Abstract
Background: Salmonella-IL2 is an attenuated Salmonella Typhimurium strain carrying the human gene for IL-2. When orally administered in preclinical trials, the bacterium colonizes tumors and locally releases IL-2, triggering immunologically-mediated tumor cell killing without untoward side effects. In addition, extensive preclinical studies and a human phase I trial demonstrated robust NK cell subset population surge with oral administration of Salmonella-IL2.
Objective: A non-randomized, two-arm phase 2 study evaluated the combination of Salmonella-IL2 with standard of care (SOC) chemotherapy was conducted.
Methods: Arm One patients received Salmonella-IL2 plus FOLFIRINOX (FFX). Arm Two patients received Salmonella-IL2 plus Gemcitabine/nab-Paclitaxel (GEM/nabP). Overall survival (OS), progression-free survival (PFS), safety, and biomarker data in each arm were collected and compared to corresponding values for reference patients with stage IV pancreatic cancer (SOC Controls) receiving care at the study site from 2016 to 2020. Four patients with stage IV pancreatic cancer were treated via Salspera’s Expanded Access Program (EAP) using the Arm One regimen.
Results: In total, 34 patients (30 in the trial, 4 via EAP) were enrolled: 26 received Salmonella-IL2 with FOLFIRINOX and eight received Salmonella-IL2 with GEM/NabP. SOC Control patients comprised of 37 administered FOLFIRINOX and 31 given GEM/nabP. Those patients who received more than five doses of Salmonella-IL2 with FOLFIRINOX (n=20) had a mPFS (median Progression Free Survival) of 15 months vs. 5.8 months (p<0.001) in control patients who had received only FOLFIRNOX. For those same compared cohorts, the mOS (median Overall Survival) was 20.3 months vs. 11.5 months (p<0.1). Only eight patients were enrolled in the GEM/NabP Arm thus limiting useful conclusions. Overall, 41 serious adverse events (SAEs) were noted and attributed to SOC chemotherapy agents but none to Salmonella-IL2. Overall Response Rate (ORR) was 70%.
Conclusions: Addition of Salmonella-IL2 to FOLFIRINOX demonstrates a remarkable safety profile in that no serious adverse events were attributed to this study drug. In addition, the compelling preliminary efficacy with an overall response rate of 70% and with a statistically significant increased mPFS and mOS supports a global, 2-Arm, multicenter and randomized phase III trial for stage 4 metastatic pancreatic cancer. ClinicalTrials.gov identifier: NCT04589234.
Keywords
Bacterial based immunotherapy, Cancer immunology, Immunotherapy, Tumor immunology
Introduction
Pancreatic ductal adenocarcinoma (PDAC) is among the most lethal malignancies worldwide, with over 500,000 new cases diagnosed annually. Due to the absence of effective early detection strategies, 40–50% of patients present with metastatic (stage IV) disease, representing over 200,000 newly diagnosed metastatic cases globally each year. Furthermore, with the incidence rising every year, it is estimated that by the year 2050 there will be nearly 1 million cases worldwide [1]. For those patients with Stage 4 distant metastatic disease, the current standard of care (SOC) is either a four drug regimen (FOLFIRINOX or NALIRIFOX) or the two-drug regimen of Gemcitabine with nab-paclitaxel (GEM/nabP) [2,3]. A recent meta-analysis of these first line chemotherapeutic strategies evaluated seven trials using data for 2,581 patients that accumulated during more than a decade of clinical trials [4]. This analysis revealed that median progression free (PFS) and overall survival (OS) for the FOLFIRINOX and NALIRIFOX regimens were 7.3 or 7.4 months, and 11.7 or 11.1 months, respectively. For patients treated with Gemcitabine/nab Paclitaxel (GEM/nabP), median PFS was 5.7 months and median OS was 10.4 months. To date, numerous clinical trials evaluating targeted agents, immunotherapies, and combination regimens in metastatic pancreatic ductal adenocarcinoma (PDAC) have yielded limited survival benefit beyond standard chemotherapy, although multiple investigational therapies remain under active evaluation. These disappointing results highlight the urgent need for therapeutic approaches that overcome the profound immune resistance and stromal barriers characteristic of PDAC [5].
In recent years, microbial-based cancer therapeutics have become attractive adjuncts for cancer therapy because of their intrinsic immune-enhancing and cancer-targeting properties [6,7]. Salspera has developed an attenuated strain of Salmonella Typhimurium that is non-toxic, orally administered, and specifically engineered to carry the human gene for IL-2 (renamed Salmonella-IL2 or Saltikva) [8]. Salmonella-IL2 triggers immunologically mediated tumor cell killing within tumor microenvironment [9–11]. Significant anti-tumor effects of this bacterial strain have been demonstrated to date in preclinical models of metastatic colorectal cancer, pancreatic cancer, neuroblastoma, and osteosarcoma [8–15]. Moreover, a large mammal trial that we conducted in companion dogs with pulmonary metastases from osteosarcoma demonstrated a 22% complete response rate and significant disease-free survival in dogs who received Salmonella-IL2 plus standard of care Doxorubicin, when compared to the response in dogs given Doxorubicin alone [16]. In addition, a phase I, single-dose, dose escalation trial in humans demonstrated significant elevation of NK and NK-T cell populations after patients with metastatic GI cancers received Salmonella-IL2 [17].
To determine whether adjunctive oral administration of Salmonella-IL2 is beneficial in patients receiving standard of care chemotherapy for stage IV pancreatic adenocarcinoma, a first of its kind phase II non-randomized clinical trial was performed where an orally administered, Live Biotherapeutic Platform attenuated bacteria was used with intent to treat. The primary outcome variables in this phase II study were overall survival and progression free survival. Secondary outcome data were obtained using biomarker analyses, radiologic studies and safety profile detection.
Methods
Trial design and monitoring
A Health Canada and local IRB approved, non-randomized, two-arm study in patients with Stage IV adenocarcinoma of the pancreas was conducted at the Segal Cancer Centre of the Jewish General Hospital (JGH), McGill University in Montreal. The goal was to recruit up to 30 patients per arm; Arm One: Salmonella-IL2 with FOLFIRINOX and Arm Two: Salmonella-IL2 with Gemcitabine/nab Paclitaxel. Salmonella-IL2 is orally administered concomitantly with the administration of the prescribed chemotherapy according to arm of enrollment. Specifically, 109 colony forming units of attenuated Salmonella-IL2 were administered orally after ingestion of a gastric acid neutralizing agent and followed with 200 ml of an isotonic crystalloid fluid. Dose escalation of the study drug was not permitted. Arm One: patients with stage IV pancreatic cancer were administered the FOLFIRINOX regimen given as first line chemotherapy in the first line. FOLFIRINOX was administered every two weeks and Salmonella-IL2 was administered three days after each cycle of FOLFIRINOX. Arm Two: patients with stage IV pancreatic cancer were administered Gemcitabine/nab Paclitaxel regimen given as first line chemotherapy in the first line. Gemcitabine/nab Paclitaxel was administered every four weeks on days one, eight, and fifteen; while Salmonella-IL2 was administered every two weeks. Dosing modification and “chemo holidays” were permitted at the discretion of treating oncologists. Routine blood work (complete blood counts, serum electrolytes, and hepatic function testing), CT scans, and biomarker analysis were performed at the minimum of every 3 months. Patients were followed biweekly to monitor for progress while on treatment and assessment of toxicity.
Primary outcome variables were overall survival and progression-free survival (as determined by CT imaging read by radiologist blinded to study arm enrollment using a standardized approach to reading CT scans to determine oncologic solid tumor progression (RECIST 1.1 criteria) [18]. Biomarker data, adverse events (AEs) and Serious Adverse Events (SAEs) were tabulated secondary outcomes [19]. Outcomes were compared to those of patients with stage IV pancreatic cancer who received FOLFIRINOX alone (SOC-FFX controls) in the first line (n=37) or Gemcitabine/nab Paclitaxel alone (SOC-Gem/nabP controls) in the first line (n=31) during four years (2016–2020) at the study site prior to initiating the present trial. This study was conducted in accordance with the principles of the Declaration of Helsinki and the International Council for Harmonization guidelines for Good Clinical Practice [20]. Trial oversight was provided by the sponsor (Salspera Inc), the principal investigators (Gerald Batist, MD and Petr Kavan, MD) and their team at the JGH, an independent clinical trial monitor (Exactis, Montreal, QC, Canada), and an independent Data Safety and Monitoring Committee (DSMC). All patients provided written informed consent.
Patients
Eligible adults (>18 years of age) had histologically confirmed diagnosis of stage IV pancreatic adenocarcinoma with radiographically confirmed distant metastatic disease measurable by Response Evaluation Criteria in Solid Tumors, version 1.1 (RECIST 1.1) criteria [18]. All patients had an Eastern Cooperative Oncology Group (ECOG) performance status of ≤1. An Eastern Cooperative Oncology Group (ECOG) performance status of ≤1 indicates that enrolled patients had limited functional limitations, reflecting a population more likely to tolerate intensive therapy. Patients who were receiving other investigational agents or who had brain metastases were not enrolled in this trial. Full inclusion and exclusion criteria are provided in the protocol (available upon request). Current standard of care practice for patients with stage IV pancreatic cancer is to offer one of two chemotherapeutic regimens (FOLFIRINOX or Gemcitabine/nab Paclitaxel) [2,3]. Assignment to treatment arms was based on the clinician’s judgement of a patient’s likely tolerance to treatment. Modifications to the chemotherapeutic regimens such as “chemo holidays” and dose reductions were at the discretion of the treating oncologist however, Salitkva was administered every 2 weeks. Given the persistently poor outcomes associated with metastatic pancreatic ductal adenocarcinoma and following presentation of the interim clinical findings at AACR and ASCO, Salspera received substantial global interest and numerous requests for access to Saltikva. In response, an Expanded Access Program (EAP) was established to provide treatment opportunities for eligible patients with limited therapeutic options. Each request was rigorously reviewed by Salspera’s Medical Advisory Board, and patients who satisfied the same inclusion and exclusion criteria as the prospective clinical trial were enrolled through the EAP and included in the overall trial analysis. Thus, in addition to recruited study patients, Salspera also provided the study drug to four patients with stage IV pancreatic cancer via an Expanded Access Program (EAP). These patients were treated per the FOLFIRINOX Arm of the study protocol, met formal inclusion criteria for the trial, and were included in the study analysis. Per protocol, their CT scans were read using RECIST 1.1 criteria and all other aspects of the clinical trial protocol were followed for these EAP patients.
Historical controls
The precedent to use historical controls in the study of therapies for rarer and deadlier cancers is well established [21–23]. In designing this clinical trial, we sought to compare outcomes not only with published benchmarks from multiple studies evaluating standard-of-care regimens for stage IV pancreatic adenocarcinoma, including FOLFIRINOX and gemcitabine/nab-paclitaxel, but also with a study site–specific historical control cohort that allowed for direct institutional comparison. This historical control group included all patients treated at the study site with stage IV pancreatic adenocarcinoma who received the same standard-of-care chemotherapy regimens (FOLFIRINOX or gemcitabine/nab-paclitaxel) during the four years preceding trial initiation (2016–2020). These patients were treated by the same oncologist, nursing staff, and pharmacy staff. Importantly, radiographic response assessments for these historical control patients were evaluated using RECIST 1.1 criteria by radiologists who were blinded to patient outcomes, providing a consistent and objective comparator for the clinical trial population.
Study drug: Salmonella-IL2
Salmonella-IL2 is an attenuated strain of S. enterica Typhimurium that is rendered avirulent by deletion of cya and crp genes required for cyclic-AMP maintenance of virulence [24,25]. In addition, this strain lacks the enzyme aspartate semialdehyde dehydrogenase (asd). Bacteria that lack this enzyme cannot synthesize diaminopimelic acid (DAP), an essential component of the bacterial cell wall, and thus cannot survive unless they carry a plasmid with the asd gene. We have constructed a plasmid (pIL2) by incorporating the cDNA sequence for C- terminally truncated human IL-2 into plasmid pYA292, which also contains the asd gene and is therefore capable of rescuing this attenuated strain of S. enterica. Thus, if this organism were to lose the plasmid, it would not be able to construct its bacterial cell wall and quickly die. These circumstances result in stable plasmid maintenance without the need for antibiotic selection. In sum, our study agent is attenuated S. enterica with the pIL2 plasmid also known as Salmonella-IL2 (Saltikva).
Preclinical experimentation demonstrated that this engineered strain of Salmonella invades and colonizes tumor microenvironments [6,11–15]. Orally administered Salmonella-IL2 carrying the IL-2 gene has been proven to produce biologically active IL-2 that is locally released in tumor microenvironments [8]. The natural activity of IL-2 is to increase populations of NK and CD8+ cytotoxic T cells in tumor microenvironments as well as in the peripheral blood [26]. Both of these cell types have the unique property of indiscriminately killing cancer cells. We have also demonstrated in pre-clinical studies that Salmonella-IL2 significantly stimulates both a NK cell and CD8+T cell population surge both within the tumor microenvironment and in the peripheral blood in preclinical studies. Both of these cell types observed experimentally are thought to impart a direct cancer cell kill and aid in the development of long-term anti-tumor memory. Salmonella infection alone (without the IL-2 gene) also appears to produce a bystander, immunologically mediated surge in various immune cell types, such as CD4+ T cells within the tumor microenvironment, further contributing to an anti-cancer effect but to a lesser effect than when the IL-2 gene is added to the attenuated Salmonella. During investigations in nearly 4,000 mice administered Salmonella-IL2 using tumor models of metastatic colorectal cancer, primary breast cancer, primary neuroblastoma, metastatic osteosarcoma, or primary pancreatic cancer, no untoward effects of the drug were observed in treated mice [6,8–15].
A phase I, dose escalation, single-dose trial was also conducted in 22 patients with metastatic GI cancers receiving care at the University of Minnesota [17]. That human trial clearly demonstrated lack of toxicity from orally administered adjunctive Salmonella-IL2. Although no survival advantage was observed when a single dose of Salmonella-IL2 was used, a significant increase in both peripheral blood NK and NK-T cell populations in these cancer patients was observed. Thus, confirming the immunologic cell populations surge that has also been observed in clinical studies.
Trial administration
Data were collected by investigators and a third-party clinical trial monitor (Exactis, Montreal, Quebec, Canada). Data were compiled by the clinical trial monitor and analyzed by the sponsor. An independent Data Safety and Monitoring Committee (DSMC) reviewed the clinical protocol and periodically reviewed the clinical trial data and gave permission to continue the trial to completion. All authors contributed to the interpretation of data and preparation of the manuscript. They vouch for the completeness of the data collected and the statistical analysis.
Endpoints
The primary endpoint was length of survival from the time of diagnosis and an objective response was defined as either a complete or partial response according to RECIST 1.1 criteria. Secondary endpoints included safety and systemic biomarker (CEA and CA19-9) responses. Patients alive at the time of data cutoff were censored at their last known date of follow-up as of March 1, 2025. Progression-free survival (PFS) was defined as the time from treatment initiation to either radiologically confirmed disease progression per RECIST 1.1 criteria or death, whichever occurred first. These definitions match established oncology standards for survival endpoints and allow proper handling of censored observations. Adverse events were graded and categorized according to the National Cancer Institute Common Terminology Criteria for Adverse Events (v5.0) with attribution to the administered chemotherapy or study drug [19].
Statistical analysis
All statistical analyses were conducted in a pre-specified, observational fashion to compare outcomes of patients who received Salmonella-IL2 adjunctive therapy in combination with standard chemotherapy to outcomes of historical control group patients treated at the same site over the four years (2016–2020) preceding study initiation.
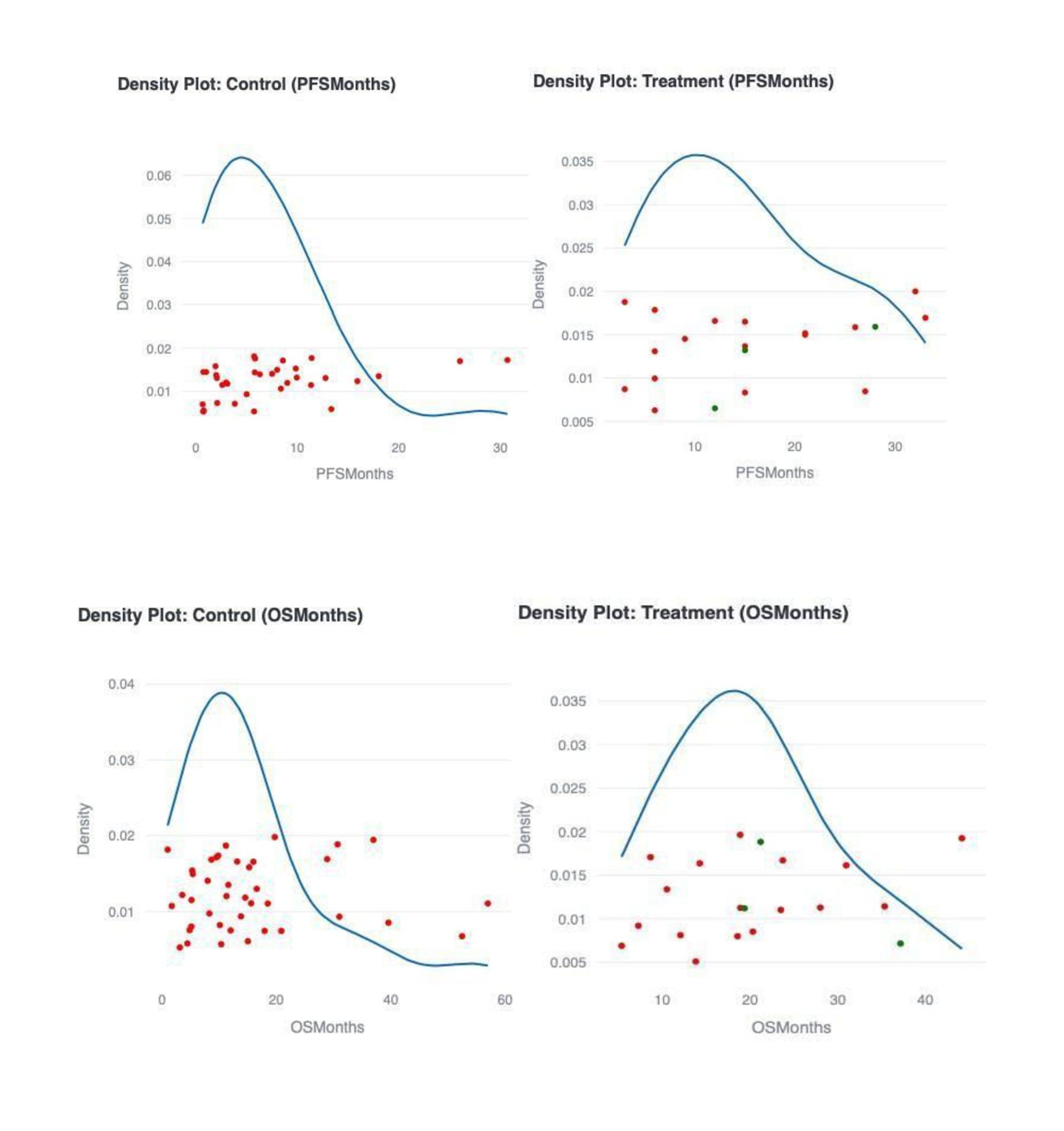
Survival distributions for OS and PFS were estimated using the Kaplan-Meier (KM) method, which provides a non-parametric estimate of the survival function and accommodates right-censored data without assuming an underlying survival distribution. Median survival times were reported with their corresponding 95% confidence intervals (CIs). Differences in survival distributions between treatment and control groups were assessed using two-sided log-rank tests. The log-rank test compares the entire survival curves, not just median values, and does not assume proportional hazards. Statistical significance was defined as p<0.05 for all two-sided tests. Kernel density estimation plots of the survival data were also constructed to visually support the statistically significant differences observed.
To quantify the relative risk of death or progression, hazard ratios (HRs) and their 95% CIs were estimated using Cox proportional hazards regression. The Cox model was fit with the treatment group (Salmonella-IL2 plus SOC versus SOC alone) as a main effect, providing an estimate of the instantaneous relative hazard over time. The HRs from the Cox models are presented to facilitate interpretation of the effect size relative to standard therapy.
Software and reproducibility
All analyses were conducted using Python (version 3.11) and the “lifelines” survival analysis library for Kaplan-Meier estimates, log-rank tests, and Cox regression models. All p-values greater than 0.05 and Confidence Interval (CIs) are presented as exact values without adjustment for multiple comparisons.
Results
Patients
As of the data cutoff date of March 1, 2025, 37 patients were enrolled in the clinical study. Recruitment was halted when improvement in the PFS relative to the control group patients reached p<0.05 in the FOLFIRINOX plus Salmonella-IL2 arm. Twenty-six patients were enrolled in the Salmonella-IL2 plus FOLFIRINOX arm. Three withdrew from the study shortly after enrolling, and one patient was non-compliant with administration of the study drug, so that 22 patients remained for full analyses. With the four Expanded Access Program patients, a total of 26 patients remained in the Salmonella-IL2 plus FOLFIRINOX arm. Of these 26 patients, 20 patients received >5 doses of Salmonella IL-2.
Eleven patients were enrolled in the Salmonella-IL2 plus Gemcitabine/nab Paclitaxel arm; three of them failed their screen entrance to the study. Thus, eight patients remained in the Salmonella-IL2 plus Gemcitabine/nab Paclitaxel arm. Table 1 details patient demographics. Enrolled patients tended to be older in the Gemcitabine/nab Paclitaxel arm but in all other noted characteristics, the participants tended to be similar.
|
|
Arm One (N=26) |
Arm Two (N=11) |
Total (N=37) |
|
Race |
|
|
|
|
N |
26 |
11 |
37 |
|
Black |
1 (4.2%) |
1 (9.1%) |
2 (5.7%) |
|
Chinese |
1 (4.2%) |
0 (0.0%) |
1 (2.9%) |
|
South Asian - East Indian, Pakistani, Sri Lankan… |
1 (4.2%) |
0 (0.0%) |
1 (2.9%) |
|
White or Caucasian |
23 (88.5%) |
10 (90.9%) |
33 (89.2%) |
|
Age at consent |
|
|
|
|
N |
26 |
11 |
37 |
|
Mean ± SD |
58.7 ± 11.2 |
68.0 ± 7.0 |
61.6 ± 10.9 |
|
Mean [CI 95%] |
58.7 [54.0, 63.4] |
68.0 [63.3, 72.7] |
61.6 [57.9, 65.4] |
|
Median (P25, P75) |
61.5 (52.2, 65.5) |
66.0 (63.5, 72.0) |
63.0 (57.5, 69.0) |
|
Min - Max |
32.0 - 74.0 |
56.0 - 82.0 |
32.0 - 82.0 |
|
Sex at birth |
|
|
|
|
N |
26 |
11 |
37 |
|
Female |
13 (50.0%) |
6 (54.5%) |
19 (51.4%) |
|
Male |
13 (50.0%) |
5 (45.5%) |
18 (48.6%) |
Historical control patients
Specifically, patients who received Salmonella-IL2 with FOLFIRINOX were compared to historical control patients who were treated at the study site in the four years prior to starting the study (n=37, average age 58 years; range 33–75 years; 46% born female) who were administered FOLFIRNOX alone in the first line (SOC-FFX controls) . Thirty-six of 37 of these SOC-FFX control patients had a documented ECOG performance status score; 34 had an ECOG score of ≤1, one was score 2, none had a score 3, and one had an ECOG score of 4. Patients who received Samonella-IL2 with Gem/nabP were compared to control patients (n=31, average age 65.1 years; range 45–84 years; 42% born female) who were administered Gem/nabP alone in the first line (SOC-Gem/nabP controls). Twenty-seven of 31 of these SOC-Gem/nabP control patients had a documented ECOG performance status score; 25 had an ECOG score of ≤1, two were score 2, none had a score 3, and none had an ECOG score of 4. Radiologists blinded to patient outcomes at the study site reviewed all of the CT scans that were obtained from both groups of these control patients to determined response using RECIST 1.1 criteria. These data were used to determine PFS. As with patients in the clinical trial, control patient chemotherapeutic management consisting of “chemo holidays”, reducing dosing, or elimination of a particular chemotherapeutic medication was performed at the discretion of the same treating oncologist who administered the clinical trial and who adjusted for drug tolerance and toxicity.
Clinical activity and efficacy
Salmonella-IL2 with FOLFIRINOX
A significant therapeutic effect was observed in those patients who received more than five doses of Salmonella-IL2 plus FOLFIRINOX (n=20). A statistically significant increase in median progression free survival (mPFS) was observed (15 months vs. 5.8 months, 95% CI, HR 0.3, Concordance Index 0.64) when compared to patients who received FOLFIRINOX alone (p<0.001) (Figure 1, Table 2). In addition, significant increase in median overall survival (mOS) of 20.3 months was also observed when compared to mOS of SOC-FFX control patients alone of 11.5 months (p<0.05, 95% CI. HR 0.59, Concordance Index 0.59) (Figure 2, Table 2). Kernel density estimation plots of the survival data visually support the differences observed, illustrating that a higher proportion of patients in the treatment group experienced longer overall and progression-free survival than those in the SOC-FFX control group. The rightward extension of the treatment density curves aligns with the reduced instantaneous risk observed in the Cox proportional hazards models. The hazard ratio was 0.59 for overall survival and for progression-free survival, it was 0.34. This graphical evidence qualitatively reinforces the quantitative message in the data (Figure 3).
When examining all compliant patients enrolled in the Salmonella-IL2 plus FOLFIRINOX arm of the trial, excluding the Expanded Access Program patients but including those who received greater than five doses of Salmonella-IL2 (n=16), the mPFS was 13.5 months compared to 5.8 months in SOC-FFX control patients (p<0.05, 95% CI, HR 0.48, Concordance Index 0.61) while the mOS was 18.6 months in treated patients compared to 11.5 months in SOC-FFX control patients (p=0.5, 95% CI, HR 0.8, Concordance Index 0.56) (Table 2). Analysis of all compliant patients who received FOLFIRINOX plus Salmonella-IL2 including those EAP patients (n=25), the mPFS was 15 months compared to 5.8 months in SOC-FFX control patients (p<0.001, 95% CI, HR 0.39, Concordance Index 0.62) and the mOS was 18.6 months compared to 11.5 in Controls (p=0.3, 95% CI, HR 0.76, Concordance Index 0.54). Lastly, analysis of all compliant patients enrolled into the trial and excluding EAP patients (n=21), the mPFS was 12.0 months compared to 5.8 months in SOC-FFX control patients (p<0.05, 95% CI, HR 0.51, Concordance Index 0.59) and the mOS was 13.8 months compared to 11.5 months in SOC-FFX control patients (p=.83, 95% CI, HR 1.06, Concordance Index 0.49) (Table 2).
|
|
Salmonella-IL2 + FFX mPFS (months) |
Salmonella-IL2 + FFX mOS (months) |
Response Rates (95% CI)** |
% Surviving 1 and 2 years |
|
All patients who received >5 doses, including EAP patients (n=20) |
15 (Range 3–33 months) |
20.3 (Range 5.3–44.1 months) |
PRR: 70% (45.5–87.9%) CRR: 0 (0–13.9%) ORR: 70% |
1 Yr Survival: 65% 2 Yr Survival: 40% |
|
All patients including ≤5 doses, including EAP patients (n=25) |
15 (Range 3-33 months) |
18.6 (Range: 2.1–44.1 months) |
PRR: 56% (34.9–75.6%) CRR: 0 (0–13.7%) ORR: 56% |
1 Yr Survival: 52% 2 Yr Survival: 32% |
|
Compliant patients, no EAP patients, including ≤5 doses (n=21) |
12 (Range 3–32 months) |
13.8 (Range 2.1–35.3 months) |
PRR:47.6% (25.7–70.2%) CRR: 0 (25.7–70.2%) ORR: 47.6% |
1 Yr Survival: 42.9% 2 Yr Survival: 19% |
|
Compliant patients who received >5 doses, No EAP patients (n=16) |
13.5 (Range 3–32 months) |
18.6 (Range 5.3–35.3 months) |
PRR: 62.5% (35.4–84.8%) CRR: 0 (0–16.9%) ORR: 62.5% |
1 Yr Survival: 56.2% 2 Yr Survival: 25% |
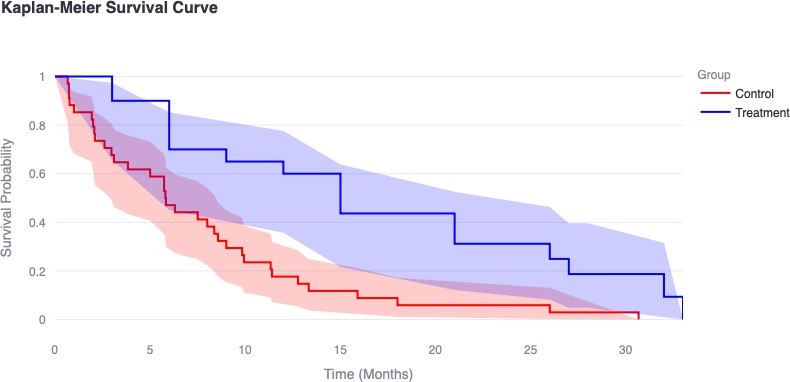
Figure 1. Median Progression Free Survival (mPFS) of study compliant and Expanded Access Program patients who received greater than five doses of Salmonella-IL2 with FOLFIRINOX (Treatment) (n=20) demonstrating statistically significant PFS of 15 months vs. 5.8 months in SOC-FFX control group (p<0.001). SOC-FFX control group (n=37) were treated with FOLFIRINOX alone at the study site in the four years preceding the clinical trial. SOC-FFX control group: Standard of Care control patients who received FOLFIRINOX alone in the first line. Legend: Control (Red Line) – SOC-FFX Control Patients; Treatment (Blue line) - Salmonella-IL2 with FOLFIRINOX.
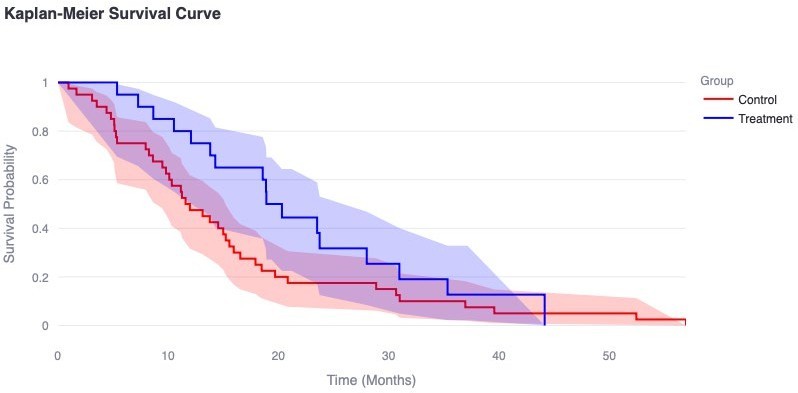
Figure 2. Median Overall Survival (mOS) of study compliant and Expanded Access Program patients who received greater than five doses of Salmonella-IL2 with FOLFIRINOX (n=20) demonstrating statistically significant mOS of 20.3 months vs. 11.5 months in SOC-FFX control group (p<0.05). SOC-FFX control group(n=37) were treated with FOLFIRINOX alone at the study site in the four years preceding the clinical trial. SOC-FFX control group: Standard of Care control patients who received FOLFIRINOX alone in the first line. Legend: Control (Red Line) – SOC-FFX Control Patients; Treatment (Blue line) - Salmonella-IL2 with FOLFIRINOX.
Salmonella-IL2 with Gemcitabine/nab Paclitaxel
Of the eight patients who received Salmonella-IL2 with Gemcitabine/nab Paclitaxel, one patient received only two doses of the study drug, so seven patients were analyzed in this group. The mPFS was six months in study patients compared to 3.6 months in SOC-Gem/nabP control patients (p=0.4) and the mOS was 8.6 months in both the study (GEM/nabP) arm and 9.1 months in SOC-Gem/nabP controls (p=0.58). Although there was a slight increase in mPFS with the addition of Salmonella-IL2, given the small numbers of enrolled patients in this arm, conclusions regarding effectiveness were not possible.
Biomarker analysis
CA19-9 and CEA levels were drawn on every study participant every 3 months. CA19-9 was the more predominant biomarker that demonstrated elevation when compared to CEA for the diagnosis of pancreatic cancer. Specifically, a downward trend was observed with treatment with Salmonella-IL2 with FOLFIRINOX for both biomarkers and rose accordingly with disease progression (data not shown).
Safety
There were 41 serious adverse events (SAE) reported during the trial. Of these 41 events, only one (dehydration) was initially attributed to use of the study drug. On secondary review the principal investigator and the DSMC concluded that this case of dehydration would likely be more attributable to chemotherapy rather than the study drug (Table 3).
|
S. No |
SAE Description |
Occurrence |
|
1 |
Abdominal Pain |
3 |
|
2 |
Ascites |
1 |
|
3 |
Biliary Infection |
1 |
|
4 |
Bowel Obstruction |
1 |
|
5 |
Biliary Obstruction |
1 |
|
6 |
Cholangitis |
2 |
|
7 |
Dehydration |
2 |
|
8 |
Diarrhea |
1 |
|
9 |
Fatigue |
1 |
|
10 |
Febrile Neutropenia |
2 |
|
11 |
Fever |
5 |
|
12 |
Hematemesis |
1 |
|
13 |
Jaundice |
1 |
|
14 |
Mucositis |
1 |
|
15 |
Nausea |
2 |
|
16 |
Neutropenia |
1 |
|
17 |
Neutropenic Sepsis |
1 |
|
18 |
Pancolitis |
1 |
|
19 |
Peripheral Sensory Neuropathy |
1 |
|
20 |
Probable Cholangitis |
1 |
|
21 |
Pulmonary Embolism |
3 |
|
22 |
Sepsis |
2 |
|
23 |
Severe Pain Radiating to the Back |
1 |
|
24 |
Syncope |
1 |
|
25 |
Tachycardia |
1 |
|
26 |
Vomiting |
3 |
|
Total |
41 |
Discussion
Stage IV pancreatic cancer is characterized by an extremely poor prognosis and alternatives to standard of care therapies are desperately needed. Currently, the standard of care is either use of a four-drug chemotherapeutic regimen (FOLFIRINOX) or a two-drug regimen (Gemcitabine/nab Paclitaxel) [2,3]. In 2011, Conroy, et al. reported a comparison of FOLFIRINOX and Gemcitabine alone, finding a significant increase in both OS and PFS for FOLFIRINOX, a result that ultimately led to the addition of nab Paclitaxel to Gemcitabine [27]. As previously stated, a recent meta-analysis of seven trials encompassing a total of 2,581 patients revealed a median PFS that ranged from 5.7–7.4 months and a median OS that ranged from 10.4–11.7 months regardless of the drug regimen used to treat metastatic pancreatic cancer [4]. Given that there have been no clinically significant approved improvements of metastatic pancreatic cancer therapies over the last 15 years, the critical need for innovation in therapeutic strategies is obvious. The present non-randomized, two arm phase II clinical study demonstrated a statistically significant increase in both median progression free survival and median overall survival when patients were administered greater than 5 doses of Salmonella-IL2 was given with FOLFIRINOX. Recruitment into the FOLFIRINOX arm was better than for the Gemcitabine/nab Paclitaxel arm and it is not possible to draw conclusions about the impact of adjunctive Salmonella-IL2 use in the latter arm. In addition, we learned that Gemcitabine possesses anti-microbial activity thus, is not the ideal candidate to be combined with any bacterial based immunotherapeutic [24].
To date, immunotherapeutic strategies have found limited success in achieving either meaningful overall or progression free survival in advanced pancreatic cancer [28,29]. Bacterial based immunotherapy potentially represents a paradigm shift in treating malignancies [6]. The unique propensity to colonize a solid tumor microenvironment and deliver a micro-factory that produces the immune modulating protein IL-2 in a nontoxic manner is especially attractive for pancreatic cancer. Salmonella-IL2 appears to be consistently successful in both preclinical experimentation and observational clinical studies. A multifactorial impact has been observed in tumor cell destruction with this treatment strategy. Multiple preclinical tumor models (pancreatic cancer, colorectal carcinoma, breast cancer, neuroblastoma and osteosarcoma) consistently demonstrate robust tumor colonization by Salmonella-IL2, a release of IL-2 into the tumor microenvironment, and subsequent immune cell mediated tumor cell killing [10–14].
In addition, in a recent phase I trial in humans with metastatic GI cancers who were administered only one dose of Salmonella-IL2, a statistically significant increase in peripheral blood NK and NK-T cell populations after Samonella-IL2 administration was observed [17]. Furthermore, preclinical experiments using this attenuated strain of Salmonella without the IL-2 gene demonstrated colonization and growth within the tumor microenvironment as it initiated a bystander immune-mediated tumor destruction [11–15]. The addition of IL-2 to this organism further enhances the observed immune mediated tumor destruction. Lastly, these rapidly growing bacteria appear to compete for nutrient resources and may essentially starve cancer cells [30]. Preclinical study has also demonstrated a synergy with Salmonella-IL2 and chemotherapy [31]. Specifically, it has been shown that an equivalent tumor cell kill can be achieved in a preclinical murine model of breast cancer when maximum tolerated dosing (MTD) of Doxorubicin is compared to a 75% reduction in Doxorubicin when Salmonella-IL2 is added to the therapy regimen.
Anecdotally, we observed that patients in the present clinical trial who were administered modified dosing of FOLFIRINOX (because of either chemo holidays, and/or eliminating oxaliplatin, and/or reduced dosing of 5-FU and/or Irinotecan) rather than MTD FOLFIRINOX experienced less serious adverse events and fared better in both progression free survival and overall survival. This association was not statistically significant.
Similar to experiences with other immune therapies, a minimum number of doses is required to observe a therapeutic effect of Salmonella-IL2 [32,33]. We determined that greater than five doses were required to observe sustained increases in both progression free survival and overall survival. Unlike other immunotherapies, no serious adverse events were observed in our observational clinical trial.
Recent successes of targeted mRNA vaccine therapies for resected pancreatic cancer demonstrate that in some contexts, immune-based therapeutics can have a beneficial impact [34]. However, this approach is useful only with early diagnosis of resectable lesions. Moreover, its use requires that a specific vaccine be created for each patient and this requires a resected specimen for the manufacture of the vaccine. In sharp contrast, Salmonella-IL2 indiscriminately targets solid cancers and its use does not require a costly, patient-specific manufacturing process [6,8–17].
The present study demonstrates the promising potential of using Salmonella-IL2 with FOLFIRINOX for metastatic pancreatic cancer therapy. However, this trial had limitations that include its nonrandomized design which inherently cannot allow for correcting confounding variables or preventing selection bias. In addition, the use of a historical control group and the number of enrolled patients are limitations. The addition of Expanded Access Program patients to the formal study patients might be considered a limitation, but given the limited number of patients with stage IV pancreatic cancer at a single site, “real-world” evidence generated from these added patients created an opportunity to analyze the study drug in an accepted, efficient, and cost effective manner [35]. The statistical methods employed—Kaplan-Meier estimation, log-rank testing, and Cox regression modeling—are standard and well-validated approaches for survival analysis in oncology. Although the observational design and reliance on historical controls limit the capacity for causal inference, these methods provide robust and transparent descriptive comparisons that support the interpretation of observed differences in OS and PFS between the patients treated with Salmonella-IL2 plus FOLFIRINOX and those who received FOLFIRINOX alone. Lastly, although robust tumor colonization by Salmonella-IL2 has been demonstrated in six preclinical tumor models, tumor sampling to culture for the presence of Salmonella-IL2 of enrolled patients while on treatment was not conducted. In addition, peripheral immune effector cell population data were also not collected in our study. Lastly, gemcitabine has known antimicrobial activity and could be the etiology of the limited therapeutic effectiveness observed in the small number of patients enrolled in the Gemcitabine arm of the clinical trial [36].
This phase II clinical trial is the first of its kind to examine the adjunctive addition of a genetically engineered bacteria that delivers an immune modulator with SOC chemotherapy for widely metastatic pancreatic cancer. In addition to both Fast Track Designation and Orphan Drug Designation for Salmonella-IL2 by the US FDA and given these promising and compelling reported results with a significant safety profile, a planned phase 3 study will be a global, multisite, randomized controlled trial designed to facilitate Biologics License Application compliance from the US Food and Drug Administration and other regulatory agencies throughout the world.
Acknowledgements
This clinical trial and the extensive amount of research and support to develop Salmonella-IL2 would not have been possible without the support of many. The concept of bacterial based cancer therapy and specifically Salmonella-IL2 requires a paradigm shift in one’s thinking and belief on how cancer should be treated. Specifically, research support from the NIH’s R-2CA131194 which funded the preliminary data that ultimately led to this clinical trial. In addition, support from Weist Family Foundation, the A. S. Leonard Endowed Chair at the University of Minnesota, the A.S. Leonard Cancer Research Foundation, and Project Stealth at the University of Minnesota created by Max Duckler, Judy Kessel, Jerrold Gershone and a host of extremely dedicated individuals at StoneArch Creative. Lastly, the selfless commitment by the Data Safety and Monitoring Committee that oversaw this clinical trial, specifically, Max Duckler, Dr. Jimmy Levine, Dr Steven Robinson, and Dr. Chris Moertel.
This phase II clinical trial study was sponsored by Salspera, Inc; Gerald Batist MD served as the principal investigator of this phase II clinical trial.
Conflicts of Interest Disclosure
Dr. Daniel Saltzman is a Professor of Surgery and Pediatrics and the Chief of Pediatric Surgery at the University of Minnesota. The therapeutic technology that is the subject of this manuscript was developed in his laboratory. Dr. Saltzman is also the co-founder and chief medical officer of Salspera. Salspera is a biotechnology company centered around bacterial based immunotherapeutics and hold the patents for Salmonella-IL2. This conflict has been extensively disclosed and is managed by the Office of Conflict Administration at the University of Minnesota.
Dr. Eddie Moradian is the co-founder and CEO of Salspera.
Mr. Jordan Moradian is a content expert in biostatistics and is a consultant for Salspera.
References
2. Mizrahi JD, Surana R, Valle JW, Shroff RT. Pancreatic cancer. Lancet. 2020 Jun 27;395(10242):2008–20.
3. Klein-Brill A, Amar-Farkash S, Lawrence G, Collisson EA, Aran D. Comparison of FOLFIRINOX vs Gemcitabine Plus Nab-Paclitaxel as First-Line Chemotherapy for Metastatic Pancreatic Ductal Adenocarcinoma. JAMA Netw Open. 2022 Jun 1;5(6):e2216199.
4. Nichetti F, Rota S, Ambrosini P, Pircher C, Gusmaroli E, Droz Dit Busset M, et al. NALIRIFOX, FOLFIRINOX, and Gemcitabine With Nab-Paclitaxel as First-Line Chemotherapy for Metastatic Pancreatic Cancer: A Systematic Review and Meta-Analysis. JAMA Netw Open. 2024 Jan 2;7(1):e2350756.
5. Cereda V, D'Andrea MR. Pancreatic cancer: failures and hopes-a review of new promising treatment approaches. Explor Target Antitumor Ther. 2025 Mar 18;6:1002299.
6. Forbes NS, Coffin RS, Deng L, Evgin L, Fiering S, Giacalone M, et al. White paper on microbial anti-cancer therapy and prevention. J Immunother Cancer. 2018 Aug 6;6(1):78.
7. Duong MT, Qin Y, You SH, Min JJ. Bacteria-cancer interactions: bacteria-based cancer therapy. Exp Mol Med. 2019 Dec 11;51(12):1–15.
8. Saltzman DA, Heise CP, Hasz DE, Zebede M, Kelly SM, Curtiss R 3rd, et al. Attenuated Salmonella typhimurium containing interleukin-2 decreases MC-38 hepatic metastases: a novel anti-tumor agent. Cancer Biother Radiopharm. 1996 Apr;11(2):145–53.
9. Saltzman DA, Katsanis E, Heise CP, Hasz DE, Vigdorovich V, Kelly SM, et al. Antitumor mechanisms of attenuated Salmonella typhimurium containing the gene for human interleukin-2: a novel antitumor agent? J Pediatr Surg. 1997 Feb;32(2):301–6.
10. Saltzman DA, Katsanis E, Heise CP, Hasz DE, Kelly SM, Curtiss R 3rd, et al. Patterns of hepatic and splenic colonization by an attenuated strain of Salmonella typhimurium containing the gene for human interleukin-2: a novel anti-tumor agent. Cancer Biother Radiopharm. 1997 Feb;12(1):37–45.
11. Soto LJ, Sorenson BS, Nelson BW, Leonard AS, Saltzman DA. Generation of immunity to hepatic metastases by attenuated Salmonella typhimurium. Ann Surg Onc. 2004;11(2)suppl: S107.
12. Soto LJ 3rd, Sorenson BS, Kim AS, Feltis BA, Leonard AS, Saltzman DA. Attenuated Salmonella typhimurium prevents the establishment of unresectable hepatic metastases and improves survival in a murine model. J Pediatr Surg. 2003 Jul;38(7):1075–9.
13. Soto LJ 3rd, Sorenson BS, Nelson BW, Solis SJ, Leonard AS, Saltzman DA. Preferential proliferation of attenuated Salmonella typhimurium within neuroblastoma. J Pediatr Surg. 2004 Jun;39(6):937–40; discussion 937–40.
14. Barnett SJ, Soto LJ 3rd, Sorenson BS, Nelson BW, Leonard AS, Saltzman DA. Attenuated Salmonella typhimurium invades and decreases tumor burden in neuroblastoma. J Pediatr Surg. 2005 Jun;40(6):993–7.
15. Sorenson BS, Banton KL, Frykman NL, Leonard AS, Saltzman DA. Attenuated Salmonella typhimurium with IL-2 gene reduces pulmonary metastases in murine osteosarcoma. Clin Orthop Relat Res. 2008 Jun;466(6):1285–91.
16. Fritz SE, Henson MS, Greengard E, Winter AL, Stuebner KM, Yoon U, et al. A phase I clinical study to evaluate safety of orally administered, genetically engineered Salmonella enterica serovar Typhimurium for canine osteosarcoma. Vet Med Sci. 2016 Jun 6;2(3):179–90.
17. Gniadek TJ, Augustin L, Schottel J, Leonard A, Saltzman D, Greeno E, et al. A Phase I, Dose Escalation, Single Dose Trial of Oral Attenuated Salmonella typhimurium Containing Human IL-2 in Patients With Metastatic Gastrointestinal Cancers. J Immunother. 2020 Sep;43(7):217–21.
18. Eisenhauer EA, Therasse P, Bogaerts J, Schwartz LH, Sargent D, Ford R, et al. New response evaluation criteria in solid tumours: revised RECIST guideline (version 1.1). Eur J Cancer. 2009 Jan;45(2):228–47.
19. NCI Guidelines for Investigators: Adverse Event Reporting Requirements for DCTD (CTEP and CIP) and DCP INDs and IDEs [Internet]. Bethesda (MD): National Cancer Institute; 2024. Available from: https://ctep.cancer.gov/protocoldevelopment/electronic_applications/docs/aeguidelines.pdf.
20. WMA Declaration of Helsinki – Ethical Principles for Medical Research Involving Human Participants [Internet]. Ferney-Voltaire: World Medical Association; 2024. Available from: https://www.wma.net/policies-post/wma-declaration-of-helsinki/?utm_source.
21. Marion JD, Althouse AD. The Use of Historical Controls in Clinical Trials. JAMA. 2023 Oct 17;330(15):1484–5.
22. Harun N, Gupta N, McCormack FX, Macaluso M. Dynamic use of historical controls in clinical trials for rare disease research: A re-evaluation of the MILES trial. Clin Trials. 2023 Jun;20(3):223–34.
23. Green AK, Reeder-Hayes KE, Corty RW, Basch E, Milowsky MI, Dusetzina SB, et al. The project data sphere initiative: accelerating cancer research by sharing data. Oncologist. 2015 May;20(5):464–e20.
24. Jordheim LP, Ben Larbi S, Fendrich O, Ducrot C, Bergeron E, Dumontet C, et al. Gemcitabine is active against clinical multiresistant Staphylococcus aureus strains and is synergistic with gentamicin. Int J Antimicrob Agents. 2012 May;39(5):444–7.
25. Curtiss R 3rd, Kelly SM. Salmonella typhimurium deletion mutants lacking adenylate cyclase and cyclic AMP receptor protein are avirulent and immunogenic. Infect Immun. 1987 Dec;55(12):3035–43.
26. Galán JE, Nakayama K, Curtiss R 3rd. Cloning and characterization of the asd gene of Salmonella typhimurium: use in stable maintenance of recombinant plasmids in Salmonella vaccine strains. Gene. 1990 Sep 28;94(1):29–35.
27. Muhammad S, Fan T, Hai Y, Gao Y, He J. Reigniting hope in cancer treatment: the promise and pitfalls of IL-2 and IL-2R targeting strategies. Mol Cancer. 2023 Jul 29;22(1):121.
28. Conroy T, Desseigne F, Ychou M, Bouché O, Guimbaud R, Bécouarn Y, et al. FOLFIRINOX versus gemcitabine for metastatic pancreatic cancer. N Engl J Med. 2011 May 12;364(19):1817–25.
29. Yoon JH, Jung YJ, Moon SH. Immunotherapy for pancreatic cancer. World J Clin Cases. 2021 May 6;9(13):2969–82.
30. Ju Y, Xu D, Liao MM, Sun Y, Bao WD, Yao F, et al. Barriers and opportunities in pancreatic cancer immunotherapy. NPJ Precis Oncol. 2024 Sep 12;8(1):199.
31. Kedia-Mehta N, Finlay DK. Competition for nutrients and its role in controlling immune responses. Nat Commun. 2019 May 9;10(1):2123.
32. Saltzman D, Augustin L, Leonard A, Mertensotto M, Schottel J. Low dose chemotherapy combined with attenuated Salmonella decreases tumor burden and is less toxic than high dose chemotherapy in an autochthonous murine model of breast cancer. Surgery. 2018 Mar;163(3):509–14.
33. Borcoman E, Nandikolla A, Long G, Goel S, Le Tourneau C. Patterns of Response and Progression to Immunotherapy. Am Soc Clin Oncol Educ Book. 2018 May 23;38:169–78.
34. Le Louedec F, Leenhardt F, Marin C, Chatelut É, Evrard A, Ciccolini J. Cancer Immunotherapy Dosing: A Pharmacokinetic/Pharmacodynamic Perspective. Vaccines (Basel). 2020 Oct 31;8(4):632.
35. Rojas LA, Sethna Z, Soares KC, Olcese C, Pang N, Patterson E, et al. Personalized RNA neoantigen vaccines stimulate T cells in pancreatic cancer. Nature. 2023 Jun;618(7963):144–50.
36. Wasser JS, Greenblatt DJ. Applying real-world data from expanded-access ("compassionate use") patients to drug development. J Clin Transl Sci. 2023 Aug 7;7(1):e181.