Abstract
Over the last few years, more papers were published related to the usefulness of sciatic nerve ultrasound elastography in clinical practice. Ultrasound elastography is a diagnostic method, to measure elasticity and strain in tissues and organs. The aim of this review was to highlight the usefulness of sciatic nerve ultrasound elastography in clinical practice, strictly compared with electromyography and MRI findings. Sonoelastographic evaluation was performed predominantly in patients with deep gluteal syndrome (DGS). The results were processed by meta-analysis. In this review, in the final processing, 16 studies were identified, 4 with strain ratio, 12 with shear wave elastography. The data was collected in a timeframe of 2013 to 2019. Looking at the reviewed studies, different techniques were applied (quasi-static, ARFI and shear wave elastography), with various joint movements, several “region of interest”, non-standardized measurement units and patients with dissimilar pathologies. The review summary leads to conclude that sciatic nerve ultrasound elastography test is not well clinically standardized. The nerve and surrounding muscles have to be assessed by color scale and B mode. Determining strain index may be useful, on particular equipment and within the same institution. The shear wave technique provides us with more secure and direct results, comparable to those of other institutions and researchers. This method is the most proven for deep gluteal syndrome with a wide range of manifestations, unilateral lumbar disc hernia, the assessment of sports injuries, to study musculoskeletal activity, monitoring the course of rehabilitation and in monitoring postoperative recovery.
Keywords
Sciatic nerve elastography, Shear wave, ARFI, Strain elastography, Deep gluteal syndrome
Abbreviations
DGS: Deep Gluteal Syndrome; MRI: Magnetic Resonance Imaging; ARFI: Acustic Radio Force Impulse
Introduction
Ultrasound elastography is a diagnostic method, to measure elasticity and strain in tissues and organs. The aim of this review was to highlight the usefulness of sciatic nerve ultrasound elastography in clinical practice. Different changes affect the sciatic nerves through various diseases and conditions. The impingement, the pressure of the surrounding structures, the damage of the nerve sheath and altered nerve structure, influence the nerve resistances. It can be effectively ascertained by ultrasound elastography. In the last few years, there were more papers about sciatic nerve elastography with controversial messages. “It`s interesting, but not very useful” is very often the clinician`s statement. The sciatic nerve stretches and slide during normal joint movement. In case of entrapped or compressed conditions, it causes pain with a change in its elasticity [1]. The sciatic nerve roots descend from the lumbar plexus, passes through the pelvis with an exit on the sciatic notch inferior to the piriformis muscle [ 2-4]. Some authors believe that it is connected with deep gluteal syndrome (DGS) [5-7]. The clinical decision making depends on neurological examination, electromyography (EMG), and very often on pelvic and lumbar MRI [2,6]. Last few years, authors considered ultrasound elastography techniques in clinical decision making, strictly compared with MRI findings. The first announcement was based on strain elastography features [8,9], later acoustic force impulse (ARFI) data were involved [10,11], and at last, the experiences were surrounded with shear wave elastography [12-17]. The pain generated by a sciatic nerve lesion can be connected with ischiofemoral impingement and hamstring dysfunction, by a combination of hip extension, adduction and external rotation, by abnormal contact between the lesser trochanter of the femur and the ischium, and in those with the DGS [1-4]. DGS may manifest as a specific entrapment within the subgluteal space, including fibrous and fibrovascular bands, piriformis syndrome, obturator internus syndrome, quadratus femoris and ischiofemoral pathology, hamstring conditions, gluteal disorders or other orthopaedic causes [1-4,18]. Sonoelastographic evaluation of the sciatic nerve was also performed in patients with unilateral lumbar disc herniation [19,20].
Materials and Methods
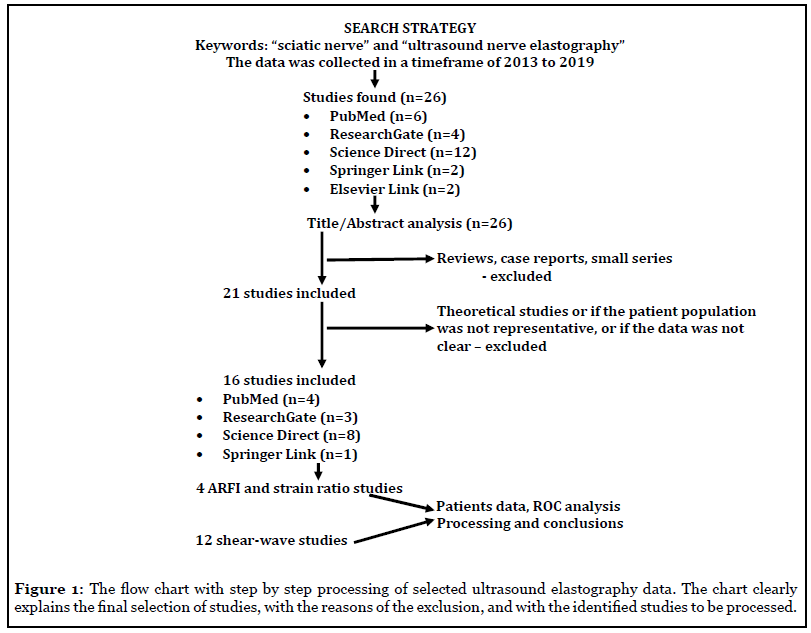
In 27 reviewed manuscripts the citations about sciatic nerve ultrasound elastography were identified. The case reports and small series (up to 5 cases), as well as the theoretical studies, non-representative population studies, or studies without clear data were excluded. In the final processing, 16 studies were identified, 4 with strain ratio. 12 with shear wave elastography. The final meta-analysis was done on patient data, elastography data, exercises data, ROC analysis, and by obtained processing. Figure 1 describes the flow chart with step by step processing of selected ultrasound elastography data. The data was collected in a timeframe of 2013 to 2019. The equipment has elastography supply. Looking at the reviewed studies, there were different techniques applied (quasi-static, ARFI and shear wave elastography), with various joint movements (“knee movement”, “limb movement”, “ankle motion”, “plantar or dorsal flexion”), at several positions of the transducer at the “region of interest”, nonstandardized measurement units and diverse pathology [8,10,12,14-17,19,21]. In 2013, Santos and Armada have tested sciatic nerve by ultrasound elastography [8]. In healthy people, there were higher percentages of blue color (hard properties) which conclude that sciatic nerve can be tested by color elastograms. That statement was confirmed in 2018 by Stajic et al. [10]. They conclude that it is possible to identify sciatic nerve conversions by color elastograms. One of the first announcement about different ultrasound elastography techniques was by Brandenburg and collaborators in 2014. The discussion was about the basic principles of ultrasound elastography techniques, including the strengths and limitations of their measurement capabilities [9]. Looking at the influence of elastography on rehabilitation, François Hug et al. [15], noted that there is growing evidence that elastography may be a useful tool in detecting subtle changes in muscle, tendon or nerve mechanical properties that occur early in the course of an injury or disorder. That should be important as an earlier detection can improve sports training and rehabilitation strategies. The quantification of muscle, tendon or nerve stiffness also provides insight into the mechanisms which may underlie treatment and rehabilitation programs and could ultimately assess their efficacy. Neto Tiago Goncalves in his doctoral thesis [17] processed the effects of neural tension by the sciatic nerve stiffness, in healthy people and people with low back related leg pain. The thesis aimed to determine the immediate effects of neural tension in the sciatic nerve stiffness. Andrade et al. reported the potential role of sciatic nerve stiffness in the limitation of maximal ankle range of motion (by shear wave elastography) [12,21]. Sciatic nerve stretching induced both, the decrease in the nerve stiffness and the increase in the maximal joint dorsiflexion. Greening and Dilley practiced shear wave elastography to examine the changes in peripheral nerve stiffness of upper (median nerve) and lower (tibial nerve) limb position by [13]. Dikici and his team [16] evaluated the tibial nerve with shear-wave elastography, as a potential sonographic method for the diagnosis of diabetic peripheral neuropathy. The conclusion was that the tibial nerve stiffness measurements appear to be highly specific in the diagnosis of established diabetic peripheral neuropathy. In 2018, Demirel and collaborators [22] also have showed that the muscle elasticity and tissue hardening increased on the problematic side, both on piriformis muscle and gluteus maximus. According to them ultrasound elastography may provide early diagnosis of piriformis muscle syndrome. The study of Ellis et al. [ 23] showed that ultrasound elastography was seen to be a reliable method for calculating sciatic nerve hamstring muscle interface by shear strain and sciatic nerve displacement. Using ultrasound elastography to quantify sciatic nerve displacement as the body moves, peripheral nerves are constantly being exposed to mechanical forces and stress from the surrounding tissues. Stajic et al. [ 10,11,24] concluded that the variation of the sciatic nerve is challenging for diagnostic and therapeutic procedure in many clinical and surgical cases. Quick ultrasound detection of the sciatic nerve makes surgical approaches more precise and effective, with a better outcome. This procedure could provide crucial information about the degree of nerve stiffness during the follow up [25]. In 2019, Celebi and collaborators [19] had shown results of elastography evaluation in patients with unilateral lumbar disc herniation. The experience directed to increase of sciatic nerve stiffness. Wang et al. [20] established the relationship of the shear wave elastography findings with unilateral lumbar disc herniation and clinical characteristics. According to their findings, ultrasound imaging can be considered as a very useful tool to detect changes in the sciatic nerve, due to disc herniation.
Results and Discussion
The significance of sciatic nerve color elastograms by quasi-static method was confirmed by Santos and Armada in 2013 [8] and by Stajic et al. in 2018 [10], presented in Table 1. Neto et al. and Hug et al. have confirmed the significance of shear-wave color scale [14,15] (Table 1). The correlation coefficient of color elastograms was 0.675. The correlation coefficient with MRI findings was 0.749. The ultrasound equipment upgraded with shear wave elastography gave a new opportunity [16]. It is based on direct measurement of muscle stiffness [22]. In the musculoskeletal field, the quasi-static method was rarely applied [15]. Stajic et al. have presented in 2018 and 2019 [10,11,24], the referent values of relative stiffness in asymptomatic patients, during extension and flexion knee movements (2.78 to 5.75SR) and in patients with DGS (7.32 to 11.97SR). The specificity was 93.5%, sensitivity 88.9%, with the accuracy 90.6%. They continued with follow up sciatic nerve stiffness in patients with the deep gluteal syndrome, who underwent surgery [25]. The neurodynamic sciatic nerve changings were noted by Francois Hug [15], in exercises of plantar flexion to dorsiflexion (from 1 to 7m/sec and by color scale). The shear wave features were presented in different conditions and diseases, respectively in healthy patients. Neto et al. [26] presented higher sciatic nerve stiffness compared to the unaffected limb (8.2 to 16.2m/sec and 9 to 13.6m/sec, P=.05) in patients with chronic low back leg pain. The resistance (shear-wave technique) in dynamic and unresisting knee extension was observed by Ellis [17]. The shear-wave resistance in active knee flexion knee was 73.06%, while in active knee extension 59.84%. The shear wave sciatic nerve stiffness was also tested during human ankle motion [12]. The shear wave velocity of the sciatic nerve significantly increased (p<0.0001) during dorsiflexion, when the knee was extended (knee 180°), but without changes when the knee was flexed (90°). The posture-induced changes by tibial nerve stiffness in different positions were 3.47 to 8.10 m/sec (Greening and Dilley) [13]. Çelebi and his team [19] assessed the sciatic nerve stiffness in patients with unilateral lumbar disc herniation and reported that on the axial (12.3kPA) and longitudinal (14.3kPA) planes of the involved side the sciatic nerve stiffness was significantly higher than non-involved side (6.8 and 8.3kPA) in the patient group (p<0.001). On the other side, Wang et al. [20] established sciatic nerve stiffness on affected side 20.4/27.5kPa (P<0.05), contrary to unaffected side 12.9/17.3kPa. Demirel and his team [22] have tested sciatic nerve in piriformis muscle syndrome by shear waves. The stiffness in piriformis muscle syndrome on painful side was 1.59m/sec (mean value), whereas it was 0.5 m/sec on normal side. The sciatic (tibial) nerve was evaluated by Dikici [16]. Patients with diabetic peripheral neuropathy had much higher stiffness values on both sides. A cutoff value proximal to the medial malleolus was 51.0 kPa, with the sensitivity of 90%. The variations of elastography score by several techniques in flexion and extension movements of painful limb are presented in Table 2. Due to these conditions, the correlation coefficient of elastographic measurements was low, r=0.195. Also, in comparison with other diagnostic findings (MRI, EMG) the correlation coefficient was not highly expected, r=0.465. The variations of elastography score in healthy persons are presented in Table 3. In several techniques involving flexion and extension limb movements, the correlation coefficient was significantly high, r=0.795. Looking at the demographic characteristics of few studies (Table 4), the average in patients groups was well-balanced, mean 42.4 years (p<0.05), as well as sex distribution.
| Color elastograms | |||
|---|---|---|---|
| Santos et al. 2013 (8) | Blue (hard) | Green/Yellow (soft) | quasi-static estimation |
| Stajic et al. 2018 (10) | Blue (hard) | Yelow/Red (soft) | quasi-static estimation |
| Neto et al. 2019 (14) | Yellow/Red (hard) | Blue (soft) | shear-wave estimation |
| Hug et al. 2016 (15) | Yellow (hard) | Blue (soft) | shear-wave estimation |
The correlation coefficient of color elastograms r=.675
The correlation coefficient with MRI findings r=.749
Table 1: The color elastograms were compared according to tissue elasticity.
| The Elastography Studies | In extension | In flexion |
|---|---|---|
| Neto et al. 2017 [14,17] | 8.2 m/sec (plantar) | 16.2 m/sec (plantar) |
| Greening et al. 2017 [13] | 3.47 m/sec (tibial) | 8.10 m/sec (tibial) |
| Celebi et al. 2019 [19] | 12.3kPa (leg) | 14.3kPa (leg) |
| Wang et al. 2019 [20] | 20.4kPa (plantar) | 27.5kPa (plantar) |
| Stajic et al. 2018 [10,11] | 7.32SR (knee) | 11.97SR (knee) |
| Ellis et al. 2018 [23] | 59.84% (knee) | 73.06% (knee) |
| Andrade et al. 2018 [21] | 1800 (ankle) | 900 ( ankle) |
| Demirel et al. 2018 [22] | 1.59 m/sec | |
| Dikici et al. 2017 [16] | 51.5kPa |
The correlation coefficient of elastographic measurements r=.195
The correlation coefficient with diagnostic (MRI,EMG) findings r=.465
Table 2:The variations of elastography score by different techniques in flexion and extension movements of painful limb.
| The Elastography Studies | In extension | In flexion |
|---|---|---|
| Neto et al. 2017 [14,17] | 9 m/sec (plantar) | 13.6 m/sec (plantar) |
| Celebi et al. 2019 [19] | 8.3 kPa (leg) | 9.8 kPa (leg) |
| Wang et al. 2019 [20] | 8 kPa | 17.7 kPa |
| Dikici et al. 2017 [16] | 12.9 kPa (leg) | 17.3 kPa (leg) |
| Stajic et al. 2018 [10,11] | 2.78SR | 5.75SR |
| Demirel et al. 2018 [22] | 0.5 m/sec |
The correlation coefficient of elastographic measurements r=.795
Table 3: The variations of elastography score by different techniques in flexion and extension movements in healthy persons.
| The Elastography Studies | Age | Gender (M/F) |
|---|---|---|
| Neto et al. 2017 [14] | 30.8 | 6/2 |
| Stajic et al. 2019 [25] | 43.5 | 12/12 |
| Wang et al. 2019 [20] | 44.5 | 7/13 |
| Celebi et al. 2019 [19] | 43.1 | 20/20 |
Table 4:The demographic characteristics (population with disease).
Conclusions
In this review it was concluded that ultrasound elastography was applied within different projects and studies, but clinical backup was not established. The ultrasound elastography was not involved in clinical and diagnostic pathways. However, the nerve and surrounding muscles must be assessed by color scale and B mode. A strain index may be useful, on particular equipment and within the same institution. The shear wave technique provides much more secure, direct results, comparable within various institutions and researchers, but it has to be standardized (m/sec or kPa). In correlation with MRI findings this method should be applied in deep gluteal syndrome with a wide range of manifestations, in unilateral lumbar disc hernia, in the assessment of sports injuries, to study musculoskeletal activity, in monitoring the course of rehabilitation and in monitoring postoperative recovery. Further investigations must be continued. The orthopedic and the ultrasound community must make agreement about principles in sciatic nerve ultrasound elastography examinations. According to this review the shear wave elastography must be a basic method. The color elastograms must be established (with subgroups). The region of interest (ROI) must be determined (intra or extra-neural or surrounding tissue) and the agreement looking at the validate cut off must be achieved. At last, in clinical practice the Ultrasound Elastography recommendations by European Federation of Societies for Ultrasound in Medicine and Biology (EFSUMB) must be respected.
References
2. Hernando MF, Cerezal L, Pérez-Carro L, Canga A, González RP. Evaluation and management of ischiofemoral impingement: a pathophysiologic, radiologic, and therapeutic approach to a complex diagnosis. Skeletal radiology. 2016 Jun 1;45(6):771-87.
3. Singer AD, Subhawong TK, Jose J, Tresley J, Clifford PD. Ischiofemoral impingement syndrome: a metaanalysis. Skeletal radiology. 2015 Jun 1;44(6):831-7.
4. Stafford GH, Villar RN. Ischiofemoral impingement. The Journal of bone and joint surgery. British volume. 2011 Oct;93(10):1300-2.
5. Martin HD, Reddy M, Gómez-Hoyos J. Deep gluteal syndrome. Journal of hip preservation surgery. 2015 Jul 1;2(2):99-107.
6. Hernando MF, Cerezal L, Pérez-Carro L, Abascal F, Canga A. Deep gluteal syndrome: anatomy, imaging, and management of sciatic nerve entrapments in the subgluteal space. Skeletal radiology. 2015 Jul 1;44(7):919-34.
7. Carro LP, Hernando MF, Cerezal L, Navarro IS, Fernandez AA, Castillo AO. Deep gluteal space problems: piriformis syndrome, ischiofemoral impingement and sciatic nerve release. Muscles, ligaments and tendons journal. 2016 Jul;6(3):384-396.
8. Santos R, Armada P. Sciatic nerve hardness measurement by using ultrasound elastography. Ultrasound in medicine and biology. 2013 May 1;39(5):S57.
9. Brandenburg JE, Eby SF, Song P, Zhao H, Brault JS, Chen S, An KN. Ultrasound elastography: the new frontier in direct measurement of muscle stiffness. Archives of physical medicine and rehabilitation. 2014 Nov 1;95(11):2207-19.
10. Stajic S, Vojvodic A, Carro LP, Gasic M, Markovic AM, Lukic G. Nerve stiffness - a challenge for ultrasound elastography. International Journal of Current Advanced Research. 2018;7(4):11773-11776.
11. Stajic S, Vojvodic A, Mihailovic J, Carro L. Diagnostic accuracy of ultrasound elastography for deep gluteal syndrome. European Congress of Radiology 2018.
12. Andrade RJ, Nordez A, Hug F, Ates F, Coppieters MW, Pezarat-Correia P, Freitas SR. Non-invasive assessment of sciatic nerve stiffness during human ankle motion using ultrasound shear wave elastography. Journal of Biomechanics. 2016 Feb 8;49(3):326-31.
13. Greening J, Dilley A. Posture-induced changes in peripheral nerve stiffness measured by ultrasound shearwave elastography. Muscle & Nerve. 2017 Feb;55(2):213- 22.
14. Neto T, Freitas SR, Andrade RJ, Gomes J, Vaz J, Mendes B, Firmino T, et.al. Sciatic nerve stiffness is not changed immediately after a slump neurodynamics technique. Muscles, Ligaments and Tendons Journal. 2017 Jul;7(3):583.
15. Hug H. Advancing musculoskeletal rehabilitation using elastography. Aspetar Sports Medicine Journal 2016 Jan;166-171.
16. Dikici AS, Ustabasioglu FE, Delil S, Nalbantoglu M, Korkmaz B, Bakan S, et.al. Evaluation of the tibial nerve with shear-wave elastography: a potential sonographic method for the diagnosis of diabetic peripheral neuropathy. Radiology. 2017 Feb;282(2):494-501.
17. Neto TG. Effects of neural tension in the sciatic nerve stiffness, in healthy people and people with low back related leg pain. 2017. http://hdl.handle.net/10400.5/15022.
18. Spencer-Gardner L, Bedi A, Stuart MJ, Larson CM, Kelly BT, Krych AJ. Ischiofemoral impingement and hamstring dysfunction as a potential pain generator after ischial tuberosity apophyseal fracture nonunion/ malunion. Knee Surgery, Sports Traumatology, Arthroscopy. 2017 Jan 1;25(1):55-61.
19. Çelebi UO, Burulday V, Özveren MF, Dogan A, Akgül MH. Sonoelastographic evaluation of the sciatic nerve in patients with unilateral lumbar disc herniation. Skeletal Radiology. 2019 Jan 1;48(1):129-36.
20. Wang Q, Zhang H, Zhang J, Zhang H, Zheng H. The relationship of the shear wave elastography findings of patients with unilateral lumbar disc herniation and clinical characteristics. BMC Musculoskeletal Disorders. 2019 Dec 1;20(1):438.
21. Andrade RJ, Freitas SR, Hug F, Le Sant G, Lacourpaille L, Gross R, et al. The potential role of sciatic nerve stiffness in the limitation of maximal ankle range of motion. Scientific Reports. 2018 Sep 28;8(1): 14532.
22. Demirel A, Baykara M, Koca TT, Berk E. Ultrasound elastography findings in piriformis muscle syndrome. The Indian Journal of Radiology & Imaging. 2018 Oct;28(4):412-8.
23. Ellis R, Rohan M, Fox J, Hitt J, Langevin H, Henry S. Ultrasound Elastographic measurement of sciatic nerve displacement and shear strain during active and passive knee extension. Journal of Ultrasound in Medicine. 2018 Aug;37(8):2091-103.
24. Stajic S, Vojvodic A, Carro LP, Mihailovic J, Gasic M, Lukic G. Role of sciatic nerve stiffness in surgical decision making and follow up in patients with deep gluteal syndrome. BioRxiv. 2018 Jan 1:390120.
25. Stajic S. et al. Follow Up of Sciatic Nerve Stiffness in Patients with Deep Gluteal Syndrome, Underwent Surgery. EC Orthopaedics 2019 Dec;10(12):1-11.
26. Neto T, Freitas SR, Andrade RJ, Vaz JR, Mendes B, Firmino T, Bruno PM, et.al. Noninvasive measurement of sciatic nerve stiffness in patients with chronic low back related leg pain using shear wave elastography. Journal of Ultrasound in Medicine. 2019 Jan;38(1):157-64.
27. Saftoiu A, Gilja OH, Sidhu PS, Dietrich CF, Cantisani V, Amy D, Bachmann-Nielsen M, et.al. The EFSUMB guidelines and recommendations for the clinical practice of elastography in non-hepatic applications: update 2018. Ultraschall in der Medizin-European Journal of Ultrasound. 2019 Aug;40(04):425-53.