Abstract
Routine implementation of guide extension catheters in percutaneous coronary intervention (PCI) has significantly increased success rates in challenging anatomies, such as in tortuous and severe calcified vessels. Recently, the “Child-In-Mother technique” has been tested successfully in carotid artery stenting (CAS) in patients with severe tortuosity of the common or internal carotid artery (ICA).
In the present report, we propose to use the “Child-in-Mother technique” to facilitate the delivery of a carotid stent in an ectatic, thrombotic and tortuous right coronary artery (RCA) in a patient presenting with acute coronary syndrome (ACS).
Keywords
Acute Coronary Syndrome, Coronary Artery Disease, Interventional Cardiology, Percutaneous Coronary Interventions
Abbreviations
PCI: Percutaneous Coronary Intervention; CAS: Carotid Artery Stent; ICA: Internal Carotid Artery; RCA: Right Coronary Artery; ACS/NSTEMI: Acute Coronary Syndrome without ST segment elevation; CAD: Coronary Artery Disease; DAPT: Dual Antiplatelets Therapy; POBA: Plain Old Balloon Angioplasty; IVUS: Intravascular Ultrasound
Introduction
The use of the guide extension catheter, a coronary device for complex interventions, has emerged as an efficacy and safe solution to overcome very challenging cases where, even after successful dilatation with balloons, the stent does not cross the lesion limiting the ability to perform coronary interventions effectively, especially in tortuous and calcified vessels [1,2].
Recently, we have proposed the "Child-in-Mother Carotid Stent technique" to perform CAS in challenging anatomies, using an 8 Fr Guideliner V3 catheter (Teleflex) and Precise Pro Rx (Cordis) or Carotid Wallstent (Boston Scientific) with excellent results [3].
We present a case of ectatic RCA PCI, in which we were not able to advance carotid stents due to the severe tortuosity of the vessel. The issue was solved by inserting the carotid stent in an 8 Fr Guideliner V3 catheter in the "Child-in-Mother" fashion.
To our knowledge, this is the first case in literature that describes using the "Child-In-Mother" technique to deliver carotid stents to treat coronary artery disease (CAD).
Case
A 62-year-old gentleman with a history of hypertension was referred for PCI of an ectatic RCA. He was admitted for acute coronary syndrome without ST-segment elevation (ACS/NSTEMI). The coronary angiography showed critical stenosis of ectatic mid-RCA with high thrombus burden (TIMI thrombus grade 4). We evaluated different treatment options, including thrombus aspiration, plain-old balloon angioplasty (POBA) and standard PCI with large drug-eluting stent (DES) platforms. However, due to the large vessel size and increased risk of severe stent malapposition, we considered none of these options safe and effective for the patients, so we chose a carotid stent to perform PCI.
Vascular access was established using the right femoral 8 Fr conventional sheath, and the Amplatz Left 1 8 Fr guide was used to engage RCA. After a dilatation with a non-compliant balloon 3.5 mm at 18 atm, the carotid artery stent failed to advance due to tortuosity in the proximal and mid-segment of the RCA. The issue was solved by inserting a Guideliner V3 (Teleflex) 8 Fr to support the advancement of nitinol carotid artery stents PRECISE PRO RX 7x40 mm (Cordis) and PRECISE PRO Rx 7x20 mm (Cordis). Finally, post-dilatation was done with a non-compliant balloon 6.0 mm up to 24 atm with an excellent angiographic result (Figure 1).
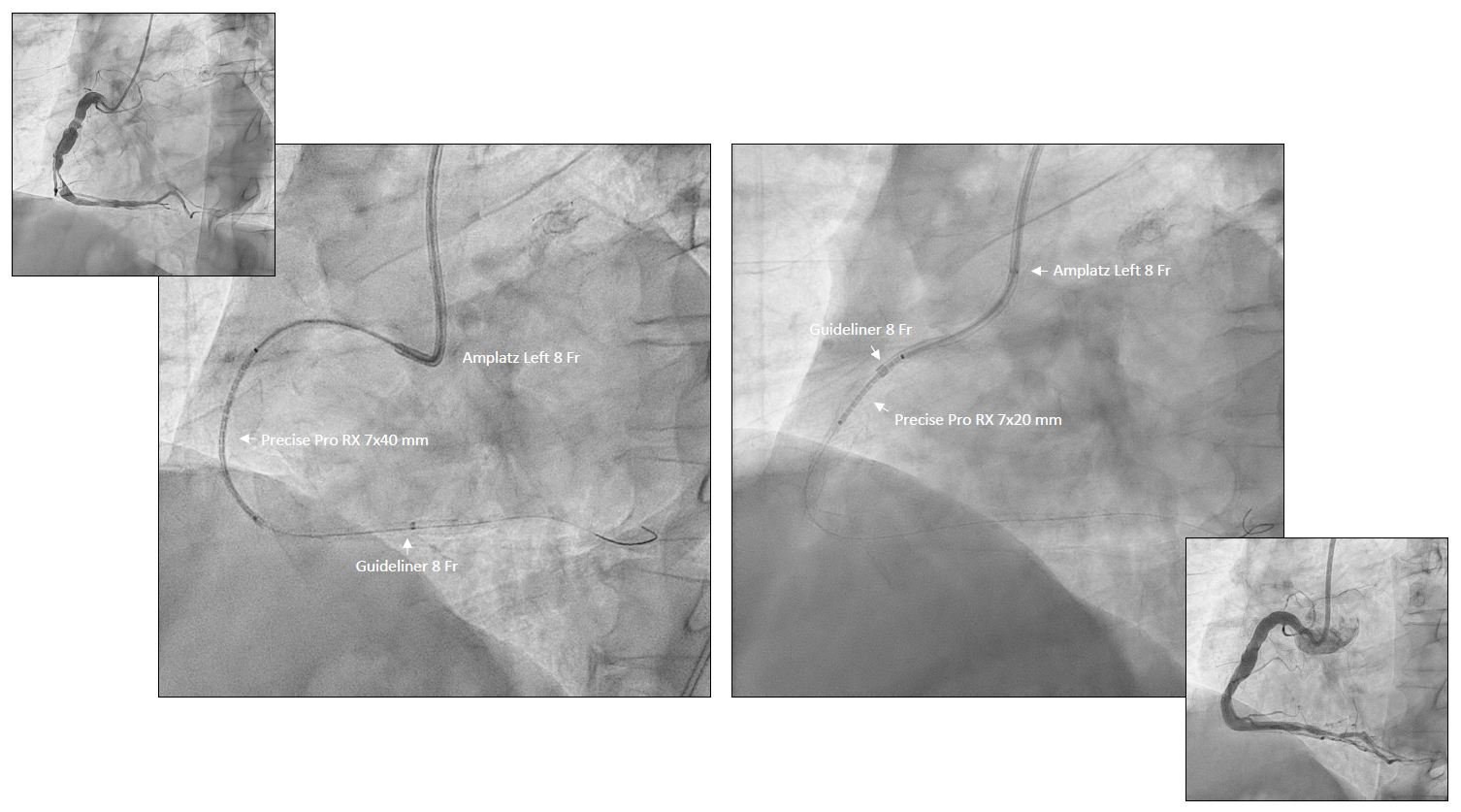
Figure 1. PCI on ectatic RCA with Guideliner and carotid stent with Child-In Mother technique.
Follow-up
The patient had no postprocedural complications with no angina recurrences. A planned angiographic follow-up was performed at 6 months showing patency of the carotid stents in the mid-RCA with optimal apposition after intravascular ultrasound (IVUS) examination (Figure 2). Prolonged dual antiplatelet therapy (DAPT) with Aspirin and Ticagrelor was indicated.
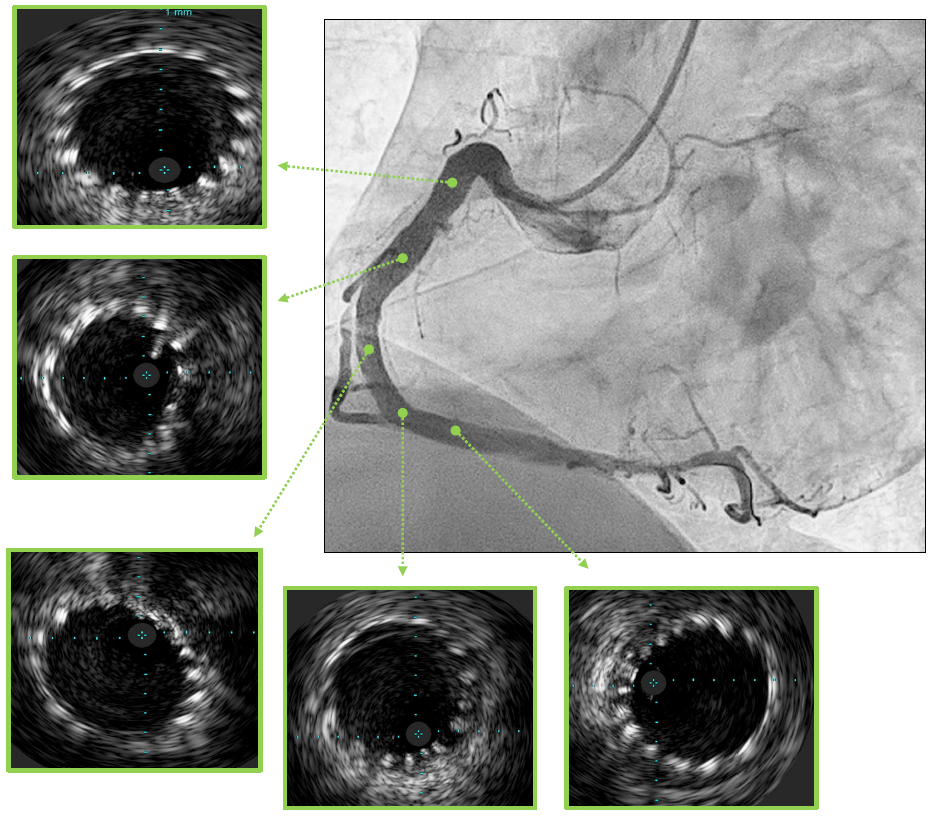
Figure 2. Angiographic follow-up.
Discussion
The treatment of the coronary artery disease of the aneurismatic RCA in the ACS setting is uncertain. Due to its high thrombus burden, it often requires a staged procedure to minimize the no-reflow risk. The ongoing RIGHTMARE study (Clinical Trials.gov ID NTC05713201) will clarify the best strategy to treat aneurismatic RCA in the acute setting.
In the present case, the main concern was the large lumen of the RCA in the presence of a high-thrombotic burden in the mid-segment of the vessel. The conventional drug-eluting stent platform cannot reach a satisfactory lumen apposition leading to a high risk of subsequent stent thrombosis. Another option should be to consider performing POBA, but the acute setting and high-burden thrombus did not make it safe for the patients.
Thus, we decide to consider an off-label use of a sizeable carotid artery stent to cover unstable plaque in the mid-segment of the RCA. Considering the tortuosity in the proximal and mid-segment of the vessel, we decided to use a more flexible open-cells, nitinol carotid artery stent-like PRECISE PRO Rx (Cordis). However, unfortunately, it did not cross the lesion.
In case of inability to advance the stent in the target site of the coronary artery, using the extension catheter with the "Child-In-Mother" technique can resolve the issue and safely deliver the stent to the target site [1]. However, this technique is tested in percutaneous coronary interventions using the ordinary DES, compatible with the guide extension's inner lumen. In our case, we had an aneurismatic RCA unsuitable to the conventional DES size, so we decided to use a larger carotid stent. On the other hand, using the carotid artery stents through the guide extension catheter has never been tested in the PCI setting, so compatibility between the stent size and the inner lumen of the guide extension remains unknown.
Recently, we have successfully performed carotid artery stenting cases using the "Child-In-Mother" technique derived from PCI using the Guideliner V3 8 Fr and three types of carotid artery stents, Precise Pro Rx 7/40 mm (Cordis), Precise Pro Rx 8/30 mm (Cordis) and carotid Wallstent 7/30 mm (Boston Scientific) [2]. On this basis, with excellent results, we have translated a similar technique, called "The Child-In-Mother Carotid stent" technique, in the PCI setting. To our knowledge, this is the first case report in the literature in which the "Child-In-Mother technique" is used to deliver carotid artery stent in the PCI setting. We proposed the "Child-In-Mother Carotid Stent" technique to treat aneurismatic RCA with severe anatomy in which a guide extension catheter safely delivers a carotid artery stent in the target site.
Limitations
Our case carries some limitations. Firstly, we used only the Guideliner V3 8 Fr, and we cannot guarantee that this technique is reproducible with other guide extension catheters. Second, we have tested only three types of carotid artery stents, and we do not assume compatibility with other types of available carotid artery stents. So, we report compatibility between Guideliner and carotid stents based on our clinical experience (Table 1). Third, this case was performed via femoral 8 Fr access. This technique is not tested via radial access, representing the most common vascular PCI setting, especially in the acute setting. Fourth, using the carotid artery stent in treating coronary artery disease is off-label and requires experience with the carotid artery stenting technique. Finally, this case was suitable for large DES platforms like SYNERGY MEGATRON (Boston Scientific) and STENTYS X-POSITION S (Stentys S.A), reaching a maximum expansion limit of 6.0 mm. However, this approach was discouraged by the high risk of uncorrectable malposition of the stent with the consequent risk of early stent thrombosis.
|
|
GUIDELINER V3 8 FR (Teleflex) – ID 0.071” – 1.80 mm |
|
Wallstent 7 mm (Boston Scientific) (OD: 0.073” – 1.85 mm) |
Yes (tested) |
|
Wallstent 8 and 9 mm (Boston Scientific) (OD: 0.086” – 2.18 mm) |
No |
|
Precise Pro Rx 7 and 8 mm (Cordis) (OD: 0.065”- 1.65 mm) |
Yes (tested) |
|
Precise Pro Rx 9 mm (Cordis) (OD:0.078” – 1.98 mm) |
No |
|
X-ACT All sizes (Abbot Ltd) (OD:0.088” – 2.24 mm) |
No |
|
RX-ACCULINK all sizes (Abbot Ltd) (OD: 0.078 – 1.98 mm) |
No |
|
Roadsaver all sized (Terumo) (OD: 0.67-1.71 mm) |
Yes, not tested |
Conclusion
In summary, the "Child-In-Mother Carotid Stent technique” involves inserting the larger carotid artery stent inside the guide extension catheter. It could be helpful to safely deliver the carotid artery stent in the target site of the aneurismatic coronary vessel to perform PCI.
At the state of the art, this technique is reproducible with carotid stents and guide extension before being reported in the paper.
References
2. Kovacic JC, Sharma AB, Roy S, Li JR, Narayan R, Kim D-B, et al. GuideLiner mother-and-child guide catheter extension: a simple adjunctive tool in PCI for balloon uncrossable chronic total occlusions. J Interv Cardiol. 2013;26:343-50.
3. Piedimonte G, Rolfo C, Tomassini F, Quadri G, Franzè A, Cerrato E, et al. Carotid artery stenting with Child-In-Mother technique from percutaneous coronary intervention: Insights from single-center case series experience. Cardiovasc Revascularization Med. 2022:4-7.