Abstract
Keeping positive mental health is essential, as it promotes overall wellness, strengthens endurance, nurtures significant relationships, and provides a framework for personal as well as professional fulfilment. The present research investigates the complex associations between prosocial behavior, aggression, and positive mental health in a range of social conditions with the aim of discovering subtle variations influenced by age groups, gender, and the type of residence. In this study, 405 participants were recruited using multi-stage random sampling. Descriptive and correlation statistical analyses are evaluated to discover gender, age, and residence-based distinct groups that varied in prosocial behavior, aggression and positive mental health. Descriptive statistics reveal distinct differences in verbal aggression, hostility, and prosocial behavior based on gender, residence, and age groups. While certain aggressive behaviors showed no correlation with positive mental health, the overall patterns highlight significant relationships between prosocial behavior, aggression, and mental well-being across diverse factors. This research presents an in-depth viewpoint on the complex interrelationships influencing positive mental health, providing a significant understanding of the discipline through its comprehensive inquiry and extensive evaluation.
Keywords
Positive mental health, Prosocial behavior, Aggression, Gender
Introduction
Positive mental health is greatly enhanced by prosocial behavior [1], which is defined as behavior meant to help others [2]. Practicing compassion, sharing, and kindness not only improves the quality of life of those who are receiving support but also makes the provider seem fulfilled and happy. Positive relationships with others have been associated with higher happiness, lower stress levels, and a stronger sense of interpersonal connection [3]. On the other hand, aggressiveness, which is characterized by harm or hostile behavior, has an adverse effect on mental health. People with aggressive tendencies can be more stressed and anxious and have poor relationships with others [4]. A supportive social context is created by fostering prosocial behavior and reducing aggressiveness, which benefits both individual and community mental health outcomes. Promoting an atmosphere of empathy and kindness can act as an effective stimulant for enhancing mental health and building strong, harmonious communities [4].
Prosocial behavior
All prosocial behavior and violence are enduring elements of human behavior that demonstrate an obvious pattern from middle childhood to adulthood [5]. Prosocial behavior is beneficial for both those giving and receiving support. Prosocial behaviors that benefit both individuals or generate positive emotions are beneficial to the welfare of the provider [6]. According to earlier studies, prosocial behavior is positively correlated with better interactions with others, stronger psychological well-being, and better physical health with a longer life expectancy. Prosocial behavior, such as altruism or helping others without expecting reimbursement, is crucial for having a healthy, long life [7]. In our history, there have also been several fewer recognized instances of kindness, sharing, helping, and donating. Strongly adopted, people with these prosociality-based principles are likely to act mainly to help others in need. Today, we have to start our daily activities with knowledge about many antisocial behaviors, such as actions of violence, human hostility, hijackings, and injustice, some of which may even impact us personally. Through human history, there have been numerous instances of cruelty, racial violence, torture, war, crime, and murder. During the past few decades, there has been a lot of research done regarding the development and correlations of prosocial behaviors [8,9]. It is remarkable that there are now barely any measures available for investigating prosocial behaviors, particularly among adult and elderly individuals, considering the importance of comprehending behaviors that contribute to society. There are plenty of evaluations; however, they are usually characterized by an expansive perspective of prosocial behavior. Investigators have still demonstrated that prosocial behaviors come in a broad range of patterns and that these forms communicate with theoretically related dimensions in specific manners [10,11]. Moreover, little is known regarding the characteristics of adults who demonstrate specific prosocial behavioral tendencies [12]. The main goal of this study was to investigate the psychometric qualities of a previously developed, multidimensional evaluation that evaluates prosocial behaviors in adults.
Types of prosocial behaviors
The following types of prosocial behaviors were first notable, based on previous theory and research: public prosocial behaviors, altruistic prosocial behaviors, compliant prosocial behaviors, and emotional prosocial behaviors. Each type's description is presented below.
Altruism: According to Pfattheicher et al., 2022, altruistic prosocial behaviors can be described as spontaneous acts of helping that are mainly motivated by an awareness of the requirements and welfare of others [13]. They are frequently spurred on by empathetic responses and adopted requirements that are consistent with helping others. In addition, these actions may come at an expense to the helper since their primary concern is maintaining the health of the individuals in need. While the existence of altruistic behaviors has been denied by academics, there are at least three pieces of research that point to the existence of altruism [11,14]. First, it has been shown by researchers that empathy is transmissible and regarded as evolutionary advantageous [15,16]. Second, research conducted over time has demonstrated that the prosocial behavior tendency is consistent throughout life [17,18]. Third, studies in various situations have revealed significant associations between personality traits and acts of kindness [19,20]. Scholars have proposed that empathy generates a need to ease the distress of the other person, whereas emotional distress leads to a desire to relieve one's own sense of distress [21]. A number of studies have discovered that altruistic behaviors are associated with sympathy, whereas egoistic responses are tied to individual discomfort [22]. So, it had been expected that mature adults who attributed responsibility to themselves and who were motivated to behave properly towards society would be more likely to support altruistic, prosocial actions.
Compliant: According to Rossi et al., 2023, compliant prosocial behaviors include those in which one helps others in response to a request, either verbal or nonverbal [23]. The vast majority of research on compliant helping has been conducted with children rather than adults, and it is more frequent than spontaneous helping. According to Pastor et al., 2024, adolescents who collaborate often are more inclined to take care of things, ask for help from adults more frequently, and react positively to their peers' prosocial behaviors [24]. When girls comply with requests to take prosocial behavior, teachers, on the other hand, tend to respond with greater favor to their actions than to boys. The particular characteristics associated with compliant support aren't restricted to preschool years; compliant prosocial behavior has been related to typically nonassertive elementary school children [25].
Emotional: A perspective towards supporting others in challenging situations was an understanding of emotional prosocial behaviors. There are specific situations where support can be extremely emotionally draining. Highly emotionally charged situations may cause overarousal and personal discomfort in particular individuals, while they can provoke sympathy in others [26]. These emotional reactions have been linked to both self-centered and altruistic methods of helping as well as controlling one's emotional capabilities [27]. Helping in highly stressful circumstances is generally believed to be closely associated with others personal characteristics and sympathetic responses [28].
Public
Engaging in prosocial actions in public might be motivated, at least partly, by the desire to boost one's self-worth and gain other people's acceptance and respect. Adjusting whether or not other individuals are witnesses to the possible prosocial act is a standard manipulation used in research on prosocial behavior [29]. Although prosocial behavior and socially desirable considerations are not always incompatible, research has shown that helping others in public is occasionally linked to self-centered motivations. In addition, performing deeds in front of an audience increases the probability of being supported [30]. Since people are frequently anxious about obtaining approval from others, it was suggested that public prosocial behaviors would positively correlate with social desirability and approval-oriented moral reasoning.
Anonymous and dire
The public prosocial behaviors subscale is integrated into two distinct components, public and anonymous prosocial behaviors, based on preliminary factor analyses from three pilot inquiries. Anonymous prosocial behavior is defined as delivering support without revealing the identity of the beneficiary. Public prosocial behaviors were defined as a propensity to engage in prosocial behavior in public. Additionally, the subscale measuring emotional prosocial behaviors is integrated into two distinct factors: serious and emotional prosocial behaviors. Respondents established the distinction between situations that involve emotionally charged indicators and those that require crisis or emergency assistance.
Aggression
The act of harming someone who does not want to be hurt is referred to as aggression [31]. Frustration was the reason for the aggression, defined as an unpleasant feeling that develops when something stands in the way of achieving an important goal [32]. According to the frustration-aggression theory, all painful events result in negative impact, which in effect promotes aggressive and frightened preferences. It is not so much the feeling of dissatisfaction as it is the unpleasant feeling that evokes aggressive behavior [31,33]. In the context of influenced stimulation, archer split stimuli that generated fear or aggression into three groups: pain, novelty, and frustration. He also defined looming, which is the term for an object that shifts swiftly towards a subject's sense of sight and can be categorized according to its magnitude. Numerous classifications and aspects related to aggression have been suggested. They involve the following factors: whether the aggression is verbal or physical; whether interpersonal aggression, such as bullying and social manipulation, takes place; whether or not harm to others is intended; whether the aggression is expressed actively or passively; and whether or not it targets others directly or indirectly. Emotions and mental states linked to aggression may also be incorporated into the classification. Both social and non-social stressors are capable of triggering aggression, and there may be a significant connection between aggression and coping mechanisms for stress. It is feasible to behave aggressively in an effort to intimidating. Political or moral beliefs may influence the practical meaning of aggression. Problems with adjustment and an array of psychopathological symptoms, notably antisocial behaviors, personality disorder, borderline personality disorder, and intermittent explosive disorder are linked to aggressive behaviors. According to biological perspectives, aggressiveness is a result of hormone variations, natural selection during evolution, internal energy generated in response to stimuli from the outside, and heredity. According to psychological viewpoints, aggression originates from a variety of variables that affect both personal and situational settings, including a constructive instinctive reaction to frustration, an affect prompted by negative stimuli, noticeable social learning, as well as different reinforcements.
Positive mental health
The term "positive mental health" was first coined by Marie Jahoda, who characterized it as "a less permanent function of personality and the social situation" or "an enduring personality characteristic" [34]. Being positive and mentally well is a lot more than not having psychopathology, a lack of mental wellness, or mental health circumstances such as anxiety or depression; it also means getting a feeling of purpose, being able to maintain relationships, being content, and substantially engaging with life. A crucial component of mental wellness involves maintaining a positive mental state. Positive characteristics like satisfaction, a sense of purpose, maintaining significant relationships, and enjoying life to the fullest are essential elements of mental health. The World Health Organization (2022) defines positive mental health, additionally referred to as good mental health, as a state of wellbeing where people are able to reach their individual potential, work effectively, overcome everyday challenges, and beneficially impact the community [35]. Sapranaviciute et al., (2022) described well-being as a person's psychological state or assessment of satisfaction and pleasure with their own lifestyles [36]. Psychological well-being encourages people to continue pursuing advantageous behaviors for both themselves and other members of the community [37]. Focusing on the "Mental Health (2013–2020)" action strategy, the World Health Organization (WHO) has characterized positive mental health as an aspect of emotional and psychological well-being that enables an individual to become creative by realizing their potential and addressing their own requirements [35]. Psychological well-being is referred to essentially by Patnaik, (2021) as including matters such as happiness, trustworthiness, the ability to control needs or requirements, fulfilment with the resources at hand, being in good physical or mental health, and overall life satisfaction [38]. The ability to form beneficial connections with other people, environmental mastery, autonomy, self-acceptance, and personal advancement are the six elements of psychological well-being defined by Hossen & Salleh, (2024) [39]. This definition expanded the idea of mental health beyond merely the absence of psychological disorders and comprised the existence of positive characteristics, contributing to significant improvements in the field's research and application. They observed that those who practiced had a great deal of consensus. Along with how you feel about yourself, mental and psychological well-being additionally involves how you manage external factors and the quality of your relationships. It's essential to keep in mind that experiencing good mental health encompasses more than just preventing mental health conditions like anxiety or sadness. Maintaining care for our mental health may help in the prevention or treatment of psychological disorders that are occasionally associated with over-time illnesses of the body. Subjective mental health, or psychological well-being, can be affected by a variety of multidimensional variables that encompass mental, emotional, and cognitive aspects, as documented by Nicolini et al., (2021) [40].
According to a study conducted by Tekin et al., (2021), individuals who lack empathy have little interest in prosocial behavior such as altruism and have few chances to engage in altruistic activities such as sharing, helping, donating, and successfully taking care of others [41]. Women are more likely than men to participate in prosocial behaviors, or helping others, in accordance with Kamas & Preston, (2021) experimental findings [42]. In accordance with Singh and Teoh (2014), there is a strong, positive, and significant association between altruistic behavior and the mental health of teenage senior secondary students [43]. According to Feng et al. (2020) and Sparrow et al., (2021), there is a beneficial relationship between mental health concerns and altruism [44,45]. As stated by Fullen et al., (2022), helping provider’s mental health is more affected by their helping acts compared to that of help beneficiaries [46]. Prosocial behavior, such as charitable giving and helping others, is an excellent gauge of mental health, as shown by Hirani et al., 2022 [47]. In the opinion of Aknin et al. (2015), contributing to others has some pleasurable consequences and makes the donors feel good [48]. Beneficial behaviors and kind feelings have a strong connection with our health (mental and physical), well-being, and life span [49]. People who are physically or mentally stressed by the demands of others and who have expertise in significant negative health outcomes, such as dementia, are the ones who are physically or mentally overwhelmed [50,51]. According to Marks et al., (2024), many different kinds of human behaviors and feelings are being studied in a conventional approach in an effort to encourage health and prevent disease [52]. Altruism, or selfish affection, is essential for mental, moral, and physical health, as stated by Kaufman & Jauk (2020) [53]. In accordance with more recent studies, volunteering is positively correlated with mental health [54,55]; additional positive correlations consist of blood donation [56], providing money or wealth to charity [57], and deeper life spans in elderly people [58]. Males are significantly more likely than girls to act aggressively [59,60]. Men seemed to score higher on items related to verbal and physical aggression, as opposed to the marginally stronger gender differences for anger and hostility [61,62]. Additional studies revealed that girls exhibited noticeably more aggression than boys [60,63].
The objectives of this research are to shed light on the complex connections present in various social contexts between prosocial behavior, aggression, and positive mental health. By analyzing the relationships among prosocial behavior, aggression, and positive mental health, the research attempts to discover specific variations influenced by age groups, gender, and type of location. By investigating the possible moderating impact of gender, residency, and age on the complex relationships between these behavioral traits and positive mental health, the research employs an in-depth strategy. The study aims to provide insights through this extensive investigation that can assist in establishing social policies, promoting targeted interventions, and driving mental health promotion activities that are tailored to address the specific needs of people across numerous demographic dimensions. In the end, the findings of this study offer the potential to generate significant improvements to the overall advancement of mental health in a wide range of circumstances.
Methodology
Participants
A total of 405 participants were in the investigation's sample. Participants had been selected from several Bangladeshi cities, including Bogura, Sirajganj, Naogaon, and Chapainawabganj (see details in Figure 1). Their age ranged from 30 to 75 years (215 men, 190 women; M age=48, SD=11.61). A multi-stage random sampling approach was employed in this study for selecting study participants.
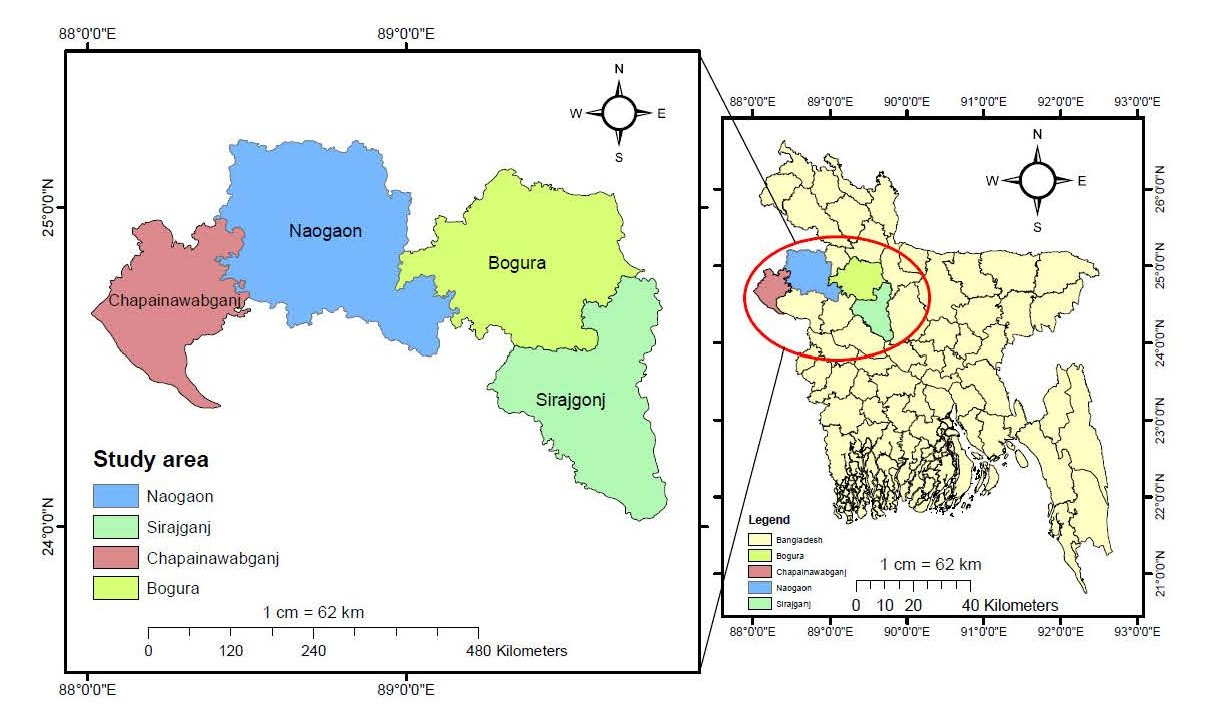
Figure 1. Research area of this study
Instruments
Prosocial tendencies measure: The prosocial tendencies measure (PTM) is a multifaceted scale that includes 23 items [64,65]. It can be classified through 6 subscales: public (4 items, Cronbach's α = 0.78), anonymous (5 items, Cronbach's α = 0:85), dire (3 items, Cronbach's α = 0:63), emotional (4 items, Cronbach's α = 0:75), compliant (2 items, Cronbach's α = 0:80), and altruism (5 items, Cronbach's α = 0:74). On a 5-point scale ranging from 1 (does not describe me at all) to 5 (describes me greatly), participants were tasked with assessing how much the statements represented them. For the sole purpose of this study, the PTM was adapted into Bengali, and its validity and reliability were evaluated.
Brief aggression questionnaire: This is a simplified and altered version of the 29-item Aggression Questionnaire [66]. The original BAQ featured four subscales: physical aggression, verbal aggression, anger, and hostility, each containing three items. The BAQ currently includes twelve items. The only item with an opposite score is the number seven. There are five ratings on the response scale: 1 being very unusual of me and 5 being extremely characteristic of me. The Bangla version of the BAQ was employed in the current research [67]. Bangla version of the Brief Aggression Questionnaire also used many previous research in Bangladesh [68].
Positive mental health scale: A quick and easy single-dimensional instrument for analyzing mental health is the positive mental health scale (PMH). There is a total of nine Likert-type items on the scale. On a Likert scale, the PMH will range from 1 (not true) to 4 (true). A higher number implies the presence of greater mental health. The total score appears to range from 9 to 36. One-dimensionality, numerical consistency across samples and over time, great internal coherence, good retest reliability, good discriminate and convergent validity, and sensitivity to modification in treatment had all been demonstrated by the scale's investigators. Additionally, it appears that the PMH-Scale can, in actuality, measure a single concept and facilitate cross-group and cross-temporal score evaluations. Consequently, the PMH scale is a brief and simple to understand instrument for assessing PMH across an array of relevant groups. In addition, the PMH was adapted into Bangla, and its initial psychometric characteristics have been studied [69]. The International Test Commission's (ITC, 2017) guidelines were adhered to in the translation and adaptation procedures.
Procedure
The input from the respondents in the present investigation was gathered using randomized data collection procedures. First, a rapport was developed, and the objective of the research was made clear to the respondents. The previously mentioned devices were subsequently distributed to each respondent. They were given assurances about the privacy of their responses. Instructions were provided to the respondents to make sure they read the questionnaire items carefully and responded honestly. Additionally, they were told that there was neither a right nor incorrect answer to any of the questionnaire questions, which encouraged them to respond to all of the questions thoroughly. They provided explanations for any queries they may have had about how to respond to the questions or about the instructions. The respondents were directed to finish the work without wasting any of their time, despite the fact that there was no set time limitation. The task took an average of thirty minutes to accomplish. They were thanked for their genuine participation after completing the work.
Statistical analysis
The descriptive test, parametric analysis (t-test if the data normality was passed), and non-parametric analysis (u- test if the data normality was not passed) were among the statistical methods used for analyzing the data. For the purpose of enhancing the quality of our findings and providing a more accurate evaluation of the connections and dependencies among the collected data, correlation analysis has been applied in this study. GraphPad 8.0.1 was employed to interpret the data, providing a reliable and accurate statistical assessment of the findings of the study.
Results
A comprehensive analysis of descriptive statistics uncovers differences between verbal aggression and hostility, which fall into distinct groups based on gender (see details in Table 1). A detailed review of descriptive qualities according to residence indicates significant differences between seven separate groups: dire, anonymous, compliant, emotional, physical, verbal, and positive mental health (details in Table 2). An in-depth review of age based descriptive attributes showed distinctions among two main categories: positive mental health and anonymous (see Table 3 for more details).
|
|
Male (n= 215) |
Female (n= 190) |
p-Value |
Significance |
||||
|
Min. |
Max. |
Mean±SD |
Min. |
Max. |
Mean±SD |
|||
|
Altruism |
5 |
25 |
14.57±4.09 |
6 |
23 |
14.20±4.18 |
0.1500 |
ns |
|
Public |
4 |
20 |
9.46±3.01 |
4 |
17 |
8.92±2.54 |
0.1100 |
ns |
|
Dire |
3 |
15 |
8.61±2.29 |
4 |
15 |
8.59±2.23 |
0.6900 |
ns |
|
Anonymous |
5 |
25 |
15.01±5.40 |
5 |
25 |
15.36±4.89 |
0.4500 |
ns |
|
Compliant |
2 |
10 |
7.26±2.27 |
2 |
10 |
6.94±2.19 |
0.1000 |
ns |
|
Emotional |
4 |
20 |
12.22±2.98 |
6 |
20 |
12.37±2.71 |
0.7300 |
ns |
|
Physical Aggression |
3 |
15 |
7.22±2.45 |
3 |
15 |
7.09±2.54 |
0.4300 |
ns |
|
Anger |
3 |
15 |
8.41±1.94 |
5 |
15 |
8.26±1.87 |
0.4000 |
ns |
|
Verbal Aggression |
3 |
14 |
6.36±2.42 |
3 |
14 |
5.67±2.08 |
0.0040 |
** |
|
Hostility |
4 |
15 |
6.98±1.78 |
3 |
11 |
6.14±1.60 |
0.0001 |
*** |
|
Positive Mental Health |
9 |
36 |
26.00±5.06 |
12 |
45 |
25.94±4.77 |
0.7000 |
ns |
|
Note. SD: Standard Deviation; ns: not significant |
||||||||
|
|
Rural (n=205) |
Urban (n=200) |
p-value |
Significance |
||||
|
Min. |
Max. |
Mean±SD |
Min. |
Max. |
Mean±SD |
|||
|
Altruism |
5 |
23 |
14.38±3.40 |
5 |
25 |
14.42±4.76 |
0.6800 |
ns |
|
Public |
4 |
16 |
9.09±2.44 |
4 |
20 |
9.32±3.14 |
0.8800 |
ns |
|
Dire |
3 |
15 |
8.21±2.01 |
3 |
15 |
9.01±2.43 |
0.0007 |
*** |
|
Anonymous |
5 |
25 |
12.57±4.21 |
7 |
25 |
17.85±4.68 |
0.0001 |
*** |
|
Compliant |
2 |
10 |
6.83±2.46 |
3 |
10 |
7.40±1.95 |
0.0350 |
* |
|
Emotional |
4 |
20 |
11.73±2.79 |
4 |
20 |
12.87±2.82 |
0.0002 |
*** |
|
Physical Aggression |
3 |
15 |
7.68±2.49 |
3 |
15 |
6.63±2.38 |
0.0001 |
*** |
|
Anger |
3 |
15 |
8.34±1.59 |
3 |
15 |
8.40±2.12 |
0.8800 |
ns |
|
Verbal Aggression |
3 |
14 |
6.42±2.27 |
3 |
14 |
5.65±2.25 |
0.0001 |
*** |
|
Hostility |
3 |
14 |
6.48±1.60 |
3 |
15 |
6.70±1.88 |
0.4100 |
ns |
|
Positive Mental Health |
9 |
36 |
25.00±4.77 |
15 |
45 |
26.96±4.89 |
0.0001 |
*** |
|
Note. SD: Standard Deviation; ns: not significant |
||||||||
|
|
Group 1 (n=211) |
Group 2 (n=129) |
Group 3 (n=65) |
p-value |
Significance |
||||||
|
Min. |
Max. |
Mean±SD |
Min. |
Max. |
Mean±SD |
Min. |
Max. |
Mean±SD |
|||
|
Altruism |
5 |
25 |
14.82±4.28 |
6 |
25 |
14.05±4.04 |
5 |
23 |
13.70±3.68 |
0.1006 |
ns |
|
Public |
4 |
20 |
9.36±2.88 |
4 |
16 |
9.07±2.64 |
4 |
16 |
8.96±2.91 |
0.6643 |
ns |
|
Dire |
3 |
15 |
8.63±2.32 |
3 |
15 |
8.71±2.32 |
6 |
15 |
8.27±1.92 |
0.2857 |
ns |
|
Anonymous |
5 |
25 |
16.37±4.98 |
5 |
25 |
14.32±4.98 |
5 |
25 |
12.98±5.11 |
0.0001 |
*** |
|
Compliant |
2 |
10 |
7.35±2.05 |
2 |
10 |
6.94±2.23 |
2 |
10 |
6.67±2.73 |
0.1539 |
ns |
|
Emotional |
4 |
20 |
12.56±2.90 |
6 |
20 |
12.11±2.89 |
6 |
18 |
11.75±2.57 |
0.0714 |
ns |
|
Physical Aggression |
3 |
15 |
7.04±2.52 |
3 |
15 |
7.15±2.48 |
3 |
14 |
7.56±2.38 |
0.2582 |
ns |
|
Anger |
3 |
15 |
8.37±1.98 |
3 |
15 |
8.31±1.87 |
4 |
12 |
8.29±1.75 |
0.8524 |
ns |
|
Verbal Aggression |
3 |
14 |
5.91±2.33 |
3 |
13 |
6.06±2.19 |
3 |
14 |
6.38±2.35 |
0.2450 |
ns |
|
Hostility |
3 |
15 |
6.60±1.85 |
4 |
14 |
6.44±1.68 |
3 |
10 |
6.83±1.49 |
0.1023 |
ns |
|
Positive Mental Health |
9 |
45 |
27.01±4.67 |
13 |
36 |
25.54±4.25 |
11 |
36 |
23.43±5.90 |
0.0001 |
*** |
|
Note. SD: Standard Deviation; ns: not significant; Age Group 1: 30–45; Age Group 2: 46–60; Age Group 3: 61–75 |
|||||||||||
With the exception of verbal and physical aggression, Table 4 demonstrates an overall connection between prosocial behavior and aggression affecting positive mental health. A convoluted interaction between these factors appears in the extremely significant values exhibited by all the elements. Table 5 highlights the gender-based relationship between aggression, prosocial behavior, and positive mental health. Despite the exception of verbal and physical aggression for both males and females, all variables revealed significant variations, hinting at distinct patterns in the gender-based connection between these variables. The residence-based correlation between aggression, prosocial behavior, and positive mental health is shown in Table 6. It's interesting to note that the data shows no significant correlation between positive mental health and emotional prosocial behavior in rural areas and physical aggression, verbal aggression, and hostility in metropolitan areas and anger for both resident areas. But when these particular factors are excluded from the analysis, prosocial behavior, aggression, and positive mental health are consistently and significantly correlated in all residence-based interactions. The age-based relationships between aggression, prosocial behavior, and positive mental health are presented in Table 7. Additionally, the results show that there is no significant link between positive mental health and other characteristics, such as physical aggression in all age groups, hostility in age groups 2 and 3, anger in age group 3, and verbal aggression in all age groups. However, when these particular factors are removed from the research, a significant and consistent relationship between prosocial behaviour, aggression, and positive mental health remains applicable to all age groups.
|
Relationship |
r value |
CL-95% |
p-value |
Significance |
|
Altruism vs. PMH |
0.3744 |
0.2848 to 0.4576 |
0.0001 |
*** |
|
Public vs. PMH |
0.2956 |
0.2013 to 0.3845 |
0.0001 |
*** |
|
Dire vs. PMH |
0.2448 |
0.1481 to 0.3368 |
0.0001 |
*** |
|
Anonymous vs. PMH |
0.3964 |
0.3083 to 0.4777 |
0.0001 |
*** |
|
Compliant vs. PMH |
0.3640 |
0.2737 to 0.4480 |
0.0001 |
*** |
|
Emotional vs. PMH |
0.3335 |
0.2413 to 0.4198 |
0.0001 |
*** |
|
Physical Aggression vs. PMH |
0.0434 |
-0.0571 to 0.1431 |
0.3836 |
ns |
|
Anger vs. PMH |
0.2513 |
0.1549 to 0.3429 |
0.0001 |
*** |
|
Verbal Aggression vs. PMH |
0.0048 |
-0.0955 to 0.1051 |
0.9230 |
ns |
|
Hostility vs. PMH |
0.1797 |
0.0808 to 0.2750 |
0.0003 |
*** |
|
Note. PMH: Positive Mental Health; CL: Confidence Limit; ns: not significant * Statistically significant ** Very statistically significant *** Highly statistically significant r-value: Two variables correlation |
||||
|
Relationship |
Gender |
r value |
CL-95% |
p-value |
Significance |
|
Altruism vs. PMH |
Male |
0.331 |
0.203 to 0.448 |
0.0001 |
*** |
|
Altruism vs. PMH |
Female |
0.408 |
0.278 to 0.523 |
0.0001 |
*** |
|
Public vs. PMH |
Male |
0.256 |
0.123 to 0.380 |
0.0001 |
*** |
|
Public vs. PMH |
Female |
0.342 |
0.206 to 0.465 |
0.0001 |
*** |
|
Dire vs. PMH |
Male |
0.213 |
0.078 to 0.341 |
0.0016 |
** |
|
Dire vs. PMH |
Female |
0.275 |
0.134 to 0.405 |
0.0001 |
*** |
|
Anonymous vs. PMH |
Male |
0.395 |
0.272 to 0.505 |
0.0001 |
*** |
|
Anonymous vs. PMH |
Female |
0.399 |
0.268 to 0.515 |
0.0001 |
*** |
|
Compliant vs. PMH |
Male |
0.319 |
0.190 to 0.438 |
0.0001 |
*** |
|
Compliant vs. PMH |
Female |
0.413 |
0.284 to 0.528 |
0.0001 |
*** |
|
Emotional vs. PMH |
Male |
0.340 |
0.213 to 0.457 |
0.0001 |
** |
|
Emotional vs. PMH |
Female |
0.318 |
0.179 to 0.443 |
0.0001 |
*** |
|
Physical Aggression vs. PMH |
Male |
0.039 |
-0.098 to 0.176 |
0.5618 |
ns |
|
Physical Aggression vs. PMH |
Female |
0.055 |
-0.092 to 0.199 |
0.4506 |
ns |
|
Anger vs. PMH |
Male |
0.273 |
0.140 to 0.396 |
0.0001 |
*** |
|
Anger vs. PMH |
Female |
0.222 |
0.078 to 0.357 |
0.0020 |
** |
|
Verbal Aggression vs. PMH |
Male |
0.021 |
-0.116 to 0.158 |
0.7535 |
ns |
|
Verbal Aggression vs. PMH |
Female |
-0.012 |
-0.159 to 0.133 |
0.8589 |
ns |
|
Hostility vs. PMH |
Male |
0.173 |
0.036 to 0.303 |
0.0110 |
* |
|
Hostility vs. PMH |
Female |
0.190 |
0.044 to 0.327 |
0.0086 |
** |
|
Note. PMH: Positive Mental Health; CL: Confidence Limit; ns: not significant * Statistically significant ** Very statistically significant *** Highly statistically significant r-value: Two variables correlation |
|||||
|
Relationship |
Residence |
r value |
CL-95% |
p-value |
Significance |
|
Altruism vs. PMH |
Rural |
0.353 |
0.221 to 0.472 |
0.0001 |
*** |
|
Altruism vs. PMH |
Urban |
0.406 |
0.282 to 0.518 |
0.0001 |
*** |
|
Public vs. PMH |
Rural |
0.413 |
0.287 to 0.524 |
0.0001 |
*** |
|
Public vs. PMH |
Urban |
0.172 |
0.031 to 0.305 |
0.0135 |
* |
|
Dire vs. PMH |
Rural |
0.207 |
0.066 to 0.340 |
0.0032 |
** |
|
Dire vs. PMH |
Urban |
0.226 |
0.088 to 0.356 |
0.0011 |
** |
|
Anonymous vs. PMH |
Rural |
0.474 |
0.356 to 0.578 |
0.0001 |
*** |
|
Anonymous vs. PMH |
Urban |
0.183 |
0.043 to 0.316 |
0.0084 |
** |
|
Compliant vs. PMH |
Rural |
0.374 |
0.244 to 0.490 |
0.0001 |
*** |
|
Compliant vs. PMH |
Urban |
0.361 |
0.232 to 0.478 |
0.0001 |
*** |
|
Emotional vs. PMH |
Rural |
0.108 |
-0.034 to 0.247 |
0.1265 |
ns |
|
Emotional vs. PMH |
Urban |
0.310 |
0.177 to 0.432 |
0.0001 |
*** |
|
Physical Aggression vs. PMH |
Rural |
0.292 |
0.156 to 0.417 |
0.0001 |
*** |
|
Physical Aggression vs. PMH |
Urban |
0.088 |
-0.052 to 0.227 |
0.2051 |
ns |
|
Anger vs. PMH |
Rural |
0.002 |
-0.140 to 0.145 |
0.9752 |
ns |
|
Anger vs. PMH |
Urban |
0.097 |
-0.043 to 0.235 |
0.1636 |
ns |
|
Verbal Aggression vs. PMH |
Rural |
0.231 |
0.092 to 0.362 |
0.0010 |
*** |
|
Verbal Aggression vs. PMH |
Urban |
0.095 |
-0.046 to 0.233 |
0.1727 |
ns |
|
Hostility vs. PMH |
Rural |
0.353 |
0.221 to 0.472 |
0.0001 |
*** |
|
Hostility vs. PMH |
Urban |
0.127 |
-0.013 to 0.264 |
0.0679 |
ns |
|
Note. PMH: Positive Mental Health; CL: Confidence Limit; ns: not significant * Statistically significant ** Very statistically significant *** Highly statistically significant r-value: Two variables correlation |
|||||
|
Relationship |
Age |
r value |
CL-95% |
p-value |
Significance |
|
Altruism vs. PMH |
Group 1 |
0.315 |
0.184 to 0.435 |
0.0001 |
*** |
|
Altruism vs. PMH |
Group 2 |
0.426 |
0.269 to 0.561 |
0.0001 |
*** |
|
Altruism vs. PMH |
Group 3 |
0.365 |
0.126 to 0.564 |
0.0027 |
** |
|
Public vs. PMH |
Group 1 |
0.286 |
0.153 to 0.409 |
0.0001 |
*** |
|
Public vs. PMH |
Group 2 |
0.280 |
0.107 to 0.436 |
0.0013 |
** |
|
Public vs. PMH |
Group 3 |
0.350 |
0.109 to 0.552 |
0.0042 |
** |
|
Dire vs. PMH |
Group 1 |
0.199 |
0.061 to 0.329 |
0.0037 |
** |
|
Dire vs. PMH |
Group 2 |
0.262 |
0.089 to 0.421 |
0.0026 |
** |
|
Dire vs. PMH |
Group 3 |
0.388 |
0.152 to 0.582 |
0.0014 |
** |
|
Anonymous vs. PMH |
Group 1 |
0.347 |
0.219 to 0.464 |
0.0001 |
*** |
|
Anonymous vs. PMH |
Group 2 |
0.289 |
0.117 to 0.444 |
0.0009 |
*** |
|
Anonymous vs. PMH |
Group 3 |
0.424 |
0.194 to 0.610 |
0.0004 |
*** |
|
Compliant vs. PMH |
Group 1 |
0.263 |
0.129 to 0.388 |
0.0001 |
*** |
|
Compliant vs. PMH |
Group 2 |
0.375 |
0.212 to 0.519 |
0.0001 |
*** |
|
Compliant vs. PMH |
Group 3 |
0.583 |
0.390 to 0.727 |
0.0001 |
*** |
|
Emotional vs. PMH |
Group 1 |
0.314 |
0.183 to 0.434 |
0.0001 |
*** |
|
Emotional vs. PMH |
Group 2 |
0.259 |
0.085 to 0.418 |
0.0030 |
** |
|
Emotional vs. PMH |
Group 3 |
0.464 |
0.241 to 0.640 |
0.0001 |
*** |
|
Physical Aggression vs. PMH |
Group 1 |
0.008 |
-0.130 to 0.147 |
0.9023 |
ns |
|
Physical Aggression vs. PMH |
Group 2 |
0.143 |
-0.035 to 0.313 |
0.1051 |
ns |
|
Physical Aggression vs. PMH |
Group 3 |
0.085 |
-0.169 to 0.329 |
0.4988 |
ns |
|
Anger vs. PMH |
Group 1 |
0.254 |
0.119 to 0.379 |
0.0002 |
*** |
|
Anger vs. PMH |
Group 2 |
0.286 |
0.114 to 0.441 |
0.0010 |
*** |
|
Anger vs. PMH |
Group 3 |
0.202 |
-0.051 to 0.431 |
0.1066 |
ns |
|
Verbal Aggression vs. PMH |
Group 1 |
-0.018 |
-0.156 to 0.121 |
0.7935 |
ns |
|
Verbal Aggression vs. PMH |
Group 2 |
0.022 |
-0.156 to 0.199 |
0.8019 |
ns |
|
Verbal Aggression vs. PMH |
Group 3 |
0.170 |
-0.084 to 0.403 |
0.1758 |
ns |
|
Hostility vs. PMH |
Group 1 |
0.242 |
0.108 to 0.368 |
0.0004 |
*** |
|
Hostility vs. PMH |
Group 2 |
0.158 |
-0.019 to 0.327 |
0.0721 |
ns |
|
Hostility vs. PMH |
Group 3 |
0.209 |
-0.043 to 0.437 |
0.0945 |
ns |
|
Note. PMH: Positive Mental Health; CL: Confidence Limit; ns: not significant; Age Group 1: 30–45; Age Group 2: 46–60; Age Group 3: 61–75 * Statistically significant ** Very statistically significant *** Highly statistically significant r-value: Two variables correlation |
|||||
Discussion
This research conducts a thorough exploration of the intricate relationships among gender, residency, and age, revealing how prosocial behavior and aggression collectively influence positive mental health. The disparities between verbal aggression and hostility, discerned through gender-based descriptive features. Table 1 establish a foundational understanding of the distinct behavioral patterns exhibited by different genders, where men showed higher verbal aggression and hostility than women. The finding that men exhibit higher levels of verbal aggression and hostility compared to women may be attributed to a combination of biological, social, and cultural factors also support existing literature [70]. From a biological standpoint, some research suggests that hormonal differences, particularly higher levels of testosterone in men, may contribute to increased aggression.
However, it is essential to acknowledge that the role of biology is complex and interacts with various environmental influences. Socially, traditional gender norms and expectations may shape behavior, with societal perceptions often associating assertiveness and dominance with masculinity. Additionally, cultural factors, such as the normalization of certain communication styles, can play a role in shaping how individuals express themselves verbally. It is crucial to interpret these findings with caution, recognizing the diversity within each gender and the potential influence of contextual factors. Further research and a nuanced understanding of the complexities surrounding gender differences in communication are necessary to draw more comprehensive conclusions. Boys are much more prone than girls to engage in aggressive behavior [59,60]. Another investigation indicated that the quantity of explicit verbal aggression used by both genders is identical [71]. As opposed to the slight strength of the gender differences for anger and hostility, men appeared to score higher on items associated with verbal and physical aggression [62]. Other research showed that, compared to boys, girls displayed significantly greater hostility [60,63].
In this Bangladeshi social and environmental context, it might offer an explanation for this discovery. Bangladesh has been reported to be an economically developing country. Similarly, to the way boys do it, girls are now actively participating in improving and developing their careers through higher education. Girls are consequently starting to develop a sense of self-respect and autonomy. When competing against their opponent, the girls face multiple challenges. Therefore, it is feasible that the females use aggression as a form of protest behavior against inequity and sloppy treatment. Prosocial behavior was substantially predicted by gender, with women demonstrating more prosocial behavior compared to males [24]. Another conclusion reinforced conclusions from previous studies investigating prosocial behavior in practice, which revealed that men are more likely to help others when there is a crowd present [72]. There are no significant gender variations in prosocial behaviors, as reported by Gregori et al., (2025) [18]. Adolescent boys expressed having a greater tendency than did adolescent girls to engage in gatherings of prosocial behavior, as opposed to these gender disparities [17,18]. Adolescent girls were able to report more submissive and prosocial behaviors than did adolescent boys [17,18]. This ought to come as no surprise considering that men and women have had different social roles for a great deal of the history of humanity and that different behaviors are anticipated of them based on their social context in nearly every society on the planet [73].When there is a context that subjects can associate with the appropriate social setting, we are likely to identify comparable variations in the laboratory if men and women follow specific standards for behavior in different social contexts [74]. Another study discovered that patients with schizophrenia-related illnesses varied by gender in their PMH total and domain scores, with women performing higher than males [75]. However, as we apply the PMH scale to people who are healthy and there are no further investigations on PMH, our research is not directly relevant to the previous findings. Initially, the majority of research has been on young people; this study is the first one of its organizations that aim at adults.
The residency-based descriptive characteristics (Table 2) shed light on positive differences within diverse groups, encompassing dire, anonymous, compliant, emotional, physical, verbal, and positive mental health categories. This thorough exploration provides a nuanced perspective on how varied residential environments can influence and mould expressions of aggression, prosocial behavior, and PMH. This study stands as a trailblazing investigation, being the first to delve into the relationships between prosocial behavior, aggression, and positive mental health based on residence, thereby filling a notable gap in prior research. This is the first finding that provides insight into potential future directions, as no prior results have been found in relation to residence for prosocial behavior. According to research by Rhoads et al., (2021), there is no statistically significant difference in respondent's levels of hostility between those who reside in rural as well as urban areas [76]. This study is the initial attempt to look into the connection between residential settings and positive mental health; no other research has been done in this specific field previously. The investigation, which is the first of its sort, provides a framework to conduct additional research and provides guidance for future studies with the goal of understanding the relationship between mental health and residence.
Considering age-based descriptive characteristics (Table 3), this investigation finds significant variations, especially in the anonymous and positive mental health categories. The findings emphasize the importance of age as a crucial factor regulating the dynamics of prosocial and aggressive behavior. Despite previous studies that mostly relied on single-scale categories, this study constitutes a breakthrough effort as the first to fully investigate the combined impact of prosocial behavior, aggressiveness, and positive mental health across age groups. Our approach is unique, and we ensure that the findings we obtain are unique and relevant in relation to previous research. The greatest amounts of prosocial behavior were demonstrated by older participants, intermediate levels by middle-aged participants, and the lowest levels by young participants [77,78]. Another study discovered that as individuals aged, their prosocial behavior increased [79]. Investigators observed that the stability of aggression decreases as measurement times remain longer [80,81] and improves with increasing age [60]. A further investigation concluded that both men and women's aggressive behavior stayed stable from childhood to middle life [82]. There have not been any previous investigations into the connection between age and positive mental health (PMH). This study is the first of its kind in this field, establishing a foundation for future investigators to look into previously unexplored aspects and advance our knowledge of the relationship between positive mental health and age.
With the exception of verbal and physical aggression, the analysis that follows in Table 4 shows a general connection between prosocial behavior, aggressiveness, and positive mental health. The extremely important results for each of the elements indicate an intricate connection, demonstrating how complex these relationships are. Evaluating the gender-based correlation in Table 5 in more detail reveals significant disparities across variables, indicating the complex influence of gender on the relationship between prosocial behavior, aggressiveness, and positive mental health.
In a comparable way, the residence-based relationship (Table 6) and age-based relationship (Table 7) highlight the complex nature of these relationships in particular contexts and provide significant insights into the manner in which environmental and developmental factors influence psychological health in general. This comprehensive study not only improves our understanding of the connections between these factors, but it also provides possibilities for specific interventions and focused approaches that promote positive mental health in a broad range of demographic circumstances.
Conclusion
This study aimed to examine the relationships between aggressive behavior, prosocial behavior, and mental health. The findings supported the hypothesis: prosocial behavior was positively correlated with mental health, while aggression showed a negative association. These results confirm that behavioral tendencies significantly influence psychological well-being. However, variations across gender, age, and geographic location suggest that these relationships are not uniform and may limit the generalizability of the findings. The findings provide administrators and policymakers with helpful recommendations that will impact the development of welcoming educational settings and comprehensive laws intended for improving community mental health Future studies should explore these variables further to enhance contextual understanding.
Ethical Approval
The ethical approval was obtained from the Ethical Review Committee-Research and Publication (ERCRP), Department of Psychology, University of Rajshahi, Rajshahi-6205, Bangladesh [approval code: ERCRP-PSYRU-7(12)24; Date: October 17, 2024]. The researchers completely declare that all methods carried out in studies involving human participants were in accordance with institutional and national ethical guidelines as well as the Helsinki Declaration (1979). The researchers have an intense commitment to research ethics.
Informed Consent Statement
Informed consent was obtained from all participants prior to their inclusion in the study. Participants were informed of their rights to confidentiality, voluntary participation, and the ability to withdraw from the study at any time without any consequences.
Data Availability Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Conflict of Interest statement
The authors declare that they have no conflicting interests.
Funding
There was no grant, technical or corporate support for this study.
Acknowledgments
The authors thank all study participants and special thanks go to the data collectors who were involved in this study.
Author Contributions
Conceptualization: Md. Muzahid Islam; Methodology: Md. Muzahid Islam, Afshana Mimi, Masom Mia; Formal analysis and investigation: Md. Muzahid Islam, Afshana Mimi, Murshida Khatun, Masom Mia, Palash Kumar Sarker; Writing - original draft preparation: Md. Muzahid Islam, Afshana Mimi, Masom Mia, Pramath Chandra Sarker, Palash Kumar Sarker; Writing - review and editing: Md. Muzahid Islam, Masom Mia, Pramath Chandra Sarker, Murshida Khatun, Palash Kumar Sarker.
References
2. Singh P. Prosocial Behavior-A Brief Overview. J Edu Psyc Res.2022;4(1):320–2.
3. Wea D, Hamu FJ. Happiness: Exploring Relationship with Empathic Sense, Altruistic Behaviour, Social Responsibility, and Interpersonal Relationship. MIMBAR PGSD Undiksha. 2023 Dec 4;11(3):375–83.
4. Mallott MA, Stryker JST, Schmidt NB. Paranoia and Social Anxiety: Predicting Aggressive Behavior. Behav Ther. 2024 Jul;55(4):825–38.
5. Mehulić J. Međudjelovanje individualnih obilježja partnera i interakcije u dijadi na percepciju svakodnevnoga stresa i održavanje kvalitetnih partnerskih odnosa. Doctoral dissertation, University of Zagreb, Faculty of Humanities and Social Sciences, Department of Psychology, 2024.
6. Mellor DJ, Beausoleil NJ. Extending the ‘Five Domains’ model for animal welfare assessment to incorporate positive welfare states. Animal Welfare. 2015 Aug;24(3):241–53.
7. Graf CS. Cross-Cultural Insights on the Role of Psychological and Institutional Factors for Real-World Prosocial Behavior and Cultural Change. Doctoral dissertation, Vrije Universiteit Amsterdam, 2024
8. Martí-Vilar M, Corell-García L, Merino-Soto C. Systematic review of prosocial behavior measures. Revista de psicología (PUCP). 2019;37(1):349–77.
9. Crone EA, Achterberg M. Prosocial development in adolescence. Current Opinion in Psychology. 2022 Apr;44:220–5.
10. Thielmann I, Spadaro G, Balliet D. Personality and prosocial behavior: A theoretical framework and meta-analysis. Psychological Bulletin. 2020 Jan;146(1):30–90.
11. Rodrigues J, Hewig J. Let´ s call it altruism! A psychological perspective and hierarchical framework of altruism and prosocial behavior. Journal of the Academy of Marketing Science. 2021 Mar 15;22(1).
12. Chávez DV, Salmivalli C, Garandeau CF, Berger C, Kanacri BPL. Bidirectional Associations of Prosocial Behavior with Peer Acceptance and Rejection in Adolescence. Journal of Youth and Adolescence. 2022 Dec;51(12):2355–67.
13. Pfattheicher S, Nielsen YA, Thielmann I. Prosocial behavior and altruism: A review of concepts and definitions. Current opinion in psychology. 2022 Apr;44:124–9.
14. Cimagalli F. Is there a place for altruism in sociological thought?. Human Arenas. 2020 Mar;3(1):52–66.
15. Radovanović B. Altruism in behavioral, motivational and evolutionary sense. Filozofija i društvo. 2019;30(1):122–34.
16. Paiva A, Correia F, Oliveira R, Santos F, Arriaga P. Empathy and prosociality in social agents. InThe handbook on socially interactive agents: 20 Years of research on embodied conversational agents, intelligent virtual agents, and social robotics volume 1: methods, behavior, cognition 2021 Sep 10:385–432.
17. Xiao SX, Hashi EC, Korous KM, Eisenberg N. Gender differences across multiple types of prosocial behavior in adolescence: A meta-analysis of the prosocial tendency measure-revised (PTM-R). Journal of Adolescence. 2019 Dec;77:41–58.
18. Gregori F, López-Pérez B, Manfredi L, Eisenberg N, Lundie D, Lee S, et al. The relations among prosocial behavior, hedonic, and eudaimonic well-being in everyday life. Journal of Personality. 2025 Apr;93(2):412–24.
19. Hui BPH, Ng JCK, Berzaghi E, Cunningham-Amos LA, Kogan A. Rewards of kindness? A meta-analysis of the link between prosociality and well-being. Psychological Bulletin. 2020 Dec;146(12):1084–116.
20. Gherghel C, Nastas D, Hashimoto T, Takai J. The relationship between frequency of performing acts of kindness and subjective well-being: A mediation model in three cultures. Current Psychology. 2021 Sep;40(9):4446–59.
21. Krol SA, Bartz JA. The self and empathy: Lacking a clear and stable sense of self undermines empathy and helping behavior. Emotion. 2022 Oct;22(7):1554–71.
22. Arman M. Empathy, sympathy, and altruism-An evident triad based on compassion. A theoretical model for caring. Scandinavian Journal of Caring Sciences. 2023 Sep;37(3):862–71.
23. Rossi G, Dingemanse M, Floyd S, Baranova J, Blythe J, Kendrick KH, et al. Shared cross-cultural principles underlie human prosocial behavior at the smallest scale. Scientific Reports. 2023 Apr 19;13(1):6057.
24. Pastor Y, Pérez-Torres V, Thomas-Currás H, Lobato-Rincón LL, López-Sáez MÁ, García A. A study of the influence of altruism, social responsibility, reciprocity, and the subjective norm on online prosocial behavior in adolescence. Computers in Human Behavior. 2024 May 1;154:108156.
25. Fedorko V. Determination of Prosocial Behavior of Preschool-Aged Children in the Context of Preschool Education. Palacký University Olomouc, 2021.
26. Trentini C, Tambelli R, Maiorani S, Lauriola M. Gender Differences in Empathy During Adolescence: Does Emotional Self-Awareness Matter? Psychological Reports. 2022 Apr;125(2):913–36.
27. Jin SV, Ryu E. "The greedy I that gives"-The paradox of egocentrism and altruism: Terror management and system justification perspectives on the interrelationship between mortality salience and charitable donations amid the COVID-19 pandemic. Journal of Consumer Affairs .2022 Spring;56(1):414–48.
28. Chung YW, Im S, Kim JE. Can Empathy Help Individuals and Society? Through the Lens of Volunteering and Mental Health.In Healthcare (Basel). 2021 Oct 20;9(11):1406.
29. Bakhti R. Testing the Impact of Interpersonal Regulatory Fit on Empathy, Willingness to Help, and Prosocial Behaviour. Doctoral dissertation, University of Roehampton, 2022.
30. Giardini F, Vilone D, Sánchez A, Antonioni A. Gossip and competitive altruism support cooperation in a Public Good game. Philosophical Transactions of the Royal Society B. 2021 Nov 22;376(1838):20200303.
31. Sturmey P. Violence and Aggression: Integrating theory, research, and practice. Cham: Springer Nature. 2022.
32. Alam QA. Frustration-aggression: revisited. International journal of scientific research in modern science and technology. 2023 Dec 30;2(12):48–53.
33. Berkowitz L. Towards a general theory of anger and emotional aggression: Implications of the cognitive—neoassociationistic perspective for the analysis of anger and other emotions. In: Wyer Jr. RS, Srull TK, Editors. Perspectives on anger and emotion. UK: Psychology Press; 2014 Jan 14. pp. 1–46.
34. Jahoda M. Current concepts of positive mental health. New York: Basic Books; 1958.
35. World Health Organization. WHO guideline on self-care interventions for health and well-being, 2022 revision. World Health Organization; 2022.
36. Sapranaviciute-Zabazlajeva L, Sileikiene L, Luksiene D, Tamosiunas A, Radisauskas R, Milvidaite I, et al. Lifestyle factors and psychological well-being: 10-year follow-up study in Lithuanian urban population. BMC Public Health. 2022 May 19;22(1):1011.
37. Bartolo MG, Palermiti AL, Servidio R, Costabile A. “I feel good, I am a part of the community”: Social responsibility values and prosocial behaviors during adolescence, and their effects on well-being. Sustainability. 2023 Nov 22;15(23):16207.
38. Patnaik G. Positive psychology for improving mental health & well-being. Chennai: Notion Press; 2021.
39. Hossen MS, Salleh SF. Social influences on the psychological well-being of elderly individuals. Journal of Humanities and Applied Social Sciences. 2025 Aug 15;7(4):315–32.
40. Nicolini P, Abbate C, Inglese S, Rossi PD, Mari D, Cesari M. Different dimensions of social support differentially predict psychological well-being in late life: opposite effects of perceived emotional support and marital status on symptoms of anxiety and of depression in older outpatients in Italy. Psychogeriatrics. 2021 Jan;21(1):42–53.
41. Tekin S, Sager M, Bushey A, Deng Y, Uluğ ÖM. How do people support each other in emergencies? A qualitative exploration of altruistic and prosocial behaviours during the COVID-19 pandemic. Analyses of Social Issues and Public Policy. 2021 Dec;21(1):1113–40.
42. Kamas L, Preston A. Empathy, gender, and prosocial behavior. Journal of behavioral and experimental economics. 2021 Jun 1;92:101654.
43. Singh S, Teoh VY. Enhancing pro-social behavior among college students: Exploring the role of abstract mindset. GSTF Journal of Law and Social Sciences (JLSS). 2014 Apr 1;3(2):28.
44. Feng Y, Zong M, Yang Z, Gu W, Dong D, Qiao Z. When altruists cannot help: the influence of altruism on the mental health of university students during the COVID-19 pandemic. Global Health. 2020 Jul 10;16(1):61.
45. Sparrow EP, Swirsky LT, Kudus F, Spaniol J. Aging and altruism: A meta-analysis. Psychology and Aging. 2021 Feb;36(1):49–56.
46. Fullen MC, Dolbin‐MacNab ML, Wiley JD, Brossoie N, Lawson G. The impact of excluded providers on Medicare beneficiaries’ mental health care. Journal of Counseling & Development. 2022 Apr;100(2):123–33.
47. Hirani S, Ojukwu E, Bandara NA. Understanding the role of prosocial behavior in youth mental health: findings from a scoping review. Adolescents. 2022 Aug 9;2(3):358–80.
48. Aknin LB, Broesch T, Hamlin JK, Van de Vondervoort JW. Prosocial behavior leads to happiness in a small-scale rural society. Journal of Experimental Psychology: General. 2015 Aug;144(4):788–95.
49. Levine GN, Cohen BE, Commodore-Mensah Y, Fleury J, Huffman JC, Khalid U, et al. Psychological Health, Well-Being, and the Mind-Heart-Body Connection: A Scientific Statement From the American Heart Association. Circulation. 2021 Mar 9;143(10):e763–83.
50. Costello H, Walsh S, Cooper C, Livingston G. A systematic review and meta-analysis of the prevalence and associations of stress and burnout among staff in long-term care facilities for people with dementia. International Psychogeriatrics. 2019 Aug;31(8):1203–16.
51. Duplantier SC, Williamson FA. Barriers and Facilitators of Health and Well-Being in Informal Caregivers of Dementia Patients: A Qualitative Study. International Journal of Environmental Research and Public Health. 2023 Feb 28;20(5):4328.
52. Marks DF, Murray M, Locke A, Annunziato RA, Estacio EV. Health psychology: Theory, research and practice. UK: SAGE Publications; 2024.
53. Kaufman SB, Jauk E. Healthy Selfishness and Pathological Altruism: Measuring Two Paradoxical Forms of Selfishness. Frontiers in Psychology. 2020 May 21;11:1006.
54. Juliá-Sanchis R, Sanjuan-Quiles Á, Richart-Martínez M, Cabrero-García J. The impact of volunteering in mental health settings on nursing students' attitudes. Nurse Education in Practice. 2020 Mar;44:102726.
55. Ling WH, Lee WP, Chui WH, Sin KM. Older adults and volunteering: Mental wellness, motivation, and satisfaction. Activities, Adaptation & Aging. 2023 Oct 2;47(4):482–500.
56. Siekierska B, Tomaszek L, Kurleto P, Turkanik E, Mędrzycka-Dąbrowska W. Blood donation practice and its associated factors among Polish population: secondary data analysis. Frontiers in Public Health. 2023 Oct 19;11:1251828.
57. Plant M, McGuire J, Dupret S, Dwyer R, Stewart B. Giving to others: how to convert your money into greater happiness for others. World Happiness Report. 2025
58. Chan AS, Chan SW, Yan E. Healthy aging, mental health, and sexuality. Frontiers in Urology. 2023 Sep 26;3:1287189.
59. Rahman MS, Nahar L. Aggression in boys and girls as related to their academic achievement and residential background. Psychology. 2013 May 16;4(5):459–62.
60. Hay DF, Paine AL, Perra O, Cook KV, Hashmi S, Robinson C, et al. Prosocial and Aggressive Behavior: A Longitudinal Study. Monographs of the Society for Research in Child Development. 2021 Jun;86(2):7–103.
61. Webster GD, Dewall CN, Pond RS Jr, Deckman T, Jonason PK, Le BM, et al. The brief aggression questionnaire: psychometric and behavioral evidence for an efficient measure of trait aggression. Aggressive Behavior. 2014 Mar-Apr;40(2):120–39.
62. Fahlgren MK, Cheung JC, Ciesinski NK, McCloskey MS, Coccaro EF. Gender Differences in the Relationship between Anger and Aggressive Behavior. Journal of Interpersonal Violence. 2022 Jul;37(13-14):NP12661–70.
63. Rahman AK, Huq MM. Aggression in adolescent boys and girls as related to socio-economic status and residential background. Journal of Life Earth Science. 2005 Jul;1(1):5–9.
64. Carlo G, Randall BA. The development of a measure of prosocial behaviors for late adolescents. Journal of Youth and Adolescence. 2002 Feb;31(1):31–44.
65. Costa M, Veríssimo L, Barbosa M, Ribeiro LM, Silva S, Carlo G. Prosocial tendencies measure validation for Portuguese late adolescents. Interação em Psicologia. 2022;26(1):83–91.
66. Buss AH, Perry M. The aggression questionnaire. Journal of Personality and social psychology. 1992 Sep;63(3):452–9.
67. Perven, A., Prosocialness on Aggression, Empathy and Psychological Well-Being Among Undergraduate Students. Unpublished Master’s Thesis, University of Rajshahi, 2022.
68. Hasan MT, Hasan MM, Perven A, Khan MHA. Validation and psychometric properties of the Bangla version of positive mental health scale (PMH-scale). Heliyon. 2023 Mar 25;9(4):e14663.
69. Khan AH, Sultana MS, Hossain S, Hasan MT, Ahmed HU, Sikder MT. The impact of COVID-19 pandemic on mental health & wellbeing among home-quarantined Bangladeshi students: A cross-sectional pilot study. Journal of Affective Disorders. 2020 Dec 1;277:121–8.
70. Padgett JK, Tremblay PF. Gender differences in aggression. The Wiley Encyclopedia of Personality and Individual Differences: Personality Processes and Individual Differences. 2020 Sep 18:173–7.
71. Amad S, Gray NS, Snowden RJ. Self-Esteem, Narcissism, and Aggression: Different Types of Self-Esteem Predict Different Types of Aggression. Journal of Interpersonal Violence. 2021 Dec;36(23-24):NP13296–313.
72. Carlo G, Padilla‐Walker L. Adolescents’ prosocial behaviors through a multidimensional and multicultural lens. Child Development Perspectives. 2020 Dec;14(4):265–72.
73. Zorotovich J, Dove M, Myers B. When traditional gender roles clash with contemporary expectations: A call to redefine success in the modern world. Journal of Family & Consumer Sciences. 2021 Apr 1;113(1):62–6.
74. Friebel G, Lalanne M, Richter B, Schwardmann P, Seabright P. Gender differences in social interactions. Journal of Economic Behavior & Organization. 2021 Jun 1;186:33–45.
75. Giordano GM, Bucci P, Mucci A, Pezzella P, Galderisi S. Gender Differences in Clinical and Psychosocial Features Among Persons With Schizophrenia: A Mini Review. Frontiers in Psychiatry. 2021 Dec 22;12:789179.
76. Rhoads SA, Gunter D, Ryan RM, Marsh AA. Global Variation in Subjective Well-Being Predicts Seven Forms of Altruism. Psychological Science. 2021 Aug;32(8):1247–61.
77. Sze JA, Gyurak A, Goodkind MS, Levenson RW. Greater emotional empathy and prosocial behavior in late life. Emotion. 2012 Oct;12(5):1129–40.
78. Tomar A. Prosocial Behavior And Wellbeing Among Middle-Aged Individuals. International Journal of Novel Research and Development. 2023 sept; 8(9), a791–805.
79. Cutler J, Nitschke JP, Lamm C, Lockwood PL. Older adults across the globe exhibit increased prosocial behavior but also greater in-group preferences. Nature Aging. 2021 Oct;1(10):880–8.
80. Drummond A, Sauer JD, Ferguson CJ. Do longitudinal studies support long-term relationships between aggressive game play and youth aggressive behaviour? A meta-analytic examination. Royal Society Open Science. 2020 Jul 22;7(7):200373.
81. Islam MM, Mimi A, Khatun M, Sarker PC, Islam T, Al Based MA. Sleeping Patterns and Online Gaming Habits: Unravelling Their Influence on Anger Tolerance Among University Students: Anger tolerance among university students. Psychiatry Nursing Journal (Jurnal Keperawatan Jiwa). 2025;7(1):1–6.
82. Loeber R, Capaldi DM, Costello E. Gender and the development of aggression, disruptive behavior, and delinquency from childhood to early adulthood. In: Leventhal BL, Tolan PH, Editors. Disruptive behavior disorders. New York, NY: Springer New York; 2013 Jun 13. pp. 137–60