Abstract
To perform elective surgery resulting in inconspicuous scarring, incisions must be placed along or parallel to tension lines or collagen fibers. Since both are invisible, we were able to show that both, tension lines and collagen fibers, run perpendicular to the striae distensae, which in humans always are formed in the same direction. We present unambiguous clinical examples and histological pictures which prove the direction and parallelization of collagen fibers and their supportive elastic fiber network. As less collagen fibers are destructed during surgery and severe stretching of the wound edges - less fibroblasts are needed for repair, resulting in an optimal scar.
Keywords
Surgical incisions, Folding lines, Skin tension lines, Striae distensae, Stretchmarks, Hypertrophic scar
The Direction of Surgical Incisions
In an early publication [1], we could show that striae distensae always develop perpendicular to the skin tension lines. In another article [2], we demonstrated that virtual skin tension lines are identical to the obvious Main Folding Lines; we recommended their use as optimal directions for orthopedic incisions, when inconspicuous scar formation is a prerequisite, as in children, younger adults, and women.
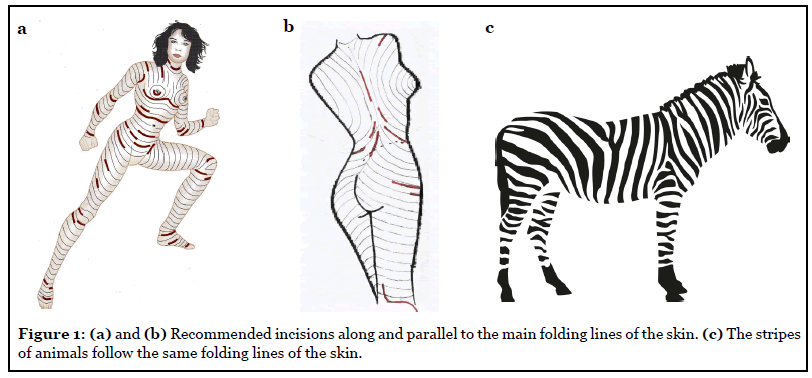
In this commentary, we discuss the histological findings of the skin structures and the correct skin incision for improved wound healing and optimal inconspicuous scarring. Most patients do not mind an obvious scar if the operation relieves a bony distortion, joint pain, or walking disability. Unfortunately, most orthopedic surgeons perform surgery according to the school manual [3,4]; with an emphasis on straight bones and movable joints, ignoring scars, which accompany patients for life. However, younger patients may be disappointed after finding wide scars across their shoulder, their hip, or in a vertical direction over their patella. These can easily be avoided if the incision is planned in the Main Folding Lines (Figures 1a and 1b).
The surrounding skin can be undermined in all parts of the human body, including the extremities, to get easy access to joints and bones. Skin incisions should always be as deep as needed in order to avoid disruption of collagen fibers in wound edges, which will stimulate fibroblasts and cause more scar production (Figures 2a and 2b). More examples and illustrations are provided in a small booklet on optimal surgical incisions [5].

Interestingly, the stripes of tigers and zebras follow similar lines, transverse at the torso and extremities, and concentric towards the inner side of the large joints. Since these animals do not have broad shoulders, they lack long stripes on their backs (Figure 1c); whereas in humans, the folding lines on the back run vertically and can be demonstrated when shoulders are moved backwards.
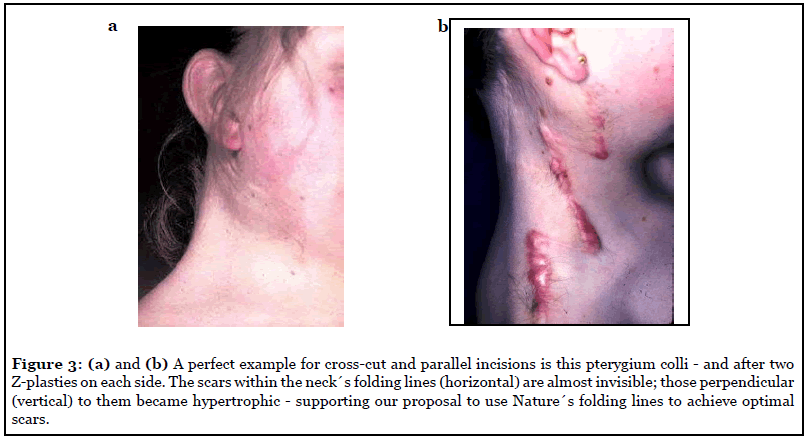
Plastic surgeons have long been aware of hypertrophic scar formations in adolescents and avoid elective surgeries at this age. However, the main cause of hypertrophy is an incision in the wrong direction, oblique or even perpendicular to the Main Folding Lines (Figures 3a and 3b). A minor cause may be wound healing disturbances or wound infections. Although facial and abdominal folds can be easily identified, folding lines may be difficult to determine on back, arms and legs, and may be absent in younger patients. However, performing the “pinch test” (Figure 4) in various directions or movement of joints on arm and foot can visualize the folding lines even in children.

Aesthetic surgeons learn to follow specific directions for incisions, reconstructive surgeons may be uncertain of the optimal direction, general surgeons focus on the fastest and most direct way to reach the abdominal cavity, and orthopedic surgeons focus on the most convenient way to access a bone or joint. Surgical and orthopedic textbooks don’t mention natural folding lines for optimal incision [6]. The concept of using natural striae distensae for optimal incision lines is new [1] and an extension to the earlier presentations of Kraissl [7] and Borges [8].
During the past century, thirty-eight various guidelines have been developed regarding elective incisions. Most surgical textbooks include Langer’s “cleavage lines” of 1861 [9], despite the fact that these incisions run oblique or even perpendicular to actual skin folds and vertically across the ante-cubital region, the wrist, thigh, and distal regions of the extremities, although concordant on neck, shoulders, back and buttocks. Therefore, new oblique, horizontal or partly circumferential directions for incisions on extremities are proposed.
Striae Distensae
Skin tension lines are a virtual imaginary concept of Borges [8]. In order to give this concept a tangible reality, we thought of natural facts like striae distensae, which are caused by hormonal changes in the skin, and obvious not only in pregnant women but also in adolescents. The elastic fibers which normally fix the collagen fibers as parallel bundles loosen and “stretchmarks” (Figure 5) occur perpendicular to the direction of the collagen bundles by pulling and tearing them apart. Since this disruption is a permanent fact until the end of life, all advertised and praised therapies against striae will be ineffective.
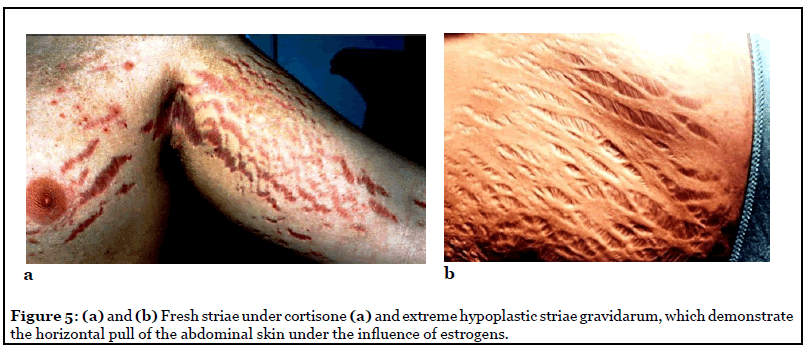
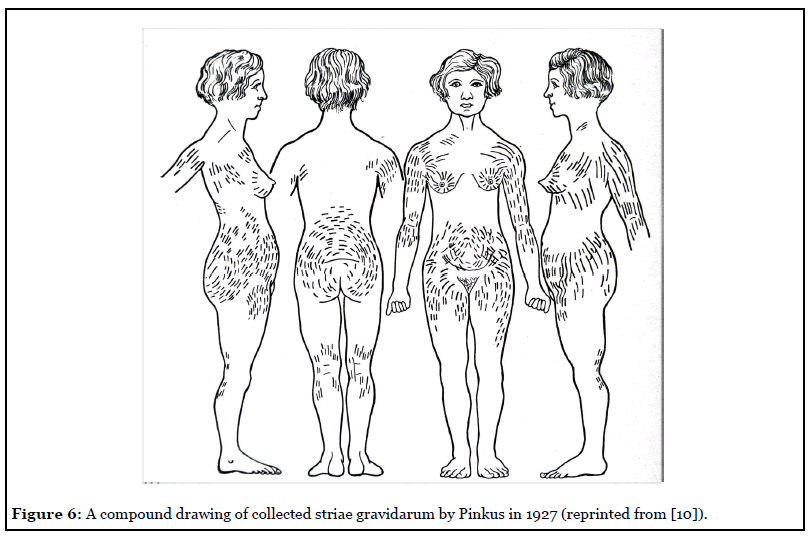
Striae distensae or striae gravidarum are seen in many male and female patients and can often act as a guide in planning elective incisions. Regardless of their etiology and slight variation, they have the same direction [10] (Figure 6) and clinical appearance, either fresh and read or mature and pale (Figure 5).
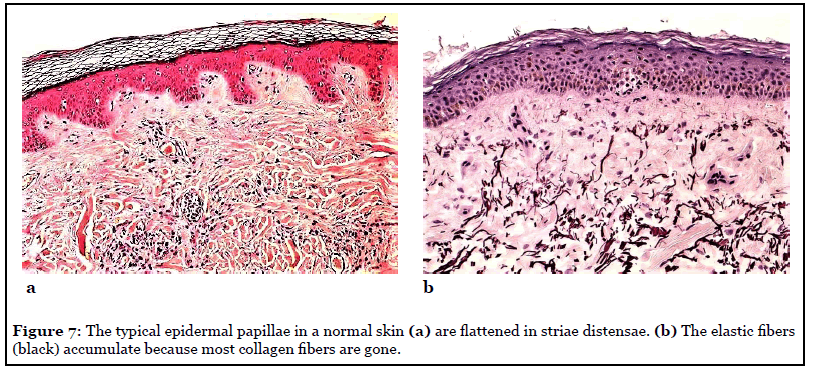
The fibroblasts in striae possess a contractile phenotype more akin to myofibroblasts [11] and the elastic fiber network proximal to the epidermal- dermal junction appears to be more prone to destruction in active striae. The collagen lattice can be ruptured under the influence of steroids and especially estrogens (Figures 7a and 7b) The newly synthesized collagen becomes reorganized by tension and is aligned in the direction of the presumed stress. The same happens in wound healing and therefore striae are considered dermal scars [12]. In general, people with a lack of elastic components in the extracellular matrix of their dermis are more prone to hypotrophic than hypertrophic scar formation.
During pregnancy, striae distensae appear in the abdominal skin often during the first months of pregnancy and before tension is caused by the growing fetus and uterus. Obesity, oral contraceptives, and breast augmentation can also cause striae in a small percentage of women. The widest and deep red striae are seen in Cushing patients and in those under chronic systemic or local cortisone therapy (Figure 5a) [14].
The claim that mechanical stretching is the main cause of striae is disputable: Striae often occur in early pregnancy when there is no obvious stretching of the skin by the growing uterus. They also appear over the hips of adolescents, when there is minimal stretching. If skin expansion is the only reason, the use of inflatable silicone expanders should be accompanied by a certain incidence of striae formation, but it is not. Also, if excessive skin stretching was a factor, athletes, gymnasts, and heavy lifting workers would be expected to develop more stretch marks than the average population. Yet the only athletes known to develop them are weightlifters and probably due to the use of anabolic steroids. In general, potential causes for striae development are family history, difficult hormonal equilibrium during adolescence, obesity, and the presence of varicosis.
Recent research on estrogen receptors in the extracellular matrix suggests the importance of estrogen in the development of striae [15]. When estrogen-, androgen-, and glucocorticoid receptors in the skin of patients with striae were compared to those in healthy skin, their number was actually double in the skin with striae [16]. These findings indicate that under certain conditions, there is an increase in hormonal receptor expression in the skin. Their activity may influence the metabolism of the extracellular matrix pointing to the important involvement of estrogens in striae formation.
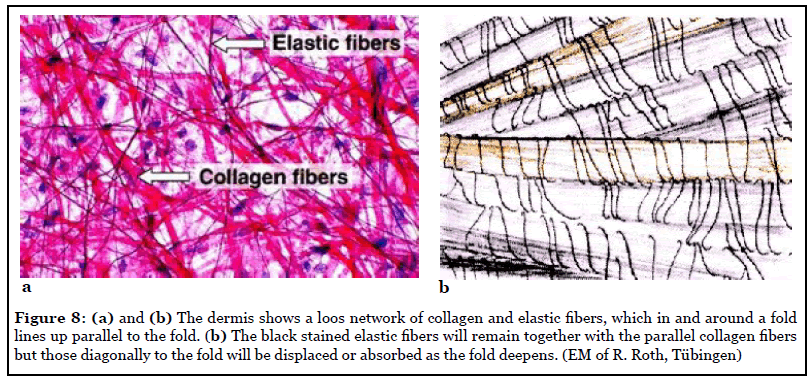
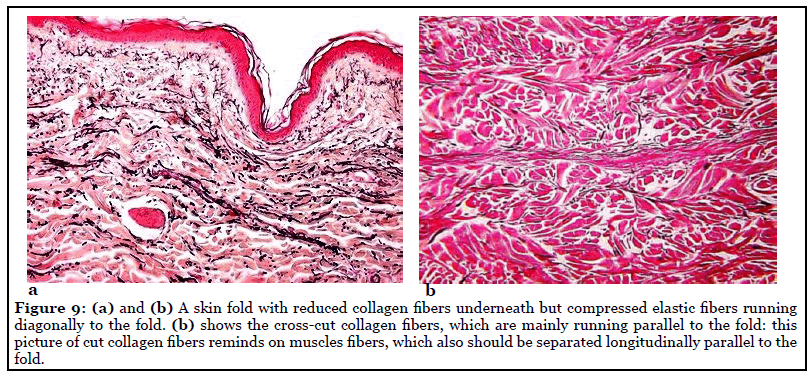
The presence of tension lines and normal wrinkle lines in the skin depends on the interrelation between elastic fibers and collagen fibers, as well as on the anchorage of collagen bundles one upon another (Figures 8a and 8b) [11]. During movement of the joints and in the normal process of aging, more and more visible and virtual folds will form in the direction of greatest tension (Figures 9a and b). At the same time, the fibroblast in the dermis produce collagen fibers, which run parallel with these tension lines or folds. When directed parallel to these collagen fibers, a scalpel will cut only the tiny elastic fibers but separate and not destroy the collagen fibers. When wound healing starts, the separated collagen fibers align to each other in a parallel direction like in a spread muscle. In a wound with little destruction, the fibroblasts must form much less scar tissue compared to the case of mass destruction of collagen fibers when they were cross-cut.
Conclusions
In many areas of the body surface, the described “main folding lines” run closely to the Langer lines, with which they are often confused. Langer lines were created by static forces in the skin of cadavers. The normal wrinkle lines are produced by dynamic forces acting on the skin of a living person.
While plastic surgeons have basically relied on these recommendations for the past 50 years, general and orthopedic surgeons still consider vertical incisions in the abdomen, over the hip joint, and across the anterior knee folds as the gold standard [3,6].
In normal wrinkle lines, the predominant orientation of collagen fibers is parallel to the wrinkles. Collagen bands in scars also form parallel to the wound edges, regardless of scar location. Striae distensae develop perpendicular to the direction of the strongest tension on the skin, and nature reveals that the tension or main folding lines are perpendicular to the striae.
Orthopedic surgeons, who have difficulty to identify skin folds or striae, may use the graphics above in Figures 1a and 1b as guidance. In elective surgery, most incisions or excisions can be planned in the direction of the main folding lines, even when the underlying structures such as ribs and bones suggest the opposite [17]. Even small incisions for minimal-invasive surgery should follow these folding lines to avoid the handwriting of the orthopedic surgeon on the body of his patients.
Authors Contribution Statement
The author was responsible for study concept and data acquisition, data interpretation, and manuscript drafting.
Conflict of Interest
There is no conflict of interest.
Funding Statement
The author got no financial support.
References
2. Lemperle G, Knapp D, Tenenhaus M. Minimal Scar Formation After Orthopaedic Skin Incisions Along Main Folding Lines. Journal of Bone and Joint Surgery. 2019 Mar 6;101(5):392-9.
3. Kocher T. Textbook of Operative Surgery (3rd English ed.). London: Adam and Charles Black 1911:p.30.
4. Patnaik VVG, Singla RK, Gupta PN. Surgical Incisions — Their Anatomical Basis. Part III - Lower Limb. Journal of The Anatomical Society of India. 2001;50: 48-58
5. Lemperle G, Knapp D. Minimal Scar Formation after Surgical Incisions in Main Folding Lines. Lambert Academic Publishing, Saarbrücken, Germany, 2017.
6. Azar FM, Canale ST, Beaty JH. Campbell’s Operative Orthopaedics, 14th Edition, Elsevier Mosby, Philadelphia 2020.
7. Kraissl CJ. The selection of appropriate lines for elective surgical incisions. Plastic and Reconstructive Surgery. 1951 Jul 1;8(1):1-28.
8. Borges AF. Relaxed skin tension lines (RSTL) versus other skin lines. Plastic and Reconstructive Surgery. 1984 Jan 1;73(1):144-50.
9. Langer K. On the anatomy and physiology of the skin: I. The cleavability of the cutis. British Journal of Plastic Surgery. 1978 Jan 1;31(1):3-8.
10. Pinkus F. Die normale anatomie der haut. InAnatomie der Haut 1927 (pp. 1-378). Springer, Berlin, Heidelberg. 1927:4-76.
11. Piérard GE, Lapière CM. Microanatomy of the dermis in relation to relaxed skin tension lines and Langer’s lines. The American journal of dermatopathology. 1987 Jun 1;9(3):219-24.
12. Arem AJ, Kischer CW. Analysis of striae. Plástic and Reconstructive Surgery. 1980 Jan;65(1):22-9.
13. Alshaiji JM, Handler MZ, Schwartzfarb E, Izakovic J, Schachner LA. Unilateral Striae Distensae Affecting the Right Axilla in a 16-Year-Old Boy: Brief Report. Pediatric Dermatology. 2014 Sep;31(5):617-8.
14. Rotsztejn H, Juchniewicz B, Nadolski M, Wendorff J, Kamer B. The unusually large striae distensae all over the body. Advances in Medical Sciences. 2010 Jan 1;55(2):343- 5.
15. Cordeiro RC, Zecchin KG, De Moraes AM. Expression of estrogen, androgen, and glucocorticoid receptors in recent striae distensae. International Journal of Dermatology. 2010 Jan;49(1):30-2.
16. Elsaie ML, Baumann LS, Elsaaiee LT. Striae distensae (stretch marks) and different modalities of therapy: an update. Dermatologic Surgery. 2009 Apr;35(4):563-73.
17. Leunig M, Hutmacher JE, Ricciardi BF, Impellizzeri FM, Rüdiger HA, Naal FD. Skin crease ‘bikini’incision for the direct anterior approach in total hip arthroplasty: a two-to four-year comparative study in 964 patients. The Bone & Joint Journal. 2018 Jul;100(7):853-61.