Abstract
Background: Spontaneous ovarian hyperstimulation syndrome (sOHSS) is a rare condition in naturally conceived pregnancies, characterized by ovarian enlargement and extravascular fluid accumulation.
Case presentation: A 19-year-old Ethiopian woman, gravida III para I, presented at 10 weeks gestation with progressive abdominal swelling, ascites, and hypoxia (SpO2 92%). She had no history of fertility treatment. Ultrasound showed bilaterally enlarged ovaries (14×12 cm left, 12×10 cm right) with massive ascites and a viable intrauterine pregnancy. She was diagnosed with severe sOHSS and managed conservatively with intravenous fluids, thromboprophylaxis, and therapeutic paracentesis.
Conclusion: The patient had an uncomplicated antenatal course and delivered a healthy term newborn. This case highlights the importance of recognizing sOHSS in spontaneous pregnancies and the efficacy of conservative management, even in low-resource settings.
Keywords
Spontaneous ovarian hyperstimulation, Pregnancy, Conservative management, Ascites, First-trimester pregnancy
Introduction
Ovarian hyperstimulation syndrome (OHSS) is a well-known and potentially serious complication of ovarian stimulation protocols used in fertility treatments. It is characterized by ovarian enlargement, ascites, electrolyte imbalances, and hemoconcentration. However, OHSS can rarely occur spontaneously in pregnant women who have not undergone any fertility interventions. This entity, known as spontaneous OHSS (sOHSS), presents a diagnostic challenge due to its rarity and non-specific symptoms. We present a case of a 19-year-old woman who developed severe OHSS during a spontaneous pregnancy, emphasizing the clinical presentation, diagnostic workup, and successful conservative management.
Case Presentation
A 19-year-old woman, Gravida III, Para I, Abortion I, presented to the Medical Outpatient Department with a chief complaint of progressive abdominal swelling of two weeks' duration. She reported amenorrhea for two months. She had a regular menstrual cycle and no history of undergoing any fertility treatments or taking ovulation-inducing medications. Notably, she recounted a similar history of abdominal swelling during her previous pregnancy, which resolved spontaneously within a few days. She had no history of chronic illness, medication use, alcohol consumption, or illicit drug use.
On physical examination, the patient appeared unwell but was in no acute respiratory distress. Her vital signs were: temperature 37.1°C, heart rate 106 beats per minute, blood pressure 110/90 mmHg, respiratory rate 22 breaths per minute, and oxygen saturation 92% on room air. Abdominal examination revealed significant distension with shifting dullness on percussion and bilateral flank fullness. Due to the patient's significant discomfort and the critical need to avoid unnecessary manipulation which could potentially rupture the fragile, enlarged ovarian cysts, a pelvic examination was deferred. This decision was made to prioritize patient safety and stability during the initial acute presentation.
Laboratory investigations revealed mild leukocytosis with neutrophilia, hyponatremia, and hypokalemia. Liver and renal function tests were within normal limits. A comprehensive hormonal panel to measure TSH, Free T4, LH, FSH, and estradiol was considered; however, these specific assays were unavailable at our facility during the patient's admission, representing a key limitation of this report. Serum beta-human chorionic gonadotropin (β-hCG) was elevated (>200,000 mIU/L).
A transabdominal ultrasound was performed and interpreted by an attending radiologist with expertise in obstetric and gynecological imaging (Figure1).
Both ovaries were significantly enlarged, measuring 14×12 cm on the left and 12×10 cm on the right (Figures 1A & 1B). An intrauterine pregnancy with a crown-rump length (CRL) consistent with a gestational age of 10 weeks (Figure 1C). They demonstrated multiple peripheral large follicles, giving a classic "ring of fire" or "spoke wheel" appearance. Massive anechoic free fluid was noted in the abdomen and pelvis (Figure 1D). All other solid abdominal organs were normal, with no evidence of lymphadenopathy or peritoneal thickening. The word "INVASIVE" appearing on image D is a machine-generated label from the ultrasound equipment and is not a clinical finding. All identifying information has been removed to protect patient confidentiality.
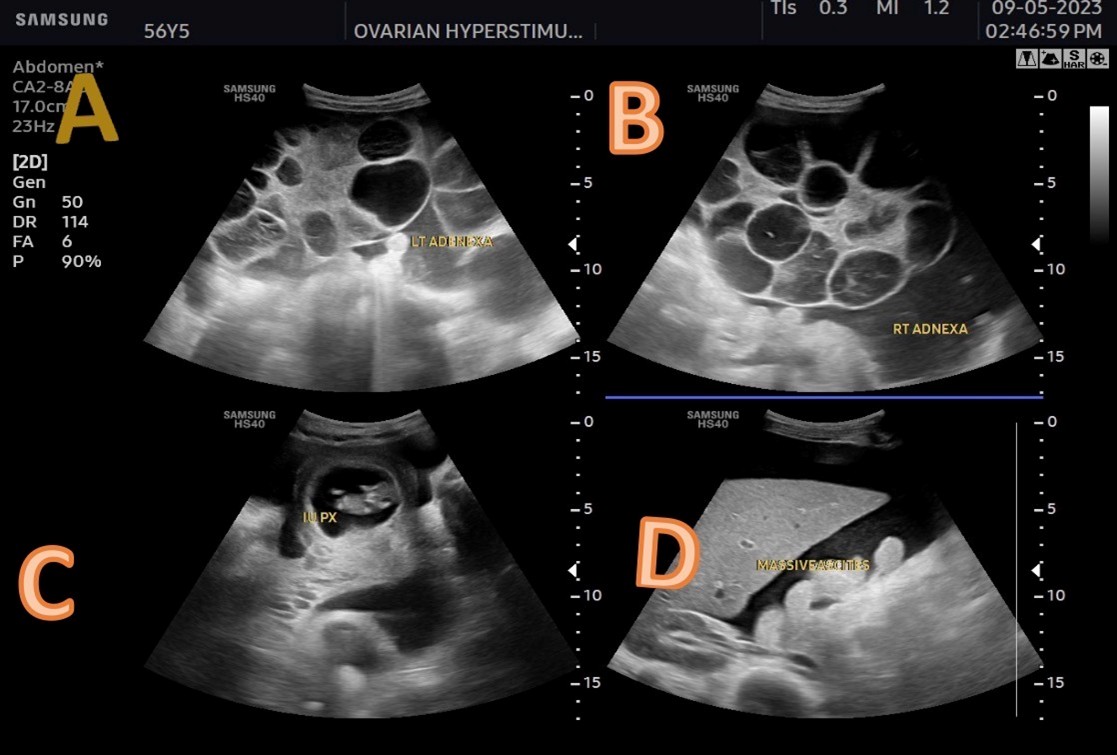
Figure 1. Findings from transabdominal ultrasound imaging.
Based on the clinical presentation, absence of fertility treatment, and characteristic ultrasound findings, a diagnosis of severe spontaneous ovarian hyperstimulation syndrome was made. The patient was admitted to the gynecologic ward. Management was primarily conservative and included: intravenous fluids for hydration; strict monitoring of vital signs and fluid balance; antiemetics (metoclopramide) and analgesics for symptom control; heparin 5,000 IU subcutaneously twice daily was administered as thromboprophylaxis given the patient's reduced mobility from massive ascites, the hypercoagulable state of pregnancy, and the documented risk of thromboembolic events in severe OHSS. Ceftriaxone 1,000 mg intravenously twice daily was initiated empirically due to the presence of leukocytosis and the theoretical risk of bacterial translocation across a tense, fluid-filled abdomen, though no definitive source of infection was identified. This was discontinued after 48 hours when cultures remained negative. A one-time therapeutic paracentesis was performed to relieve abdominal discomfort. The patient showed significant clinical improvement over the next few days, with resolution of symptoms and normalization of laboratory values. She was discharged home after four days of hospitalization with instructions for close obstetric follow-up.
Subsequent follow-up via telephone contact at 38 weeks gestation confirmed an uncomplicated antenatal course. The patient ultimately delivered a healthy, term newborn via spontaneous vaginal delivery without any complications. Both mother and infant were reported to be in good health at the six-week postnatal check. The successful term delivery following this severe first-trimester complication provides reassuring data on the potential for favorable obstetric outcomes with appropriate supportive care.
Discussion
Spontaneous ovarian hyperstimulation syndrome (sOHSS) is an exceedingly rare condition, with only a few hundred cases reported in the literature. It is distinct from iatrogenic OHSS as it occurs in the absence of exogenous gonadotropins or ovulation induction agents [1]. The incidence is difficult to estimate, but it is a diagnostic consideration that clinicians—especially in low-resource settings where fertility treatment is less common—must be aware of.
A clear diagnostic pathway was followed in this case: clinical presentation (respiratory distress, ascites) → ultrasound findings (enlarged multicystic ovaries, intrauterine pregnancy) → exclusion of iatrogenic causes (no fertility treatment) → laboratory correlation (elevated hCG, electrolyte imbalances). This pathway was explicitly stated as the basis for diagnosis given the resource limitations.
The pathophysiology of sOHSS is complex and not fully understood. The leading theories involve an abnormally high sensitivity of the follicle-stimulating hormone (FSH) receptor to circulating hCG or cross-reactivity of very high hCG levels with the FSH receptor [2,3]. In a normal pregnancy, hCG peaks around 8–12 weeks of gestation, which correlates perfectly with our patient's presentation at 10 weeks. Mutations in the FSH receptor gene can make it promiscuous, allowing it to be activated by hCG and TSH, leading to the clinical syndrome [4].
Furthermore, conditions associated with very high hCG, such as multiple pregnancies, hydatidiform moles, or hyperplacentosis, are also risk factors [5]. Our patient's history of a similar, spontaneously resolving episode in a prior pregnancy strongly suggests an underlying genetic predisposition, such as an FSH receptor mutation, although genetic testing was not available in our setting.
The diagnosis of sOHSS relies on a high index of suspicion. The differential diagnosis for abdominal pain and ascites in the first trimester is broad and includes ovarian torsion, ruptured ectopic pregnancy, hemorrhagic ovarian cyst, and malignancy [6]. Ultrasound is the cornerstone of diagnosis, revealing the characteristic bilaterally enlarged, multicystic ovaries (often described as "giant theca lutein cysts") with massive ascites, in the context of an intrauterine pregnancy [7]. The presence of a similar history in a previous pregnancy, as seen in our case, is a key indicator that should immediately alert the clinician to the possibility of recurrent sOHSS.
Based on clinical and imaging findings, ovarian hyperstimulation syndrome, including the spontaneous type, is classified into three categories and five grades according to the modified Golan classification [11,12]:
- Mild OHSS: characterized by bilateral multicystic ovarian enlargement
- Grade 1: abdominal distention and discomfort
- Grade 2: Grade 1 with nausea, vomiting, and/or diarrhea, and ovarian enlargement from 5-12 cm
- Grade 1: abdominal distention and discomfort
- Moderate OHSS: characterized by ascites and abdominal distension
- Grade 3: features of mild OHSS with ultrasonographic evidence of ascites
- Grade 3: features of mild OHSS with ultrasonographic evidence of ascites
- Severe OHSS: characterized by hypovolemia, hemoconcentration, thrombosis, oliguria, pleural and pericardial effusion
- Grade 4: moderate OHSS with clinical evidence of ascites and/or hydrothorax and dyspnea
- Grade 5: Grade 4 with change in blood volume, hemoconcentration, coagulation abnormalities, and diminished renal perfusion and function
- Grade 4: moderate OHSS with clinical evidence of ascites and/or hydrothorax and dyspnea
Our patient presented with significant ascites, tachypnea (RR 26), and hypoxia (SpO2 92% on room air), which constitutes clinical evidence of respiratory compromise secondary to ascites and possibly subdiaphragmatic irritation or early hydrothorax. Therefore, despite being classified as Grade 3 based on the initial ultrasound finding of ascites alone, the presence of respiratory distress and hypoxia places her presentation more accurately within the spectrum of Grade 4 severity. This underscores the dynamic nature of OHSS and the need for clinical correlation alongside imaging findings. The clinical findings resolved completely in the second trimester.
The syndrome is usually self-limiting in most cases and management is mainly supportive; however, cases with fatal outcomes have been reported [13]. Severe cases require hospitalization and close monitoring of hematocrit, liver function, renal function, serum electrolytes, and oxygen saturation.
This case contributes to the literature by detailing the clinical course and successful conservative management of severe sOHSS in a low-resource setting, where access to advanced hormonal testing is limited. It underscores the critical role of thorough clinical assessment and ultrasonography by skilled operators in reaching a timely diagnosis when a full endocrine workup is not feasible. The recurrence of symptoms in a previous pregnancy, as noted in the patient's history, supports existing evidence of a possible familial or recurrent pattern in some patients with sOHSS, which is an important clue for clinicians.
Management of sOHSS is primarily conservative and supportive, mirroring the approach to iatrogenic OHSS, as the condition is usually self-limiting and resolves as hCG levels plateau or decline in the late first trimester [8]. The goals of management are to maintain intravascular volume, correct electrolyte imbalances, prevent thromboembolic complications, and provide symptomatic relief. Aggressive surgical intervention is avoided due to the high risk of pregnancy loss. Paracentesis is reserved for cases with severe abdominal pain or respiratory compromise due to massive ascites [9]. Our patient responded well to this conservative approach, with complete resolution of symptoms and a good pregnancy outcome. The use of prophylactic heparin in this case was justified by the patient's immobilization and high thrombotic risk, while the short-course antibiotics were a precautionary measure in the absence of overt infection, reflecting a risk-averse approach in a severe presentation.
This case has several limitations. We were unable to perform genetic testing to confirm a possible FSH receptor mutation, nor could we measure levels of specific hormones like estradiol or inhibin. The diagnosis was made on strong clinical and ultra sonographic grounds.
In conclusion, this case highlights that spontaneous OHSS, though rare, can occur and should be considered in any pregnant patient presenting with acute abdominal distension and ascites. A detailed history, including prior pregnancy complications, is crucial. A conservative, supportive approach is safe and effective, leading to favorable maternal and fetal outcomes. We hope this report increases awareness of this condition among healthcare providers in all settings.
Data Availability
The data used to support the findings of this study are available from the corresponding author upon reasonable request.
Ethical Approval
The report was conducted as per the Declaration of Helsinki. At Haramaya University’s Health Science Campus, the Institutional Review Board granted ethical clearance, including publishing this patient’s case information. The patient’s privacy and confidentiality were protected.
Consent
The patient gave written informed consent for this case report and any related images to be published.
Conflicts of Interest
The authors declare that they have no conflicts of interest.
Authors’ Contributions
All authors contributed to data analysis, drafting, or revising of the article, have agreed on the journal to which the article will be submitted, gave final approval of the version to be published, and agree to be accountable for all aspects of the work.
Acknowledgments
The authors thank the patient for giving permission for the case details to be written.
References
2. Vasseur C, Rodien P, Beau I, Desroches A, Gérard C, de Poncheville L, et al. A chorionic gonadotropin-sensitive mutation in the follicle-stimulating hormone receptor as a cause of familial gestational spontaneous ovarian hyperstimulation syndrome. N Engl J Med. 2003 Aug 21;349(8):753–9.
3. Smits G, Olatunbosun O, Delbaere A, Pierson R, Vassart G, Costagliola S. Ovarian hyperstimulation syndrome due to a mutation in the follicle-stimulating hormone receptor. N Engl J Med. 2003 Aug 21;349(8):760–6.
4. Montanelli L, Delbaere A, Di Carlo C, Nappi C, Smits G, Vassart G, Costagliola S. A mutation in the follicle-stimulating hormone receptor as a cause of familial spontaneous ovarian hyperstimulation syndrome. J Clin Endocrinol Metab. 2004 Mar;89(3):1255-8. Corrected and republished in: J Clin Endocrinol Metab. 2004 Apr;89(4):1255–8.
5. Ludwig M, Gembruch U, Bauer O, Diedrich K. Ovarian hyperstimulation syndrome (OHSS) in a spontaneous pregnancy with fetal and placental triploidy: information about the general pathophysiology of OHSS. Hum Reprod. 1998 Aug;13(8):2082–7.
6. Fauser BC, Van Heusden AM. Manipulation of human ovarian function: physiological concepts and clinical consequences. Endocr Rev. 1997 Feb;18(1):71–106.
7. Hamoda H, Drakeley AJ, Brian K, Evbuomwan IO, Mathur R; Royal College of Obstetricians and Gynaecologists. The Management of Ovarian Hyperstimulation Syndrome Green-Top Guideline No. 5. BJOG. 2026 Apr 13.
8. Practice Committee of the American Society for Reproductive Medicine. Electronic address: ASRM@asrm.org; Practice Committee of the American Society for Reproductive Medicine. Prevention and treatment of moderate and severe ovarian hyperstimulation syndrome: a guideline. Fertil Steril. 2016 Dec;106(7):1634–47.
9. Alzebidi JA, Almushri K, Elmoheen R. Spontaneous Ovarian Hyperstimulation Syndrome Associated With Primary Hypothyroidism. Cureus. 2023 Jan 2;15(1):e33247.
10. Delvigne A, Rozenberg S. Epidemiology and prevention of ovarian hyperstimulation syndrome (OHSS): a review. Hum Reprod Update. 2002 Nov-Dec;8(6):559–77.
11. Golan A, Ron-el R, Herman A, Soffer Y, Weinraub Z, Caspi E. Ovarian hyperstimulation syndrome: an update review. Obstet Gynecol Surv. 1989 Jun;44(6):430–40.
12. Golan A, Weissman A. Symposium: Update on prediction and management of OHSS. A modern classification of OHSS. Reprod Biomed Online. 2009 Jul;19(1):28–32.
13. Semba S, Moriya T, Youssef EM, Sasano H. An autopsy case of ovarian hyperstimulation syndrome with massive pulmonary edema and pleural effusion. Pathol Int. 2000 Jul;50(7):549–52.