Abstract
Background and objectives: Previous studies have reported inconsistent findings regarding the association between H. pylori infection and overweight/obesity. This study aims to evaluate the clinical and anthropometric characteristics of children and adolescents with chronic abdominal pain, grouped as follows: (1) non-ulcer dyspepsia with confirmed H. pylori gastritis, and (2) dyspepsia with confirmed chronic esophagitis and without H. pylori infection.
Methods: This single-center, observational, retrospective case-control study used a convenience sample of children and adolescents referred for chronic abdominal pain and non-ulcer dyspepsia. All underwent endoscopy. Diagnosis of Gastritis was based on histopathological findings of inflammation in gastric biopsies from the antrum and gastric body, using the Sydney system classification. Antral-predominant gastritis was defined as moderate to severe antral inflammation and normal to mild corpus inflammation. Pangastritis was defined as inflammation spread throughout the stomach, with little or no difference between the antrum and corpus. The histopathological diagnosis of esophagitis was established using two methods recommended by ESPGHAN.
Results: Among 223 participants, 120 (54%) were classified as having H. pylori gastritis, defined as histologically confirmed gastritis associated with Helicobacter pylori infection, and 103 (46%) were classified as having esophagitis, defined as endoscopically or histologically confirmed inflammation of the esophagus. The groups were well matched. There were no statistically significant differences in baseline characteristics or clinical features, except for nausea (OR=1.79 (1.04–3.03, p=0.03)) and vomiting (OR=1.74 (1.01 – 2.94, p=0.04). Both symptoms were more prevalent in Hp gastritis. There were no significant differences in the proportions of overweight/obesity between the groups: H. pylori gastritis (23.3%) and esophagitis (28.1%). No significant differences were observed between Helicobacter pylori antral and pangastritis for any of the variables analyzed.
Conclusions: Non-ulcer dyspepsia due to H. pylori gastritis or esophagitis is not associated with increased prevalence of overweight or obesity in children from similar environments. Overweight and obesity in this population appear unrelated to H. pylori gastritis.
Keywords
Helicobacter pylori, Esophagitis, Non-ulcer dyspepsia, Overweight, Obesity, Case–control, Children, Adolescents
Abbreviations
BMI: Body Mass Index; CI: Confidence Interval; CRP: C-reactive Protein; ESPGHAN: European Society for Pediatric Gastroenterology; Hepatology and Nutrition; HDI: Human Development Index; IQR: Interquartile Range; MALT: Mucosa-Associated Lymphoid Tissue; NSAIDs: Nonsteroidal Anti-Inflammatory Drugs; WHO: World Health Organization
Introduction
Helicobacter pylori (H. pylori) is a Gram-negative, flagellated, microaerophilic, motile, curved or slightly spiral bacterium that functions as a human gastric pathogen. Its ability to survive in the acidic gastric environment allows it to penetrate the protective mucus layer and persist as a lifelong infection if untreated, since spontaneous elimination during childhood is uncommon [1,2]. H. pylori represents the most prevalent common chronic infection globally, with an estimated 4.4 billion individuals affected [3]. The infection is particularly prevalent in developing countries, where the main risk factors include socioeconomic status, crowded living conditions, and exposure to infected family members [4].
Two meta-analyses examining the global prevalence of H. pylori infection, including pediatric populations, reported seroprevalence rates of 32.6% (95% CI: 28.4–36.8) and 33% (95% CI: 27%–38%) in children, compared to rates exceeding 50% in adults [5,6]. A 2022 meta-analysis further estimated the global prevalence of H. pylori among individuals aged 18 years or younger at 32.3%. The highest infection rates are observed in low- and middle-income countries, particularly in Africa and Latin America, where prevalence in some nations exceeds 70% [4]. Recent data indicate a declining trend in global prevalence among adults, now at 43.7%, whereas prevalence among children remains elevated at 34.4% [7].
H. pylori infection colonizes the gastric mucosa and induces chronic inflammation [8]. It is widely recognized as a causal agent in the development of chronic gastritis, peptic ulcer disease, Mucosa-Associated Lymphoid Tissue (MALT) lymphoma, and gastric adenocarcinoma [8]. Accordingly, the World Health Organization has classified H. pylori as a group I carcinogen [9]. The bacterium's ability to cause persistent inflammation in the gastric mucosa can have significant clinical implications for pediatric populations, potentially impacting growth and increasing the likelihood of chronic gastritis as they develop.
Multiple studies have suggested a potential role for Helicobacter pylori in the pathogenesis of extragastric diseases. H. pylori infection has been linked to iron and vitamin B12 deficiencies, as well as idiopathic thrombocytopenic purpura [10]. It is also strongly associated with chronic active gastritis [11]. In contrast, H. pylori infection appears to be inversely associated with certain upper gastrointestinal diseases, such as gastroesophageal reflux disease. Thus, the causal relationship between H. pylori and these associations remains unestablished, especially in delayed growth [12].
Analogously, overweight and obesity have emerged as major global public health concerns in the twenty-first century, with the prevalence of overweight and obesity having risen substantially. From 1975 to 2016, the number of school-age children and adolescents with obesity increased more than tenfold, with a nearly 50% rise observed between 2000 and 2015 [13,14]. Pediatric obesity is a strong predictor of adult obesity. Approximately 20% of obese infants become obese children, 40% of obese children become obese adolescents, and 80% of obese adolescents become obese adults [15].
Studies examining the association between H. pylori infection and obesity have produced inconsistent results. A central question emerges: does H. pylori have a protective role against obesity, or does it contribute to it, especially in children? Thus, there is ongoing debate over the relationship between obesity and H. pylori infection, while acknowledging that obesity's etiology is far more complex. The association between H. pylori infection and the development of overweight or obesity remains controversial, with inconsistent conclusions across published studies [16,17]. Given that H. pylori gastritis and chronic esophagitis likely share sociodemographic and clinical features with dyspepsia, this study hypothesizes that the presence of chronic H. pylori gastritis may differentially affect anthropometric findings.
Aims
This study aims to evaluate clinical and anthropometric characteristics in children and adolescents, with chronic abdominal pain categorized into two subgroups: (1) non-ulcer dyspepsia associated with H. pylori gastritis and (2) dyspepsia associated with chronic esophagitis.
Methods
Study design, setting, and selection of participants
This single-center study was observational, retrospective, and case-control. It used a convenience sample of consecutive children and adolescents referred to the Brazilian Public Health System between July 2010 and December 2020. Referrals were for the initial evaluation of chronic abdominal pain at a tertiary Outpatient Paediatric Gastroenterology Clinic. All participants lived in the same geographic area: Botucatu, São Paulo State, Southern Brazil. Participants demonstrated adequate educational attainment and general health. Botucatu's Human Development Index (HDI) is 0.800 (HDI Income: 0.790, HDI Longevity: 0.869, HDI Education: 0.746). The study received approval from the local medical and Institutional Review Board (OF 642/2006-CEP).
Inclusion criteria comprised children and adolescents aged 4 to 15 years. Participants had to live with a parent or caregiver showing signs or symptoms consistent with chronic abdominal pain [18], as defined by Apley and Naish [19]. These criteria ensured a homogeneous study population related to the condition. This allowed for a more precise assessment of chronic abdominal pain associated with their living environment. Exclusion criteria included: other chronic digestive diseases (inflammatory bowel disease, celiac disease, cystic fibrosis, intestinal parasitosis, duodenal or gastric ulcers, active gastrointestinal bleeding, history of gastric surgery), genetic, metabolic, immune, cardiac, hepatic, or renal chronic disorders, neurodevelopmental delay, or missing weight or height data.
Data collection
Data were extracted from electronic medical records using a standardized questionnaire for chronic abdominal pain. This questionnaire included demographics, gastrointestinal symptoms, alarm symptoms, and signs. It was based on questions used to take a patient's clinical history [20–22]. The gastroenterology team determined the origin of chronic abdominal pain to be organic based on diagnostic testing. All patients underwent routine laboratory tests, including complete blood count, C-reactive protein (CRP), urinalysis, stool examination for ova and parasites, and H. pylori serology. The gastroenterology team ordered additional diagnostic tests as needed.
Anthropometric measurements and indices
At the initial visit, trained pediatric nurses measured body weight in kilograms using an electronic scale. Height was measured in centimeters with an adjustable stadiometer, following World Health Organization guidelines [23]. BMI (kg/m2) and z-scores were calculated using the WHO AnthroPlus software [24,25], with adjustments for sex and age. Children were then classified as obese (z score >2), overweight (z score 1–2), normal BMI (z score −2 to +1), or underweight (z score <−2) [26].
Endoscopy
Chronic dyspeptic syndrome was described as a set of symptoms believed to originate in the upper gastrointestinal tract. It was defined by recurring or persistent pain or discomfort for at least 2 days per week over at least 3 months. Children and adolescents with chronic dyspeptic syndrome and alarm symptoms or signs suggestive of organic disease underwent esophagogastroduodenoscopy and histopathological examination. Symptoms included epigastric pain, postprandial fullness, retrosternal pain, early satiety, upper abdominal distention, nausea, retching, belching, and vomiting for at least two days per week for at least three months. None of the patients received antisecretory drugs (H2 receptor blockers and proton pump inhibitors), bismuth compounds, NSAIDs, antibiotics, or immunosuppressive drugs in the 4 weeks before endoscopy. At least four biopsy specimens were collected: one from the distal esophagus, two from the gastric antrum, and one from the corpus [27]. One antrum biopsy was used for a rapid urease test (Renylab uretest, Brazil). Collecting biopsy specimens from multiple sites increases diagnostic sensitivity. This is essential for distinguishing H. pylori gastritis from chronic esophagitis.
Histopathology examination
For H. pylori colonization assessment, serial 4-mm longitudinal sections were stained with Hematoxylin-Eosin and Giemsa. Gastritis was diagnosed based on histopathological inflammation in gastric biopsies from the antrum and the gastric body, according to the Sydney system classification [28,29]. An antral-predominant gastritis pattern was defined as moderate to severe inflammation in the antrum and normal to mild inflammation in the corpus. Pangastritis refers to inflammation throughout the stomach, with little or no difference between the antrum and corpus [30]. Esophagitis was diagnosed using two methods, as recommended by ESPGHAN [31,32].
Definition of H. pylori status
Routine diagnosis of H. pylori gastritis and esophagitis was performed using previously described methods [30,33]. Briefly, two experienced pediatric gastroenterologists (the study authors, MAC and NCM) determined the final diagnoses after 3 months of follow-up. Nonulcer dyspepsia with H. pylori was diagnosed if both histopathological evaluation and rapid urease testing were positive on gastric biopsies from the antrum and the gastric body [28]. Patients with only one positive test were excluded from the study. Noninfected status was assigned when both tests were negative. The diagnosis of esophagitis was based on clinical symptoms and signs, endoscopy, and histologic evaluation [34,35]. For more details on data collection, endoscopy, histopathology, and H. pylori status definition, see Carvalho et al. [30] and Correa Silva et al. [33].
Statistical analysis
All data were entered into Excel (Microsoft, Redmond, WA) by one author and checked by another. GraphPad Prism version 8.4.0 for Windows (GraphPad Software, San Diego, California, USA; www.graphpad.com) was used for analysis. Normality of the data distribution was tested with the Shapiro–Wilk test. This test is suitable for small sample sizes and improves the robustness of data interpretation. Fisher's exact test was used to analyze categorical data reported as counts and percentages. It is precise for small sample sizes and low expected counts. Mann–Whitney test was used for continuous variables expressed as median and interquartile range (IQR). This test works well for non-normally distributed data and for unequal variances. For dichotomous data, odds ratios (ORs) and 95% CIs were calculated to estimate effect sizes. This provides a clear understanding of the magnitude and precision of associations. All tests were two-sided. P-values <0.05 were considered statistically significant.
Results
Study population
Figure 1 shows the study eligibility flowchart. During the study, 817 children and adolescents with chronic abdominal pain were assessed. Of these, 279 (34%) were diagnosed with non-ulcer dyspepsia using a standard method. Fifty-six were excluded (33 with H. pylori gastritis, 23 with esophagitis) because of incomplete data or alternative causes. The main reason for excluding the HP subgroup was failing to meet both study inclusion criteria. Of the 223 who met criteria and had endoscopy, 120 (54%) had H. pylori gastritis and 103 (46%) had esophagitis.
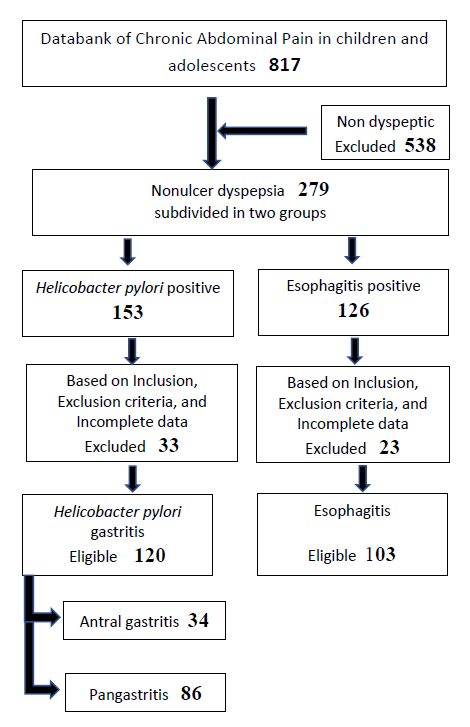
Figure 1. Flow diagram showing the participant's enrollment, eligibility, and final diagnosis.
Baseline characteristics and clinical features
Table 1 compares the baseline characteristics of the Helicobacter pylori gastritis and esophagitis groups. No statistically significant differences were found, confirming that both groups were well matched. Most patients were female: 65.8% in Helicobacter pylori gastritis and 67.9% in esophagitis. Many had family members with gastritis: 51.6% in Helicobacter pylori gastritis and 41.7% in esophagitis.
|
|
*Helicobacter pylori gastritis |
*Esophagitis |
|
Children's characteristics: Median (IQR) Number of children Sex: female n (%) Age of pain onset (mo) Age at first visit, (mo) Duration of symptoms (mo) |
120 79 (65.8) 100 (72–128) 120 (100–152) 12 (5–31) |
103 70 (67.9) 96 (60–120) 117 (93–138) 18 (6–32) |
|
Family's characteristics: Median (IQR) Age of mothers, (y) Age of fathers, (y) Crowding index (person/room) Number of people at home Number of children at home Family gastritis n (%) Family gastric cancer n (%) |
33 (30–37) 37 (32–44) 0.8 (0.6–1.2) 4 (4–5) 2 (2–3) 62 (51.6) 07 (5.8) |
34 (30–39) 38 (33–42) 1.0 (0.6–1.0) 4 (4–5) 2 (1–3) 43 (41.7) 05 (4.8) |
|
*Data analysed with the Mann-Whitney test. All comparisons were statistically nonsignificant. mo: months; y: years. |
||
Table 2 shows the clinical features of both groups. Most features were similar in both. Compared to esophagitis, Helicobacter pylori gastritis showed high frequencies for epigastric pain (85.8% vs. 84.4%), retrosternal pain (50.8% vs. 60.1%), burning (50.8% vs. 47.5%), nocturnal pain (39.1% vs. 28.1%), and decreased appetite (48.3% vs. 39.8%). Few reported weight loss. Only nausea (OR = 1.79, 95% CI: 1.04–3.03, p <0.03) and vomiting (OR = 1.74, 95% CI: 1.01–2.94, p <0.04) differed significantly, both more common in Hp gastritis. These findings support that the two groups had similar clinical and sociodemographic variables.
|
|
Helicobacter pylori gastritis |
Esophagitis |
OR |
95% CI |
p< |
|
Number of children |
120 |
103 |
|
|
|
|
Clinical features n (%) Epigastric pain Retrosternal pain Nausea* Vomiting* Belching Burning type Nocturnal pain Periumbilical pain Early satiety Postprandial fullness Decreased appetite Weight loss |
103 (85.8) 61 (50.8) 71 (59.1) 69(57.5) 10 (8.3) 61 (50.8) 47 (39.1) 10 (8.3) 25 (20.8) 20 (16.6) 58 (48.3) 02 (1.6) |
87 (84.4) 62 (60.1) 46 (44.6) 45 (43.6) 13 (12.6) 49 (47.5) 29 (28.1) 12 (11.6) 12 (11.6) 13 (12.6) 41 (39.8) 05 (4.8) |
1.11 0.68 1.79 1.74 0.62 1.13 1.64 0.68 1.99 1.38 1.41 0.33 |
0.53–2.30 0.40–1.18 1.04–3.03 1.01–2.94 0.26–1.53 0.66–1.89 0.93–2.87 0.28–1.58 0.94–4.17 0.67–2.85 0.81–2.39 0.06–1.60 |
0.85 0.17 0.03 0.04 0.37 0.68 0.09 0.50 0.07 0.45 0.22 0.25 |
|
Sex (Female) |
79 (65.8) |
70 (67.9) |
0.90 |
0.52–1.60 |
0.77 |
|
First-born child |
49 (40.8) |
39 (37.8) |
1.13 |
0.60–1.93 |
0.68 |
|
Data analyzed with Fisher's Exact test. All comparisons were statistically nonsignificant, except for Nausea* and Vomiting*. |
|||||
Nutritional status
Table 3 gives z-scores and percentiles for weight, height, and BMI for age. No significant differences were seen between groups. Overweight or obesity was found in 23.3% of H. pylori gastritis patients and 28.1% of esophagitis patients. Few were undernourished: 1.7% with Helicobacter pylori gastritis and 0.9% with esophagitis. The two groups did not differ on any clinical or anthropometric measures. Table 4 compares anthropometric values between Helicobacter pylori antral and pangastritis. No significant differences were found in any variable. Figure 2 shows no difference in rates of undernutrition, normal nutrition, or overweight/obesity between children and adolescents with H. pylori gastritis and esophagitis.
|
|
Helicobacter pylori Gastritis |
Esophagitis |
|
Number of children |
120 |
103 |
|
Weight* Weight/age z score Weight/age Percentile |
-0.05 (-0.64–0.67) 47.90 (25.9–75.1) |
0.12 (-0.77–1.20) 54.65 (21.83–87.75) |
|
Height* Height/age z score Height/age Percentile |
-0.19 (-0.79–0.57) 43.0 (21.5–71.9) |
0.11 (-0.61–0.90) 54.4 (26.90 –81.60) |
|
BMI* BMI (kg/m2) BMI/age z score BMI/age Percentile |
17.5 (15.5–19.5) 0.15 (-0.61–0.96) 56.5 (28.4–83.5) |
17.10 (15.40 –19.30) 0.08 (-0.73–1.22) 52.30 (23.20–85.33) |
|
*Data analysed with the Mann–Whitney test. All comparisons between Helicobacter pylori gastritis and esophagitis were statistically nonsignificant. |
||
|
|
Helicobacter pylori |
|
|
|
*Antral gastritis |
*Pangastritis |
|
Number of children |
34 |
86 |
|
Weight* Weight/age z score Weight/age Percentile |
0.02 (-0.43–0.83) 50.65 (33.20–79.83) |
-0.12 (-0.74–0.64) 45.30 (22.10–74.10) |
|
Height* Height/age z score Height/age Percentile |
0.02 (-0.56–0.94) 50.95 (28.75–82.60) |
-0.27 (-0.80–0.43) 40.20 (21.30–67.35) |
|
BMI* BMI (kg/m2) BMI/age z score BMI/age Percentile |
17.15 (15.30–20.10) 0.19 (-0.59–0.99) 57.80 (27.33–83.95) |
17.09 (15.58–19.40) 0.11 (-0.63–0.95) 56.00 (28.30–83.30) |
|
*Data analysed with the Mann–Whitney test. All comparisons between Helicobacter pylori antral gastritis and pangastritis were statistically nonsignificant. |
||
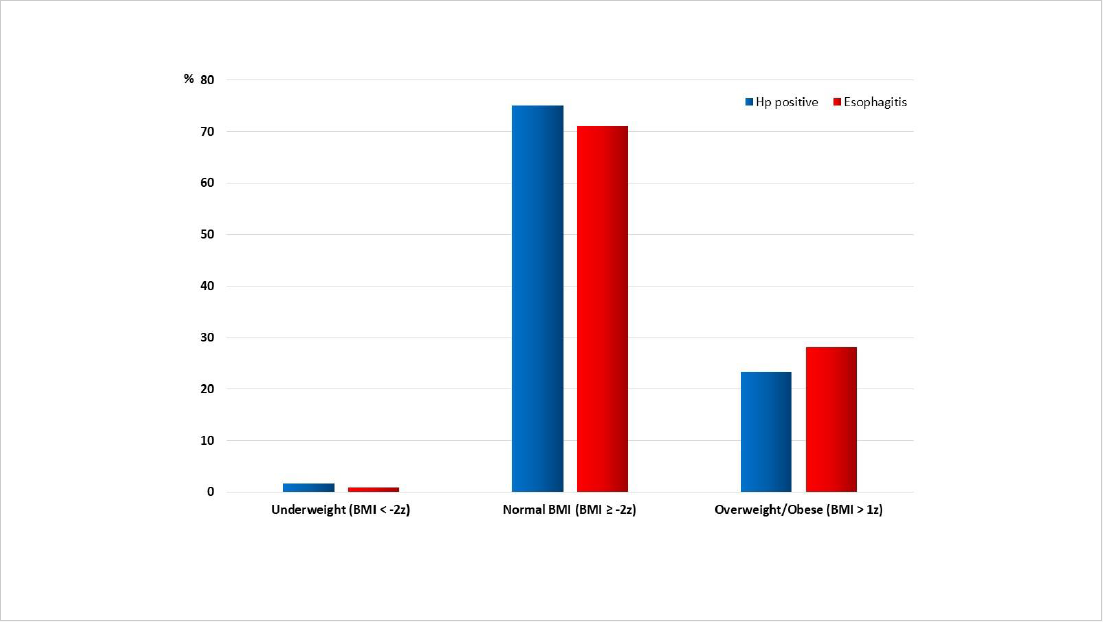
Figure 2. Proportions of undernutrition, normal nutritional status, and overweight/obesity among children and adolescents with H. pylori gastritis and esophagitis.
Discussion
This study specifically compared clinical features and anthropometric indices, such as weight, height, and BMI z-scores and percentiles for age. It aimed to clarify the potential nutritional impact of H. pylori gastritis, using chronic esophagitis as a control. The main findings were: 1) Comparable proportions of overweight and obesity were observed in both groups, with minimal undernutrition and weight loss. 2) No statistically significant differences were found in anthropometric measurements and indices, as assessed by z-scores and percentiles for weight, height, and BMI for age. 3) Baseline characteristics and clinical features did not differ significantly between groups. A high proportion of patients in both groups reported epigastric pain, retrosternal pain, burning sensation, and decreased appetite. 4) Nausea and vomiting were the only clinical features with statistically significant differences, being more prevalent in the H. pylori gastritis group. 5) A substantial proportion of family members had a history of Gastritis in both groups. 6) No significant differences in nutritional status were identified between Helicobacter pylori antral and pangastritis. 7) Throughout the study period, similar proportions of children and adolescents were diagnosed with H. pylori gastritis (with a higher proportion of pangastritis) and esophagitis.
Several methodological aspects warrant emphasis. The methodology was designed to directly support the study's objective of evaluating the association between H. pylori gastritis and esophagitis in patients with non-ulcer dyspepsia. Enhanced diagnostic accuracy reinforced the link between the study methods and the validity of the findings. Two abstractors (MAC, NCM) were trained and standardized in data collection to ensure data quality. One author performed data entry continuously, and another independently verified these entries. Both data abstractors and outcome assessors were blinded to participants' case or control status to minimize potential bias. The blinding process and randomization of data entry contributed to the integrity and objectivity of data handling. All variables were well-matched across groups, further supporting the validity of the study comparisons. Although a lack of significant differences may seem inconclusive, it instead indicates equivalence in baseline characteristics and anthropometric indices. This outcome reinforces the validity of the study's comparisons.
Helicobacter pylori infection is most commonly acquired during early childhood, particularly within the first decade of life, in both high and low-prevalence countries. The infection typically persists throughout life unless appropriately treated with an eradication protocol [36]. The prevalence of H. pylori infection in pediatric populations is high and varies internationally. Major risk factors include low socioeconomic status, inadequate sanitation (such as untreated water, consumption of food in unsanitary conditions, and poor hygiene practices), crowded living environments (including larger family size and more siblings), lower parental educational attainment, and the presence of infected family members [1,3,4].
In this study, the median age of symptom onset and age at first consultation were both below 10 years in each group. Families were generally small, with a crowding index of 0.8–1.0. A substantial proportion of participants reported a family history of Gastritis (51–41%). However, this was based on informant reports rather than clinical or laboratory confirmation. No significant differences in sociodemographic characteristics were identified between the H. pylori gastritis and esophagitis groups. These circumstances characterize the study population as consisting of small families, living in crowded conditions, with a high epidemiological background for gastritis. The region also has a favorable Human Development Index for healthcare, as explained in the Methodology section.
H. pylori can cause persistent inflammation in the gastric mucosa, which has clinical implications. Children and adolescents with non-ulcer dyspepsia linked to H. pylori infection may experience compromised nutritional status. The clinical features of this condition can influence treatment strategies. The precise impact of H. pylori-associated non-ulcer dyspepsia on pediatric patients remains uncertain. Studies exploring H. pylori's role in non-ulcer dyspepsia among children have been inconclusive. The literature often addresses two topics: 1) the link between chronic abdominal pain and H. pylori infection, and 2) the clinical presentation of H. pylori as non-ulcer dyspepsia. Epidemiological studies in pediatric populations report no difference in the prevalence of recurrent abdominal symptoms between children with and without H. pylori [37–39].
During the 1990s and 2000s, several studies reported an association between H. pylori infection and impaired growth. This finding attracted considerable scholarly attention. The infection may impair growth, as it is often acquired during infancy or early childhood, persists throughout life, and causes chronic inflammatory gastritis. These systemic effects could influence growth and potentially reduce final adult height. However, other studies did not support this relationship. Notably, neither the European Study Group for Pediatric Gastroenterology, Hepatology and Nutrition (ESPGHAN) Consensus Conference Report [40] nor the Canadian Helicobacter Study Group Consensus Conference Report [41] endorsed a link between H. pylori infection and impaired growth. The debate continues.
Currently, the relationship between H. pylori infection and overweight, obesity, or BMI remains controversial. Some systematic reviews or meta-analyses have not combined data from both developed and developing countries. This makes it hard to assess the role of H. pylori in overweight or obesity in the general population. In children, some studies suggest that H. pylori infection affects growth, whereas others attribute growth disorders to factors such as socioeconomic status [42–46].
A meta-analysis of 15 studies found no association between H. pylori infection and short stature when prevalence exceeded 50%, suggesting that poor socioeconomic conditions may confound this relationship [12]. This points to the complexity of interpreting H. pylori's impact on growth, especially in comparable populations.
In 2022, a meta-analysis was conducted using a detailed, rigorous search strategy. Strict inclusion criteria were meticulously developed and applied. The meta-analysis summarized evidence on the association between H. pylori infection and growth in children. Twenty-nine studies were included, comprising 16 cross-sectional, seven case-control, and 6 cohort studies. These provided data from 9384 subjects. After quality assessment, 10 studies (all cross-sectional) were of medium quality, while the remaining 19 were of high quality. The results support the hypothesis that H. pylori infection is associated with growth issues in children, thereby increasing the risk of growth disorders [47].
This study has several limitations. First, the retrospective design and recruitment of children from an outpatient pediatric gastroenterology clinic, as well as the relatively small sample size, may limit the generalizability of the findings beyond the population in Southern Brazil (as described in the Methods section). Second, the use of a convenience sample in this retrospective case-control study may introduce selection bias, despite a standardized approach. Third, data on key obesity factors—such as lifestyle, socioeconomic status, and heritability—were unavailable and may have affected the results. Fourth, dietary quality was not assessed. Fifth, BMI does not comprehensively assess body composition, as it cannot distinguish between fat-free mass and adipose tissue.
The study also has strengths. First, diagnoses were systematically evaluated using clinical features, alarm symptoms, routine laboratory tests, endoscopy, and histopathology. Inclusion and exclusion criteria were set to minimize confounding variables and to focus the analysis on chronic abdominal pain with non-ulcer dyspepsia. Second, a standardized methodology was adopted to evaluate children with chronic abdominal pain and yielded a homogeneous convenience sample. Third, all variable characteristics were well matched across groups, supporting the validity of the study comparisons. Fourth, to the best of our knowledge, this is the first study to assess the nutritional status of H. pylori gastritis in Brazilian children and adolescents.
Conclusions
In this study, the proportions of overweight and obesity in H. pylori and esophagitis groups (23.3% and 28.1%, respectively) were similar to the prevalence of overweight and obesity (about 20%) reported in Southeast Brazil for comparable age groups [48,49]. The findings indicate no clinical outcome differences between H. pylori gastritis and esophagitis that would affect growth. The presence of H. pylori in patients with non-ulcer dyspepsia did not independently increase or decrease the prevalence of overweight or obesity among children with similar environments and with esophagitis. These results suggest that the factors influencing overweight and obesity in this population are not directly linked to H. pylori gastritis. Future research should assess food consumption, eating behavior, and adiposity in children and adolescents with H. pylori-associated non-ulcer dyspepsia.
Declarations
Acknowledgments
The authors would like to express their appreciation to the incredible children and families who have profoundly enriched our understanding of the art of Medicine.
Funding
This research received no specific grant from the public, commercial, or not-for-profit funding agencies.
Conflict of interest
The authors declare no conflict of interest.
Author contributions
Study design (NCM, MAC), acquisition of data (JTD, GNH, CDFJ), analysis and interpretation of data (NCM, JTD, MAC), drafting of the manuscript (NCM, MAC), critical revision of the manuscript (NCM). All authors have contributed significantly to this study.
Consent for publication
All authors approved the final manuscript and consented to publication.
Ethical statement
The Ethics Committee approved this retrospective case-control study of Botucatu Medical School (Institutional Review Board (OF 642/2006-CEP). The study was conducted and reported following the guidance from the Committee on Publication Ethics (COPE) and practices according to the Recommendations for the Conduct, Reporting, Editing, and Publication of Scholarly work in Medical Journals from the International Committee of Medical Journal Editors (ICMJE). The individual consent for this retrospective analysis was waived.
Data sharing statement
No additional data are available.
References
2. Suerbaum S, Michetti P. Helicobacter pylori infection. N Engl J Med. 2002 Oct 10;347(15):1175–86.
3. Hooi JKY, Lai WY, Ng WK, Suen MMY, Underwood FE, Tanyingoh D, et al. Global Prevalence of Helicobacter pylori Infection: Systematic Review and Meta-Analysis. Gastroenterology. 2017 Aug;153(2):420–9.
4. Yuan C, Adeloye D, Luk TT, Huang L, He Y, Xu Y, et al. The global prevalence of and factors associated with Helicobacter pylori infection in children: a systematic review and meta-analysis. Lancet Child Adolesc Health. 2022 Mar;6(3):185–94.
5. Zabala Torrres B, Lucero Y, Lagomarcino AJ, Orellana-Manzano A, George S, et al. Review: Prevalence and dynamics of Helicobacter pylori infection during childhood. Helicobacter. 2017 Oct;22(5).
6. Zamani M, Ebrahimtabar F, Zamani V, Miller WH, Alizadeh-Navaei R, Shokri-Shirvani J, et al. Systematic review with meta-analysis: the worldwide prevalence of Helicobacter pylori infection. Aliment Pharmacol Ther. 2018 Apr;47(7):868–76.
7. Chen YC, Malfertheiner P, Yu HT, Kuo CL, Chang YY, Meng FT, et al. Global Prevalence of Helicobacter pylori Infection and Incidence of Gastric Cancer Between 1980 and 2022. Gastroenterology. 2024 Apr;166(4):605–19.
8. Rugge M, Genta RM, Malfertheiner P, Dinis-Ribeiro M, El-Serag H, Graham DY, et al. RE.GA.IN.: the Real-world Gastritis Initiative-updating the updates. Gut. 2024 Feb 23;73(3):407–41.
9. Schistosomes, liver flukes and Helicobacter pylori. IARC Monogr Eval Carcinog Risks Hum. 1994;61:1–241.
10. Franceschi F, Covino M, Roubaud Baudron C. Review: Helicobacter pylori and extragastric diseases. Helicobacter. 2019 Sep;24 Suppl 1:e12636.
11. Rugge M, Genta RM. Staging and grading of chronic gastritis. Hum Pathol. 2005 Mar;36(3):228–33.
12. Wei S, Dang Y, Peng L, Li X, Tang L, Zhang G. Association between Helicobacter pylori infection and delayed growth in children: A meta-analysis. Exp Ther Med. 2020 Jun;19(6):3814–28.
13. Ng M, Fleming T, Robinson M, Thomson B, Graetz N, Margono C, et al. Global, regional, and national prevalence of overweight and obesity in children and adults during 1980–2013: a systematic analysis for the Global Burden of Disease Study 2013. Lancet. 2014 Aug 30;384(9945):766–81.
14. NCD Risk Factor Collaboration (NCD-RisC). Worldwide trends in body-mass index, underweight, overweight, and obesity from 1975 to 2016: a pooled analysis of 2416 population-based measurement studies in 128·9 million children, adolescents, and adults. Lancet. 2017 Dec 16;390(10113):2627–64.
15. GBD 2015 Obesity Collaborators, Afshin A, Forouzanfar MH, Reitsma MB, Sur P, Estep K, et al. Health Effects of Overweight and Obesity in 195 Countries over 25 Years. N Engl J Med. 2017 Jul 6;377(1):13–27.
16. Vo HD, Goli S, Gill R, Anderson V, Stefanov DG, Xu J, et al. Inverse correlation between Helicobacter pylori colonization and obesity in a cohort of inner city children. Helicobacter. 2015 Feb;20(1):64–8.
17. Moran-Lev H, Lubetzky R, Mandel D, Yerushalmy-Feler A, Cohen S. Inverse Correlation between Helicobacter pylori Colonization and Pediatric Overweight: A Preliminary Study. Child Obes. 2017 Aug;13(4):267–71.
18. Di Lorenzo C, Colletti RB, Lehmann HP, Boyle JT, Gerson WT, Hyams JS, et al. Chronic abdominal pain in children: a clinical report of the American Academy of Pediatrics and the North American Society for Pediatric Gastroenterology, Hepatology and Nutrition. J Pediatr Gastroenterol Nutr. 2005 Mar;40(3):245–8.
19. APLEY J, NAISH N. Recurrent abdominal pains: a field survey of 1,000 school children. Arch Dis Child. 1958 Apr;33(168):165–70.
20. Rasquin A, Di Lorenzo C, Forbes D, Guiraldes E, Hyams JS, Staiano A, Walker LS. Childhood functional gastrointestinal disorders: child/adolescent. Gastroenterology. 2006 Apr;130(5):1527–37.
21. Di Lorenzo C, Colletti RB, Lehmann HP, Boyle JT, Gerson WT, Hyams JS, et al. Chronic Abdominal Pain In Children: a Technical Report of the American Academy of Pediatrics and the North American Society for Pediatric Gastroenterology, Hepatology and Nutrition. J Pediatr Gastroenterol Nutr. 2005 Mar;40(3):249–61.
22. Chelimsky G, Czinn SJ. Techniques for the evaluation of dyspepsia in children. J Clin Gastroenterol. 2001 Jul;33(1):11–3.
23. Physical status: the use and interpretation of anthropometry. Report of a WHO Expert Committee. World Health Organ Tech Rep Ser. 1995;854:1–452.
24. de Onis M, Onyango AW, Borghi E, Siyam A, Nishida C, Siekmann J. Development of a WHO growth reference for school-aged children and adolescents. Bull World Health Organ. 2007 Sep;85(9):660–7.
25. World Health Organization. WHO AnthroPlus for personal computers Manual: Software for assessing growth of the world's children and adolescents. 2009. Available from: https://www.who.int/toolkits/growth-reference-data-for-5to19-years/application-tools
26. de Onis M, Lobstein T. Defining obesity risk status in the general childhood population: which cut-offs should we use? Int J Pediatr Obes. 2010 Dec;5(6):458–60.
27. Elitsur Y, Lawrence Z, Triest WE. Distribution of Helicobacter pylori organisms in the stomachs of children with H. pylori infection. Hum Pathol. 2002 Nov;33(11):1133–5.
28. Dixon MF, Genta RM, Yardley JH, Correa P. Classification and grading of gastritis. The updated Sydney System. International Workshop on the Histopathology of Gastritis, Houston 1994. Am J Surg Pathol. 1996 Oct;20(10):1161–81.
29. Rugge M, Genta RM. Staging and grading of chronic gastritis. Hum Pathol. 2005 Mar;36(3):228–33.
30. Carvalho MA, Machado NC, Ortolan EV, Rodrigues MA. Upper gastrointestinal histopathological findings in children and adolescents with nonulcer dyspepsia with Helicobacter pylori infection. J Pediatr Gastroenterol Nutr. 2012 Nov;55(5):523–9.
31. Knuff TE, Benjamin SB, Worsham GF, Hancock JE, Castell DO. Histologic evaluation of chronic gastroesophageal reflux. An evaluation of biopsy methods and diagnostic criteria. Dig Dis Sci. 1984 Mar;29(3):194–201.
32. Leape LL, Bhan I, Ramenofsky ML. Esophageal biopsy in the diagnosis of reflux esophagitis. J Pediatr Surg. 1981 Jun;16(3):379–84.
33. Correa Silva RG, Machado NC, Carvalho MA, Rodrigues MA. Helicobacter pylori infection is high in paediatric nonulcer dyspepsia but not associated with specific gastrointestinal symptoms. Acta Paediatr. 2016 May;105(5):e228–31.
34. Vandenplas Y. Reflux esophagitis in infants and children: a report from the Working Group on Gastro-Oesophageal Reflux Disease of the European Society of Paediatric Gastroenterology and Nutrition. J Pediatr Gastroenterol Nutr. 1994 May;18(4):413–22.
35. Lundell LR, Dent J, Bennett JR, Blum AL, Armstrong D, Galmiche JP, et al. Endoscopic assessment of oesophagitis: clinical and functional correlates and further validation of the Los Angeles classification. Gut. 1999 Aug;45(2):172–80.
36. Kienesberger S, Perez-Perez GI, Olivares AZ, Bardhan P, Sarker SA, Hasan KZ, et al. When is Helicobacter pylori acquired in populations in developing countries? A birth-cohort study in Bangladeshi children. Gut Microbes. 2018;9(3):252–63.
37. Shu X, Ping M, Yin G, Jiang M. Investigation of Helicobacter pylori infection among symptomatic children in Hangzhou from 2007 to 2014: a retrospective study with 12,796 cases. PeerJ. 2017 Jan 31;5:e2937.
38. Chobot A, Porębska J, Krzywicka A, Żabka A, Bąk-Drabik K, Pieniążek W, et al. No association between Helicobacter pylori infection and gastrointestinal complaints in a large cohort of symptomatic children. Acta Paediatr. 2019 Aug;108(8):1535–40.
39. Alimohammadi H, Fouladi N, Salehzadeh F, Alipour SA, Javadi MS. Childhood recurrent abdominal pain and Helicobacter pylori infection, Islamic Republic of Iran. East Mediterr Health J. 2017 Feb 1;22(12):860–4.
40. Drumm B, Koletzko S, Oderda G. Helicobacter pylori infection in children: a consensus statement. European Paediatric Task Force on Helicobacter pylori. J Pediatr Gastroenterol Nutr. 2000 Feb;30(2):207–13.
41. Bourke B, Ceponis P, Chiba N, Czinn S, Ferraro R, Fischbach L, et al. Canadian Helicobacter Study Group Consensus Conference: Update on the approach to Helicobacter pylori infection in children and adolescents--an evidence-based evaluation. Can J Gastroenterol. 2005 Jul;19(7):399–408.
42. Crowe SE. Helicobacter pylori Infection. N Engl J Med. 2019 Mar 21;380(12):1158–65.
43. Pundak OY, Topf Olivestone C, Hofi L, Kori M. Lack of association between Helicobacter pylori infection and childhood overweight/obesity. Helicobacter. 2020 Oct;25(5):e12728.
44. Bray GA, Frühbeck G, Ryan DH, Wilding JP. Management of obesity. Lancet. 2016 May 7;387(10031):1947–56.
45. Lender N, Talley NJ, Enck P, Haag S, Zipfel S, Morrison M, et al. Review article: Associations between Helicobacter pylori and obesity--an ecological study. Aliment Pharmacol Ther. 2014 Jul;40(1):24–31.
46. Xu C, Yan M, Sun Y, Joo J, Wan X, Yu C, et al. Prevalence of Helicobacter pylori infection and its relation with body mass index in a Chinese population. Helicobacter. 2014 Dec;19(6):437–42.
47. Xu C, Wu Y, Xu S. Association between Helicobacter pylori infection and growth outcomes in children: A meta-analysis. Helicobacter. 2022 Feb;27(1):e12861.
48. Niehues JR, Gonzales AI, Lemos RR, Bezerra PP, Haas P. Prevalence of overweight and obesity in children and adolescents from the age range of 2 to 19 years old in Brazil. Int J Pediatr. 2014;2014:583207.
49. Ferreira CM, Reis NDD, Castro AO, Höfelmann DA, Kodaira K, Silva MT, et al. Prevalence of childhood obesity in Brazil: systematic review and meta-analysis. J Pediatr (Rio J). 2021 Sep-Oct;97(5):490–9.