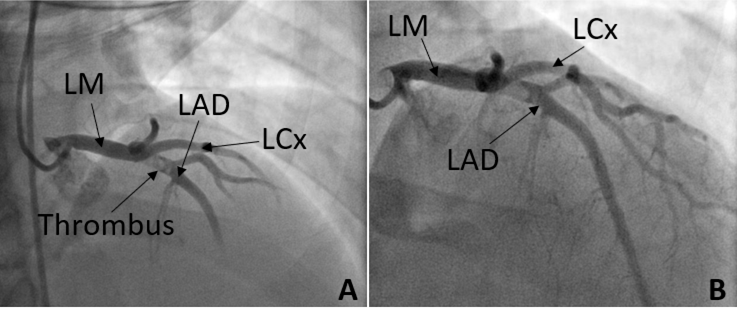
Figure 2. A. Left Heart Catheterization showing LAD with presence of thrombus in the proximal segment. B. Left Heart Catheterization showing LAD immediately after aspiration thrombectomy and intracoronary adenosine administration.
A repeat coronary angiogram performed two days later showed persistent pLAD thrombus. No additional intervention was performed at that time and repeat angiography with intravascular ultrasound was planned. Transthoracic echocardiography showed new severe left ventricular systolic and diastolic dysfunction with an ejection fraction of 20%–25%, grade II diastolic dysfunction, and akinesis of the apical anterior, apical inferior, apical septal, apical lateral, and apical segments. Before the next planned angiogram, however, the patient left the hospital against medical advice after the risks had been explained.
Several days later, the patient returned to the emergency department to complete the evaluation. He reported only one brief episode of chest pain at rest and acknowledged that he had not been taking his medications consistently. Repeat coronary angiography demonstrated a contained pLAD dissection without residual thrombus (Figure 3). Given the initial angiographic appearance of an occlusive thrombus, the interval resolution of thrombus, and the new appearance of the dissection after thrombectomy, the contained dissection was considered most consistent with an iatrogenic complication of the prior intervention rather than the primary etiology of the index event. No further coronary intervention was performed. The patient again elected to leave against medical advice and was instructed to continue guideline-directed medical therapy for coronary artery disease and heart failure with reduced ejection fraction.
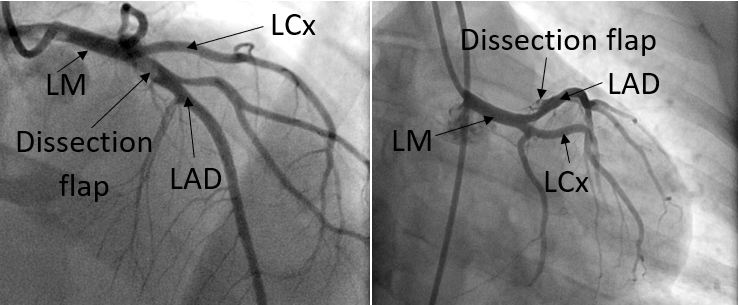
Figure 3. Coronary angiogram one week after initial thrombectomy, showing a dissection flap in proximal LAD from two views.
Discussion
Plasma-derived medicinal products are used in the treatment of immune deficiencies, bleeding disorders, neurologic diseases, liver disease, refractory hyperlipidemia, and other conditions; as a result, the use of source plasma donation has increased substantially [3]. Source plasma donation is performed by plasmapheresis, a selective extracorporeal process in which plasma is removed, and the cellular blood components are returned to the donor. Accordingly, the mechanistic literature on plasmapheresis is relevant to plasma donation in this case. Most adverse effects are minor and include venipuncture-site trauma, vasovagal reactions, and transient hypotension, whereas severe complications are rare [1,2,6]. In the 2021 Plasmavigilance study, which evaluated 1.1 million donors and more than 12 million donations over 4 months, hypotensive and phlebotomy-related events were the most frequent adverse events [1]. Similarly, the 2012–2014 AABB Donor Hemovigilance Report, based on 2,487,392 donations, did not identify arterial thrombosis as a commonly reported complication [7].
Several mechanisms have been proposed to explain a transient prothrombotic state after plasmapheresis and plasma donation. Exposure of blood to artificial surfaces and centrifugation may alter coagulation pathways and platelet activity. Prior reports have described increased activity of coagulation factors I, II, V, VII, IX, and X; reduced levels of protein C, plasminogen, and antithrombin III; and prolonged circulation of activated platelets after apheresis [5,8,9]. In one study, comparison of pre-donation and post-donation samples in healthy donors suggested a shift toward hypercoagulability after plasmapheresis [5]. A second proposed mechanism is vasospasm triggered by hypovolemia, vasovagal responses, or citrate-related symptoms [2,5].
The risk of arterial thrombosis may be higher in individuals with inherited or acquired thrombophilia. Large-volume donor plasmapheresis has previously been implicated in arterial thrombosis in donors with thrombophilic predisposition [10]. Although universal thrombophilia screening is unlikely to be cost-effective, these reports suggest that donation-related hemostatic perturbations may unmask pre-existing susceptibility in selected patients.
Acute myocardial infarction after plasma donation has been described in a small number of case reports [11–13]. Reported patients were predominantly young or middle-aged men and typically presented within minutes to hours after donation, similar to the present case (Table 1). Ischemic stroke after plasmapheresis has also been reported [14]. Because symptoms of coronary ischemia may initially be mistaken for benign donation-related complaints or citrate-associated symptoms, persistent chest pain after donation should prompt evaluation for acute coronary syndrome.
|
AUTHORS |
EVENT REPORTED |
AGE AND SEX OF THE PATIENT |
DONATION STATUS |
PREDISPOSING FACTORS |
|
Despotis et al. [7] |
ACS |
62-year-old, male |
34 previous donations |
CAD |
|
Despotis et al. [7] |
ACS |
42-year-old, male |
48 previous donations |
CAD |
|
Leurent et al. [8] |
ACS |
47-year-old male |
21 previous donations |
Apparently not present |
|
Rosencher et al. [9] |
ACS |
57-year-old, male |
54 previous donations |
Apparently not present |
|
Shams and Tipoo [10] |
ACS |
34-year-old, male |
Naïve |
COVID-19 convalescence period |
|
Salahuddin et al. [11] |
Ischemic stroke |
24-year-old, male |
Not reported |
Heterozygous for MTHFR |
|
Salahuddin et al. [11] |
Ischemic stroke |
42-year-old, male |
Multiple, twice weekly for over a year |
Cigarette smoking |
|
Ovali et al. [12] |
Diffuse cerebral thrombosis |
48-year-old, male |
Not reported |
Heterozygous for MTHFR and prothrombin 20210A gene mutations |
An additional consideration in this case is the patient's cannabis use. Cannabis exposure has been associated with adverse cardiovascular outcomes, including acute coronary syndromes, in observational studies [15]. Although the quantity and timing of use could not be reliably established in this case, cannabis use represents a potential cofactor that may have lowered the threshold for thrombosis or coronary vasoreactivity. For that reason, we have interpreted plasma donation as a plausible trigger rather than the sole definitive cause of the event.
Conclusion
With increasing utilization of plasma-derived medicinal products, donors and clinicians should be aware that plasma donation may rarely be followed by life-threatening arterial thrombosis, including STEMI. In patients who develop persistent chest pain after donation, acute coronary syndrome should remain in the differential diagnosis and should prompt urgent evaluation. This case also highlights the importance of considering concomitant prothrombotic or vasoreactive exposures, such as cannabis use, when interpreting rare adverse events after donation.
Take-Home Message
Thrombotic events are extremely rare but potentially lethal complications of plasma donation. Persistent chest pain after donation should be taken seriously and evaluated promptly for acute coronary syndrome.
Abbreviations
AABB: Association for the Advancement of Blood & Biotherapies; ACS: Acute Coronary Syndrome; BMI: Body Mass Index; ECG: Electrocardiogram; EF: Ejection Fraction; HFrEF: Heart Failure with Reduced Ejection Fraction; IVUS: Intravascular Ultrasound; LAD: Left Anterior Descending; Plad: Proximal Left Anterior Descending; PD: Plasma Donation; STEMI: ST-elevation Myocardial Infarction; TIMI: Thrombolysis in Myocardial Infarction
References
2. Amrein K, Valentin A, Lanzer G, Drexler C. Adverse events and safety issues in blood donation--a comprehensive review. Blood Rev. 2012 Jan;26(1):33–42.
3. Benjamin RJ, McLaughlin LS. Plasma components: properties, differences, and uses. Transfusion. 2012 May;52 Suppl 1:9S–19S.
4. Eder AF, Dy BA, Kennedy JM, Notari Iv EP, Strupp A, Wissel ME, et al. The American Red Cross donor hemovigilance program: complications of blood donation reported in 2006. Transfusion. 2008 Sep;48(9):1809–19.
5. Beyan C, Kaptan K, Savaşçi S, Ifran A, Oztürk Y, Okmen B. Platelet apheresis affects prothrombin time and plasminogen levels in healthy donors. Transfus Apher Sci. 2005 Aug;33(1):47–50.
6. Despotis GJ, Goodnough LT, Dynis M, Baorto D, Spitznagel E. Adverse events in platelet apheresis donors: A multivariate analysis in a hospital-based program. Vox Sang. 1999;77(1):24–32.
7. Rajbhandary S, Stubbs JR, Land KJ, Whitaker BI (eds). AABB Donor Hemovigilance Report: 2012-2014 on behalf of the AABB US Donor Hemovigilance Working Group, AABB Press, 2016.
8. Flaum MA, Cuneo RA, Appelbaum FR, Deisseroth AB, Engel WK, Gralnick HR. The hemostatic imbalance of plasma-exchange transfusion. Blood. 1979 Sep;54(3):694–702.
9. Wun T, Paglieroni T, Holland P. Prolonged circulation of activated platelets following plasmapheresis. J Clin Apher. 1994;9(1):10–6.
10. Ovali E, Ratip S, Ozmenoglu M, Karti SS, Uçar F, Ukinç K, et al. Large volume donor plasmapheresis in inherited thrombophilia implicated in arterial thrombosis. Transfus Apher Sci. 2003 Jun;28(3):201–6.
11. Leurent G, Bedossa M, Camus C, Behar N, Mabo P. Can plasma donation induce coronary-artery thrombosis. J Blood Disord Transfus. 2010;1:103.
12. Rosencher J, Zuily S, Varenne O, Spaulding C, Weber S. Acute myocardial infarction secondary to platelet apheresis in a 57-year healthy donor. Int J Cardiol. 2011 Aug 4;150(3):e119–20.
13. Shams P, Tipoo FA. Lateral ST-elevation myocardial infarction after donation of COVID-19 convalescent plasma in a naïve donor. BMJ Case Rep. 2021 Mar 24;14(3):e242542.
14. Salahuddin H, Sheikh AA, Hussaini S, Verghese C, Tietjen GE. Ischemic Stroke After Plasmapheresis. Am J Med Sci. 2018 Oct;356(4):399–403.
15. Jeffers AM, Glantz S, Byers AL, Keyhani S. Association of Cannabis Use With Cardiovascular Outcomes Among US Adults. J Am Heart Assoc. 2024 Mar 5;13(5):e030178.