Abstract
Introduction: A Monteggia fracture is a fracture of the proximal ulna with radial head dislocation. The Bado classification is frequently used, though it does not cover all patterns. Type 1 is the most common, while Types 3 and 4 are rare. A rare complication is radial nerve palsy, particularly posterior interosseous nerve palsy, which usually manifests as neuropraxia and resolves spontaneously.
Case Presentation: We present a 11-year-old black, boy who we managed as a case of Bado type III Monteggia variant associated with ipsilateral fractures of humerus and ulnar shaft and radial nerve injury, an extremely rare combination of injuries in an 11-year-old boy who presented to the emergency department after a motor vehicle crush (MVC) as an unrestrained passenger. Plain radiographs demonstrated a right midshaft humerus fracture and a right segmental ulnar fracture (olecranon and distal third ulnar shaft) with a lateral radial head dislocation. Wound debridement, ORIF with ESIN for the humeral shaft fracture, lag screw fixation for olecranon fracture and Kirschner wire pinning for the distal third ulnar fracture. A split thickness skin graft for the degloved forearm was performed after 2 weeks. The patient was discharged home and followed up subsequently. The affected limb function was excellent (95) using the May Elbow Performance Score(MEPS) with no complications.
Conclusion: Accurate diagnosis and classification of forearm fractures are essential for effective treatment. This case report emphasizes the importance of advancing clinical comprehension of forearm fracture-dislocations to improve therapeutic outcomes and contribute to a broader knowledge base.
Keywords
Monteggia fracture-dislocation, Bado classification, Olecranon fracture, Neuropraxia
Introduction
Monteggia fractures, first described in 1814 by Giovanni Battista Monteggia, are classically defined by the combination of a radial head dislocation with an ulnar shaft fracture. Although the Bado classification, introduced in 1967, has long provided a framework for categorizing these injuries, many patterns do not conform to its strict criteria and are now identified as Monteggia variants or equivalents. Jose Luis Bado in his groundbreaking 1967 article first introduced the term “Monteggia equivalent lesion” [1]. Aside from defining the four classical types of Monteggia lesions, Bado also described a group of injuries that, while sharing a similar mechanism, manifested in varied ways compared to typical Monteggia lesions. He outlined five subgroups within the type I equivalents: (Ia) anterior dislocation of the radial head without a clear ulnar fracture, it also includes the pediatric ‘pulled elbow syndrome’; (Ib) a fracture of the ulnar diaphysis accompanied by a fracture of the radial neck; (Ic) an isolated fracture of the radial neck; (Id) a fracture of the ulnar diaphysis with a fracture of the proximal third of the radius; (Ie) a fracture of the ulnar diaphysis combined with an anterior dislocation of the radial head and a fracture of the olecranon. It is noticed that, type Ib–Id and type II equivalents do not specifically address the condition of the radio-capitellar joint unlike the traditional types I–IV, each of which involves a dislocated radial head. Bado did not describe any equivalents for types III and IV. Over the ensuing decades, case reports have greatly expanded the spectrum of lesions classified as “Monteggia equivalent,” thereby blurring the original definition [2,3]. This issue is further complicated in pediatric patients, where the immature radio-capitellar epiphysis and a more flexible joint predispose to subluxation, leading to frequent misdiagnoses or oversights. Overall, these fractures are rare, constituting less than 2% of all forearm fractures, with an even lower occurrence in adults. Robles et al. reported diagnostic challenges persist as radiologists overlook up to 25.5% of cases, while bedside clinicians including orthopedic surgeons fail to diagnose 14.9% of cases and 10.6% by both groups. The intricate anatomy and biomechanics of the forearm and elbow, combined with the varied presentations of Monteggia injuries, complicate accurate diagnosis. As a result, early clinical detection is vital, with key indicators such as localized pain, swelling, deformity, restricted movement, and neurovascular deficits especially posterior interosseous nerve (PIN) neuropathy. Timely diagnosis and surgical intervention are essential to prevent complications, ensuring better functional outcomes and reducing the risk of long-term disability [4].
In pediatric patients, about 70% are Bado Type I featuring a proximal or mid-ulnar fracture with anterior radial head dislocation, roughly 20% are Bado Type II, which involves posterior radial head dislocation. Bado Types III and IV are less common, with Type IV (1%) involving fractures of both the ulna and radius. Additionally, the Jupiter subclassification refines Type II injuries by detailing fracture patterns in relation to the coronoid process [5]. Complications include nonunion (occurring in 2–10% of cases), PIN neuropathy (affecting up to 10% of patients, typically resolving within 9–12 weeks), and persistent radial head dislocation particularly when reduction is delayed beyond two to three weeks due to fibrotic changes [6].
We herein present a Monteggia variant in an 11-year-old male, along with its treatment strategy and follow-up care, thereby contributing to the evolving discourse on the optimal management of these complex injuries.
Case Presentation
An 11-year-old black, male with no relevant past medical, social or surgical history who was an unrestrained passenger in a vehicle that rear ended a stationary vehicle. Client lost consciousness for an unknown period of time with a mechanism of injury from an axial loading from bracing during impact, Rotational forces due to limb position at collision, valgus stress at the elbow causing lateral radial head displacement and a High-energy bending forces fracturing the proximal ulna. He presented to Nkawie Toase Hospital where first aid was administered and subsequently referred to Komfo Anokye Teaching Hospital with the arm being supported in a sling in adduction for further management. There was no seizure, vomiting, bleeding from ENT orifices but headache. On examination, there were no immediate life-threatening injuries. There was no cervical spine, chest, or pelvic compression tenderness. GCS was 15/15. There was a degloving injury on the posterior aspect of the right forearm extending from the elbow joint to the wrist joint. A 1 cm ´ 1 cm wound on the anterolateral aspect of the proximal third of the right arm was also found. CRT was less than 3 seconds. He was able to do the ok sign, able to minimally flex digits but was unable to dorsiflex wrist joint and was unable to fully extend thumb. sensations in the distributions of the radial, ulnar and medial nerve were present. Radial artery pulsations were palpable. There were no signs or symptoms of compartment syndrome. X rays showed a fracture of the proximal ulnar with lateral dislocation of the radial head, a displaced transverse fracture of the middle third of the right humerus and a transverse fracture of the distal third of the right ulna (Figure 1). Broad spectrum antibiotics, adequate analgesics, tetanus prophylaxis were given and he was optimized for surgery.

Figure 1. Admission radiographs showing a right mid-shaft humeral fracture with segmental ulnar fractures (proximal/olecranon region and distal third ulnar shaft) with associated lateral radio-capitellar (radial head) dislocation (Monteggia variant). Clinical photograph shows a posterior forearm degloving injury extending from the elbow region toward the wrist. A small wound is seen over the anterolateral aspect of the proximal arm.
Surgical Technique
Under sterile conditions, general anesthesia with a supraclavicular block was induced, and the patient was positioned supine with routine cleaning and draping of the right upper limb. A 5-cm longitudinal incision was made over the olecranon and deepened, through which the fracture was reduced and provisionally stabilized with a Kirschner pin before definitive fixation with a 4.5 mm × 75 mm lag screw. The distal third ulnar fracture was reduced via the degloving wound and stabilized with pin fixation. After copious irrigation with normal saline, the olecranon incision was closed in layers using interrupted nylon 0 sutures. A separate 6-cm incision was then made over the lateral shoulder approximately 4-cm distal to the deltoid insertion, with dissection carried down to the humerus. An awl was employed to create a tract, allowing for the insertion of a 2 mm FTN, with a second 2 mm FTN placed approximately 2-cm medial to the initial one. The radial head reduction was achieved via a closed method following ulna alignment. Fluoroscopic imaging confirmed the correct positioning of all hardware. The degloved forearm was dressed and allowed to granulate, and two weeks later, it was successfully covered with a fenestrated split-thickness skin graft (Figure 2).
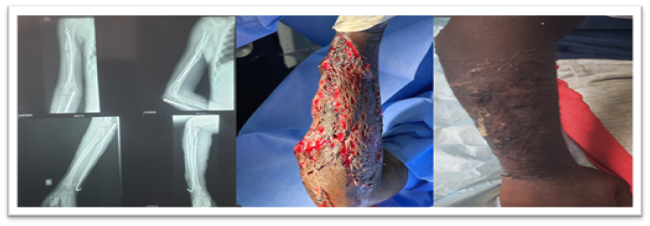
Figure 2. Post-operative radiographs show fixation and stabilization of the fractures with restored alignment. The degloved forearm wound is shown after debridement and dressing, allowed to granulate prior to definitive coverage. Follow-up photograph showing the post-coverage appearance.
At 6 weeks follow up visit the affected limb function was excellent, scoring 95 using the Mayo Elbow Performance Score (MEPS) with no complications (Figure 3).

Figure 3. Follow-up clinical photographs show functional finger extension with hand opening and a “thumbs-up” posture demonstrating satisfactory thumb extension and overall functional recovery on examination.
Discussion
The injury described herein deviates from the classic Monteggia fracture. Instead, this case involves a proximal olecranon fracture combined with lateral dislocation of the radio-capitellar joint and an ulna shaft fracture. According to the Bado classification, the presence of a segmental ulnar fracture also suggests features of a Type Ie injury however the lateral radial head dislocation component aligns the injury most closely with a Type III lesion [1]. This hybrid pattern underscores the complexity of the variant, highlighting its incompatibility with the established classification framework. Bado type III injuries are associated with a high risk of complications. Improper treatment or a delay in treatment of more than 3 weeks could lead to old unreduced Monteggia fracture.
As noted previously, not all Monteggia fractures conform to the traditional classification system. Artiaco et al. have proposed an alternative, more comprehensive framework for forearm and Monteggia variant fractures, founded on a "locker" concept that extrapolates from the functional and anatomical joints of the forearm described earlier [7]. This system delineates 13 distinct fracture patterns: the numeral "1" designates the proximal forearm joint (including the PRUJ), "2" represents the middle radioulnar joint—comprising the forearm bones and the interosseous membrane—and "3" corresponds to the distal radioulnar joint (DRUJ). Modifiers are appended with letters: "R" indicates a concomitant radial fracture, "I" denotes an interosseous membrane (IOM) rupture, and "U" signifies an associated ulnar fracture. Although this classification is more inclusive of Monteggia variants or equivalents, its use in clinical practice remains limited.
Lastly, it is imperative to emphasize the distinctiveness of the case presented herein. To our knowledge, a child with the specific injury pattern characterized by a lateral radial head dislocation with ipsilateral segmental ulnar shaft fracture (olecranon and distal third), humerus shaft fracture and radial nerve palsy has not been previously documented in the literature. This pattern was absent from the retrospective reviews discussed earlier and remains an outlier following an exhaustive examination of reported Monteggia variants. For instance, Chao Gao et al. described a variant corresponding to a classic Bado Type III with ipsilateral distal radius and ulna fractures [8]. Gupta et al. reported a 47-year-old with segmental comminuted fracture of ulna with anterior radial head dislocation [9]. Similarly, Fallah et al. detailed a Type IV lesion associated with a segmental fracture of the ulnar shaft, a proximal radial shaft fracture, and a comminuted radial head fracture [10]. Dattani et al. described a Monteggia fracture dislocation and an ipsilateral lateral humeral condyle fracture in a 3-year-old child [11]. Although Jain et al. reported a case of a 33-year-old male with a segmental ulna fracture and radial head dislocation, none of these cases precisely mirror the unique constellation of findings in our patient [12]. Consequently, this case represents a novel variant that expands the current understanding of Monteggia injury patterns and underscores the need for further refinement of classification systems to encompass such atypical presentations.
Conclusion
This case report describes a previously unrecognized variant of Monteggia fracture, highlighting a gap in the current literature and emphasizing the limitations of the conventional Bado classification in fully encompassing the spectrum of Monteggia fracture patterns. Although these variants are less common than classic Monteggia injuries, emerging evidence suggests they are associated with poorer clinical outcomes. The complexity of Monteggia fractures, coupled with their diverse and potentially severe complications, underscores the critical need for early recognition and precise anatomic reduction to optimize patient prognosis. By presenting this unique case, we aim to enhance clinical awareness of atypical Monteggia injuries and advocate for a reassessment and potential expansion of existing classification systems. A more comprehensive understanding of these variants will aid in accurate diagnosis, inform preoperative planning and decision-making, and ultimately support the restoration of anatomical alignment and functional recovery.
Patient Perspective
The patient and his guardian were very content and satisfied with the whole management and outcome of the condition.
Ethics Approval and Consent to Participate
Not applicable. Ethical approval is not required for single case reports at our institution.
Consent for Publication
Written informed consent was obtained from the patient's legal guardian for publication of this case report and any accompanying images. A copy of the written consent is available for review by the Editor-in-Chief of this journal.
Availability of Data and Materials
All data generated or analysed during this case report are included in this published article.
Authors' Contributions
All the authors managed the patient. Peter Agyekum Boateng drafted the manuscript, performed the literature review and critically revised the manuscript with Isaac Ahorklu. All authors read and approved the final manuscript.
Acknowledgements
The authors would like to acknowledge the Surgical team and Nursing staff of the Directorate of Trauma and Orthopedics, Komfo Anokye Teaching Hospital, Kumasi, Ghana, for their support in the management of the patient.
Declaration of Patient Consent
Informed consent was obtained from the patient's guardian for the publication of clinical data and images. All reasonable measures have been taken to ensure the patient’s anonymity, although absolute anonymity cannot be guaranteed.
Conflict of Interest
The authors declare that they have no competing interests.
Source of Funding
The authors received no financial support for the authorship or publication of this article.
References
2. Robles EL, Rolfs H, Hargett D. Monteggia variant with posterior elbow dislocation and radial shaft fracture: A case report. Int J Surg Case Rep. 2022 Oct;99:107705.
3. Xu L, Ye W, Li H, Xu J, Zhu W, Zhen Z, et al. Monteggia equivalent lesion in children: a narrative review. World J Pediatr Surg. 2021 Jul 7;4(3):e000283.
4. Zilliacus K, Nietosvaara Y, Helenius I, Kämppä N, Vuorimies I, Grahn P. Bado type III Monteggia fractures have a high injury- and treatment-related complication rate: a single center study of 73 fractures. Acta Orthop. 2024 Oct 14;95:600–6.
5. Degreef I, De Smet L. Missed radial head dislocations in children associated with ulnar deformation: treatment by open reduction and ulnar osteotomy. J Orthop Trauma. 2004 Jul;18(6):375–8.
6. Stitgen A, McCarthy JJ, Nemeth BA, Garrels K, Noonan KJ. Ulnar fracture with late radial head dislocation: delayed Monteggia fracture. Orthopedics. 2012 Mar 7;35(3):e434–7.
7. Artiaco S, Fusini F, Sard A, Dutto E, Massè A, Battiston B. Fracture-dislocations of the forearm joint: a systematic review of the literature and a comprehensive locker-based classification system. J Orthop Traumatol. 2020 Dec 2;21(1):21.
8. Gao C, Sun JH, Zheng HJ, Wu YY, Cao J. Type III Monteggia Injury With Ipsilateral Distal Forearm Fracture in a Child: A Case Report. Front Pediatr. 2022 Jan 31;9:805985.
9. Gupta L, Rathore LP. An atypical type of monteggia equivalent: A case report. Int J Orthop Sci. 2018; 4:1037–9.
10. Fallah Y, Baghianimoghadam B, Baghbani S, Karim A. Type IV Monteggia-equivalent fracture in an adult: a case report. Clin Shoulder Elb. 2023 Jun;26(2):205–7.
11. Dattani R, Patnaik S, Kantak A, Lal M. Distal humerus lateral condyle fracture and Monteggia lesion in a 3-year old child: a case report. Acta Orthop Belg. 2008 Aug;74(4):542–5.
12. Jain D, Singh S, Binyala S, Kumar P. An Atypical Type of Monteggia Equivalent: A Case Report. J Orthop Case Rep. 2021 Oct;11(10):96–9.