Abstract
The coronavirus (COVID-19) outbreak occurred in China and spread to the whole world in a short period of time. The WHO (World Health Organization) named the viral disease as COVID-19 (Novel Coronavirus, SARS-CoV-2) on February 11, 2020. As per the reports till 16th August 2022, there have been 588,757,628 confirmed cases of COVID-19, including 6,433,794 deaths, reported to WHO. As of 8th August 2022, a total of 12,355,390,461 vaccine doses have been administered. The Pandemic, a type of biological disaster, is a phenomenon that requires proactive approach and successful risk management. In this study, the risk-emergency management implemented by Turkey and some other countries during the COVID-19 pandemic is examined, and it aims to contribute to the pandemic risk management issues/studies that need to be implemented in the future.
Keywords
COVID-19 Turkey, Pandemic, Risk Management, COVID-19
Introduction
Throughout history, epidemic diseases have left deep traces in society, including economic, political and demographic consequences, the deaths of millions of people, and the destruction of so-called invincible armies. People have developed resilience, experience and strategies against disasters they have faced in the past. Today, it is necessary to look at what purpose these strategies and experiences served in the COVID-19 pandemic. When the reactions of the countries against the COVID-19 pandemic faced by the whole world are examined, it is observed that the history of humanity does not encounter such epidemic diseases and acts as a new disaster. This was perhaps a situation we were not used to in the century we have been living. The main reason for this is that there are observable large social and cultural differences when the old and new pandemics are compared. We can say that outbreaks causing the death of many people in human history are more difficult to detect since these outbreaks have spread to limited geographies. However, today's outbreaks can be seen quickly in all geographies, and we can provide a rapid diagnosis as a result of the current developments in genetics and the analysis performed at low costs. The COVID-19 outbreak was first reported in Wuhan, China in December 2019, and a public health emergency was declared by the World Health Organization (WHO). Till 16th August 2022, there have been 588,757,628 confirmed cases of COVID-19, including 6,433,794 deaths, reported to WHO. As of 8th August 2022, a total of 12,355,390,461 vaccine doses have been administered were reported (Figure 1). The distribution of case numbers by region is given in Table 1.

Figure 1. WHO Coronavirus Disease (COVID-19) Dashboard (Data last updated: 2022/08/18).
| Americas | 173,610,001 |
| Europe | 245,289,313 |
| Eastern Mediterranean | 22,881,182 |
| Western Pacific | 78,879,202 |
| South-East Asia | 59,764,980 |
| Africa | 9,254,926 |
Although it is commonly believed that WHO is late to guide the world against the virus, later they developed strategies in the fight against it to minimize the impact in the public, social and economic area, cut off person to person contact, isolate patients in the early stages, identify and reduce the transmission/contamination from animal sources, reveal unknown information about the virus and, to speed up the research and convey information correctly. Understanding the basic mechanism of the virus is very important for effective treatment and drug development. Current treatments provide supportive care, but how the virus affects the immune system has not yet been determined [2]. New Coronavirus (COVID-19) is a deadly virus that is of great importance for global public health. It has spread to many countries around the world due to insufficient risk assessment of the urgency of the situation, causing many deaths.
Compared to SARS and MERS, the COVID-19 virus was found to spread more rapidly due to increased globalization and adaptation of the virus in all settings/environments. Therefore, this epidemic, which has been observed worldwide since December 2019, has led to changes and transformations in many areas including health, social, economy, education, and politics on a global scale. The disease can be easily transmitted from person to person. When a person with COVID-19 coughs, droplets from the nose or mouth settle on the surfaces in the environment and can infect people who inhale or touch these particles, depending on the virus load. The experiences have shown that the elderly and those with chronic diseases (such as high blood pressure, heart disease, lung disease, cancer) or diabetes can survive the disease more heavily than other groups or lose their lives [3,4]. The purpose of this study in the light of these data is to present the examples of risk-management and emergency implemented by Turkey and some other countries in the COVID-19 pandemic and to reveal the pandemic risk management that should be applied in the future.
Biological Disaster: Pandemic
Disaster is defined as events of natural origin or human origin that develop suddenly, interrupt or stop social life, cause loss of life and property and which mostly cannot be overcome with local capacity. Outbreaks and pandemics are also included in the category of biological disasters in the sub-category of human-technological disasters. Looking at the history, it is seen that humanity has encountered many pandemics such as plague, measles, yellow fever, Ebola, SARS. The risk management and proactive approach are very important in pandemics, just like in other disasters. Disaster management can be defined as the works and operations performed to reduce risks and prevent loss of life and property before, during and after the disaster. Disaster risk management has stages of risk reduction, mitigation, response, and recovery. In pandemics, it is necessary to apply the prevention stage before virus spread, the stages of risk reduction and response after the case is seen; furthermore, implement the recovery stages for the damaged system and for the secondary problems when the case starts to decrease and disappear. Therefore, in order to combat the pandemic, governments must create disaster-resilient society and resilient systems. Resilience can be defined as the sociological, psychological and physical capacity of a community and the system, the ability to overcome disasters and emergencies, to survive with the least damage and to regain balance [5].
Challenges and General Protective Measures
There are numerous reasons why pandemics have increased rapidly in recent years. Increasing human population, changing ecosystems, environmental degradation, climate change, frequency of travel, intervention in animal habitats and globalization are among the main reasons [6,7]. The difference in the number of cases and mortality rates in a country is related to the age of the population, population density, population mobility, compliance with measures, resilience of the health system and cultural behavior [8]. Outbreaks affect economies as well as people's health. In the 2003 SARS epidemic, the global economy lost an estimated $ 40 billion [9]. In the 2014 Ebola epidemic, the direct economic loss is reported to be 2.8 billion USD [10]. In the COVID-19 pandemic, global economic losses are estimated to be between $ 18-51 billion. The COVID-19 has emerged as the most dangerous epidemic threat globally. Researchers and virologists are struggling to find a cure and vaccine for this deadly disease [2]. Insufficiency of healthcare professionals and equipment may be inadequate to treat infected patients in high numbers. Moreover, some people who are contagious can be asymptomatic and they increase transmission of virus by continuing their social life and travel. These factors pose a challenge for scientists, healthcare professionals, and government officials to address and cover the situation. The government officials in all countries have taken various steps, such as self-quarantine, to ensure public safety and limit social interactions, while continuing efforts to minimize human contact by facilitating the closure of public places across the country. This will reduce the risk of spreading COVID-19 to humans by breaking the transmission chain and preventing the entry of new COVID-19 cases within a given time frame [2]. The virus can spread from person to person through small drops of nose or mouth when a person with COVID-19 coughs or breathes. Therefore, it is important to stay 1 m away from a sick person. Reports indicate that older people who previously had chronic conditions or people with diseases such as high blood pressure, heart disease, lung disease, cancer or diabetes developed more serious diseases than the others. In addition, some Asian populations have been reported to be more susceptible to COVID-19 infection than other racial populations. The protective measures given by WHO are as follows;
“a) Disinfecting your hands using an alcohol-based hand sanitizer kills the virus,
b) Avoid touching eyes, nose, and mouth while outside
c) Be conscious of the virus
d) Avoid crowded places, traveling, and gathering
e) Women who have babies are encouraged to breastfeed to increase their immunity.”
These general rules are methods used in Chinese experience and in previous pandemics. Slowing down the spread of COVID-19 cases and limiting the number of people in need of hospital care will significantly reduce the burden on the country's health system. It will also give researchers more time to develop a vaccine against COVID-19 [11]. In order to prepare for a possible increase in the number of cases, the health system capacity should be increased. Implementing a good risk management depends on the realization of successful communication and coordination strategies. Supply and supply chain management should also be strengthened. All these studies are carried out by the ministries of health, disaster agencies, municipalities, ministries of internal affairs, foreign ministries, ministries of economy, ministries of education, private sectors, NGOs and etc. since it requires an interdisciplinary approach covering many institutions and societies.
Examples from the World
Considering Asia's experience with pandemics and outbreaks, it can be said that Europe and the United States are less experienced in combating pandemics. North Korea, China, Japan, Hong Kong, Thailand, Taiwan, Vietnam have a culture of fighting similar epidemics. Japan faced the first cases with the detection of COVID-19 in several people on the Diamond Princess ship in January 2020, and then took severe measures. The schools were closed in early March. Flexible working system was launched. The spread of cases and the number of deaths were limited by avoiding public transportation and public areas. Loan packages were offered to small businesses in February [12]. In South Korea, sudden increases and high mortality rates were observed. There is an opinion that especially religious orders are effective in this spread. However, Taiwan, by benefitting from the 2003 SARS experience, took stringent measures and thus limited the spreading by applying excessive number of testings. Singapore also took strict measures and decided to quarantine and followed the movements of infected people. Thanks to these measures, the spread of cases could be significantly limited. Korean government hired hundreds of public health doctors, ran rapid and effective screening tests. By declaring 254 hospitals as public hospitals, it enabled the public to go to hospitals without fear of infection. She cooperated with religious groups, thereby, weekly meetings were held online, and collective ceremonies were canceled. The number of cases confirmed on 15 March was reduced to 75 thanks to the proactive actions of the government and the cooperation of citizens [13]. In these experiences, early detection of risk, risk perception, risk control and harm reduction studies seem to play a key role in preventing the spread of the disease [14].
In Europe, the highest number of cases by population was seen in Belgium, Italy, Spain and Germany. Relatively high number of deaths was observed in Italy and Belgium and a low number of deaths in Germany. The open border policy between the EU countries enabled the disease to reach/spread to England as well as France, Switzerland. In this process, the European Union (EU) mechanisms were initially found very slow in terms of preventive measures. For example, when the epidemic was on fire/flared up in Italy, on 26 February 2020 she asked for help from other countries [13]. However, EU member states started sending aid only in mid-March. In the next process, following the high numbers of cases and deaths, the European Commission encouraged to coordinate common European cooperation to strengthen health sectors and mitigate the socio-economic impact. The European Union has allocated € 10 million as a research fund. The United Kingdom (UK) government has also invested £ 20 million in research [15]. Local borders started to be closed first and then national borders. The EU became the epicenter of the pandemic.
While some states declared a state of emergency at an earlier stage, the U.S. declared a national emergency in the second week of March. Travel bans have been implemented, screening tests have been carried out and mandatory quarantine has begun. In addition, the United States (US) has suspended all entrances of immigrants and non-immigrants into the country and prohibited travel to risky areas [16]. The US government has provided around $ 50 billion in aid to states, cities, and regions. However, these financial and material assistance were not considered sufficient by most states.
COVID-19 Global Outbreak Measures in Disaster Risk Management and Policy of Turkey
After the first case occurred (11.03.2020), Turkey has followed disaster risk management and policy against the COVID-19 global epidemic. When the circulars published in line with all the measures on education, health, industry and public spaces with the understanding of social distance, and the prohibitions of entry and exit abroad, partial curfews made throughout this process; it is observed that controlled spread is targeted by considering the capacity of the health sector in the test, diagnosis and treatment triangle aiming at “Reducing the spreading risk of the epidemic to the maximum extent within the scope of fluctuation of economic policy to a minimum degree”.
Corona virus occurs in several subtypes of coronaviruses including HCoV-229E, HCoV-OC43, HCoV-NL63, and HKU1-CoV found in humans that can be easily transmitted from person to person [17]. Infection rate of the COVID-19 is the foremost issue to understand the risk of the disease. This importance is caused by missing data of accurate time path characterization of the coronavirus pandemic. These characterization profiles are found by rates of positive findings among persons who have been tested for infection. However, if the person has not been tested, infection data are missing . Testing is performed generally after the demonstration of symptoms associated with presence of infection or close contact with infected persons. Not tested but infected patients take in place in person those asymptomatic or pre-symptomatic carriers of the COVID-19 disease [18]. For the detection of the COVID-19, there are mainly three various ways including nasal swab test with q-PCR, serological tests, and CT results. Sensitivity of the tests are RT-PCR nasal swab 63%, pharyngeal 32%, swab chest CT 97%, and blood test ELISA 93-99% [19-21]. However, for the three methods some of the obstacles are available. Especially nasal swab test is only available for detection of live virus located within a person's nose or mouth [22]. On the other hand, for getting reliable results from serological tests, patients infected by COVID-19 must show antibody production against virus within the body [23]. Thus, we assume that cumulative and actual infection rate from COVID-19 higher than the reported rate.
The disease is mainly transmitted by droplets. In addition, the droplets emitted by sick individuals through coughing and sneezing are transmitted by touching the mouth, nose, or eye mucosa after contact with other people's hands. Since viruses can be detected in respiratory tract secretions of asymptomatic people, these people can be contagious. In a meta-analysis study by Khalili et al., the mean incubation time was calculated as 5.84 (99% Confidence Interval 4.8-6.8) days [24]. The median incubation time is 4.8 days [25]. Generally, the incubation period varies between 2-14 days. The contagious period of COVID-19 is not known exactly. It is thought that it starts 1-2 days before the symptomatic period and ends with the disappearance of symptoms [26]. Although RNA is detected negatively in infected people, it can become positive again later. It is accepted that such positivity is due to procedural reasons rather than reactivation or reinfections. Although the virus is found to be positive in the stool, especially after the second week of the disease, the fact that the virus has been produced from the stool sample of only one case. This transmission has not been reported so far suggests that fecal-oral transmission is unlikely. The virus is rarely found positive in blood and urine, and it is considered that the virus does not pose a safety problem in terms of blood banking. Apart from that virus was not detected in milk, vaginal swab, and sperm samples. The viral load is higher in the elderly. Viral load is an important marker for disease severity and prognosis. It has been shown that viral load is 60 times higher in severe cases than mild cases.
Basic reproduction number R0 is the number of different individuals that an infected individual will infect during the period of infectious disease in a population that is all susceptible [27]. If R0 is greater than 1, each existing infection will cause multiple new infections. The disease spreads among people and can cause an epidemic. In the modeling, it has been reported that the R0 for COVID-19 is between 2.76-3.25 in Italy, the average R0 in China is 3.28 and the median R0 is 2.79 [20,28,29]. The highest R0 value was reported as 14.8 on the Diamond Princess Ship at the beginning of the pandemic. The calculation of the outbreak in Turkey for 10 days while the R0 values of 9.6, 45 and 1:30 daily [11]. The transmission coefficient of the disease should be calculated at regular intervals in the outbreak and should be considered as one of the follow-up criteria for the outbreak. Thus, Social Immunity Level or Herd Immunity is a certain percentage of people in a society becoming immune to any infectious disease, it refers to the protection of the whole society against that disease. When taken as R0 2.2, the level of social immunity is calculated as 60% for COVID-19 [20]. Throughout all this information, studies on COVID-19 in our country started on January 10 and the first meeting of the Scientific Advisory Board of the Ministry of Health was carried out . Up to 31st December 2020, in Turkey 24,504,567 tests are performed in which 2,208,652 persons infected, 20,881 deaths, 2,100,650 patient recovering has been observed. On the other hand, in the whole World 81,475,053 cases were confirmed till 31st December 2020 [11].
Throughout the entire process, the risk-management operation procedure has been implemented to increase the social immunity and to expand the economy-health capacity to the maximum extent, by extending the process to an optimal degree, considering the spread-time scale of all precautionary studies carried out in Turkey. COVID-19 measures and risk management policy implemented between 10.01.2020-01.05.2020 are listed chronologically below (Tables 2 and 3).
| Date | Measures Taken - Outbreak Management in Society |
| 10.01.2020 | COVID-19 Operation center and Coronavirus Science Board were established within the Ministry of Health. |
| 24.01.2020 | At the airports, with the presence of the virus in other countries, especially the passengers from China, simultaneous scanning with the thermal cameras at the contact doors of the foreign contacts, measures were taken under the control of the health personnel and the risk management of the people with symptoms was planned. |
| 31.01.2020 | With the operation directed by the Ministry of National Defense (RSD), 34 Turkish citizens evacuated from Wuhan city of China and the crew were brought in a center turned into a quarantine hospital in Ankara, and risk management was conducted on the first experience and asymptomatic cases. |
| 03.01.2020 | All flights to and from China have been stopped. |
| 23.02.2020 | Border entry and exit measures were taken at the border upon cases in Iran. |
| 29.03.2020 | Precautionary flights were stopped mutually with Italy, South Korea, and Iraq. Field hospitals were set up in areas close to the Iraqi and Iranian borders. |
| 08.03.2020 | In some provinces, especially in Istanbul, disinfection procedures have been initiated for public transport and public gathering areas. |
| Date | Measures Taken - Outbreak Management in Society |
| 10.03.2020 | In the first case with a history of traveling to an epidemic European country, the persons with whom the patient was in contact after returning to the country were quarantined for precautionary purposes with information such as departure and return dates and the patient's anamnesis. |
| 12.03.2020 | The measures taken after the five-hour meeting attended by senior government executives were announced to the public and started to be implemented. Going abroad with special permission, sports competitions with the condition of playing without spectators were allowed, and overseas travel of the presidency was delayed. |
| 13.03.2020 | A circular was issued within the scope of the measures taken at the immigration removal centers. |
| 15.03.2020 |
Out of 10,330 people returning from Umrah, 5,392 were quarantined for precautionary measures in Ankara, and 4,938 in state dormitories in Konya. |
| The entrance and exit of passengers to and from Germany, Spain, France, Austria, Norway, Denmark, Sweden, Belgium, and the Netherlands were suspended. For the citizens who want to return from these countries, quarantine applications were made by returning within 2 days. | |
| 16.03.2020 | Public Rest and Entertainment Places were closed. |
| Education in primary, secondary and high schools as well as universities was interrupted. | |
| 17.03.2020 | The entrance and exit of passengers to and from England, Ireland, Switzerland, Saudi Arabia, Egypt, and the United Arab Emirates were stopped. |
| General Directorate of Population and Citizenship Affairs issued a circular within the scope of the measures taken in the Directorate of Population. | |
| 19.03.2020 | Football, volleyball, basketball, and handball leagues were postponed. |
| 20.03.2020 | All private hospitals and foundation hospitals were declared as pandemic hospitals. |
| Opengate mobile –e application was initiated enable people to convey requests and suggestions on 322 issues and in 17 different fields such as education, health, youth centers and social services. | |
| 21.03.2020 | Activities of hairdressers, barbershops and beauty centers were suspended. |
| Curfew was imposed on people aged 65 and over as well as those with chronic (lung, asthma, COPD, cardiovascular, kidney, hypertension and liver) diseases. | |
| A circular has been issued stating that all restaurants, patisseries and similar establishments with and without beverages can only serve without takeaway or takeaway. | |
| 23.03.2020 | Favipiravir was administered to intensive care patients and its effects were monitored and evaluated. |
| 24.03.2020 |
In the provinces and districts, all the markets were published to be open between 09:00 and 21:00, and a circular was issued within the scope of providing services by accepting a number of customers as much as one tenth of the area that provides direct service to the customer. In this circular, it was also accepted that the number of passengers could not exceed the 50% of the passenger capacity in intercity and urban transportation. |
| Respirator mass production started. | |
| Fund support was provided for vaccine production. | |
| 27.03.2020 | All marketplaces, especially bazaars, where the items such as clothing, toys, ornaments, bags, etc. are exhibited in displays and stalls that are not essentially needed to be sold are closed down. |
| 28.03.2020 | Circular on travel permit rules was published. Restrictions on traveling could only be lifted with a permit. |
| 29.03.2020 | Circular was published on the measures taken in commercial taxis. |
| In order to meet the personnel needs, the gendarmerie started to produce a daily mask with a capacity of 100,000. | |
| 30.03.2020 | Quarantine implementation was initiated in 39 settlements (1 town, 6 neighborhoods, 28 villages and 4 hamlets). |
| Okmeydani Training and Research Hospital was put into service with 600 beds. | |
| 31.03.2020 | Work has been started to increase the total number of 5,452 hospital beds in Istanbul. |
| A total of 75 active test centers were opened. | |
| 02.04.2020 | In this whole process, 81 provinces were monitored. Efforts to reduce mobility have been initiated in all cities. |
| 05.04.2020 | Studies have been started to distribute masks to all citizens aged 20-65. |
| 07.04.2020 | The “COMMUNITY SCIENCES COMMITTEE” was launched for the first time in the world. |
| 08.04.2020 |
Two new hospitals started to be constructed in Atatürk Airport and Sancaktepe. |
| Within a few days, the “application”, which is planned to be implemented in order to monitor whether the isolation rule is followed at home, has been developed. | |
| The virus was isolated for vaccination studies. | |
| “Pandemic Isolation Tracking Project” was initiated by the Ministry of Health. | |
| 09.04.2020 | After the Marmara University hospital was revised, its bed capacity of 535 was increased. |
| 03.04.2020 | Circular on city entry / exit measures and age restriction were published. |
| 05.04.2020 | Circular was published for street animals. |
| 06.04.2020 | 32,000 additional healthcare personnel were appointed. |
| 08.04.2020 | Quarantine implementation was initiated in 156 settlements (45 provinces, 2 district centers, 6 towns, 92 villages, 47 neighborhoods and 9 hamlets). |
| 09.04.2020 | A circular was issued for children and young people with special needs. |
| 10.04.2020 | A curfew was imposed on all citizens in 30 metropolitan cities and Zonguldak for two days (weekend). |
| 17.04.2020 | A curfew was imposed on all citizens in 30 metropolitan cities and Zonguldak for two days (weekend). |
| 20.04.2020 | The first phase of Istanbul Basaksehir City Hospital, which has the largest intensive care unit in Europe, was opened. |
| 22.04.2020 | Within the scope of Ramadan, the corona virus circular was published. |
| 23.04.2020 |
A curfew was imposed on all citizens in 30 metropolitan cities and Zonguldak for four days (23-24-25-26). |
| 26.04.2020 | Daily 50,000 test capacity has been reached. |
| 30.04.2020 | A curfew was imposed on all citizens in 30 metropolitan cities and Zonguldak province for four days (30-01-02-03). |
When Table 4 is examined; it is seen that the first steps of the coronavirus struggle are taken, with all the precautions and preparations to combat COVID-19 virus, before it has spread in Turkey.
| Date | Measures Taken - Outbreak Management in Society |
| 03.05.2020 | It was decided to extend the restrictions on entry and exit to 30 metropolitan and Zonguldak cities until 24:00 on May 04. |
| The 3-day curfew in 31 cities was issued on May 3 at 24:00. | |
| 04.05.2020 | The restriction on entering and leaving 23 metropolitan and Zonguldak cities was extended until 24:00 on May 19. Ministers of the Republic of Turkey R:T Erdogan after a cabinet meeting, arrangements relating to gradually stretching to the limit in overall May, June and July will be announced by or on. It has been published that people over the age of 65 can go out on one of the days of the curfew and for 4 hours. It has been reported that the intercity entry-exit restrictions for the cities of Antalya, Aydin, Erzurum, Hatay, Malatya, Mersin and Mugla have been canceled. |
| 05.05.2020 | Commercial taxis' traffic restrictions expired on May 4, 2020, at 24:00. For commercial taxis in Istanbul, Ankara and Izmir the single-double plate application will end as of May 5. |
| 06.05.2020 | The circular of opening beauty salons and hairdressers was issued. Minister of Health of Turkey Fahrettin KOCA reported about the normalization process and this new era of "controlled social life" as a designation. The curfew restriction exception circular for people aged 65 and above with chronic illnesses at the age of 20 and under was issued. |
| 07.05.2020 | Market places circular was sent to 81 provincial governorships |
| 08.05.2020 | Commercial taxi hygiene circular sent to 81 provincial governorships |
| 11.05.2020 | It has been reported that the malls will start serving as of May 11, provided that the rules are followed. On May 5, 2020, Industry and Technology Minister Mustafa VARANK stated that as of May 11, all the main automotive factories in the country will start operating again. It was reported that businesses such as hairdressers and beauty salons could start operations on May 11 |
| 10.05.2020 | 2-Day curfew in 24 cities expires on May 10, 24:00 |
| 12.05.2020 | A new circular on city entry and exit measures was issued to 81 provincial governorships |
| 13.05.2020 | Children up to the age of 14 were able to go out on 13 May between 11:00 and 15:00 within walking distance |
| 14.05.2020 | A total of 7,132,453 calls were made to Vefa Social Support Groups on 22 March-13 May, including 2,561,283 calls over 112, 858,686 calls over 155, 373,310 calls over 156, and 3,339,174 calls from other numbers. In these calls, the needs of our elder's 6,649,461 were met by social support groups |
| 15.05.2020 | The curfew restriction to be applied between 15.05.2020 24.00 and 19.05.2020 24.00 in 15 provinces. 15-20 age group was reported to be able to go out between 11.00 and 15.00 hours on Friday, May 15 |
| 15.05.2020 | Curfew days and hours have been reported for citizens aged 65 and over with chronic illnesses |
| 19.05.2020 | The curfew restriction decision to be applied in 81 provinces between 24.00 on 22.05.2020 and 24.00 on 26.05.2020 was reported |
| The ministry sent an additional circular on city entry-exit measures to 81 provincial governorships. With the circular, all entrances/exits to 14 provinces with metropolitan status and Zonguldak by land, air and sea (public transportation vehicle, private vehicle etc.) It was temporarily suspended until 24:00. Curfew Restrictions in 15 Provinces are decided to end on May 19, 24.00 | |
| Curfew Restrictions in 15 Provinces are decided to end on May 19, 24.00 | |
| 20.05.2020 | A travel permit circular has been issued to 81 provincial governorships for citizens aged 65 and over |
| 22.05.2020 | 4 before the restrictions come across the street today Turkey 103,785 workplaces were checked |
| Circular on congregational worship in Mosques and Masjids was stated that within the framework of the rules to be determined on Friday, May 29, 2020. It was decided that noon, afternoon and Friday prayers can be performed in mosques in congregation. | |
| 26.05.2020 | It was decided to end the 4-day curfew in 81 provinces on May 26 at 24.00 |
| 28.05.2020 | Curfew restrictions were imposed in 15 provinces between 29.05.2020 at 24.00 and 31.05.2020 at 24.00 |
| 29.05.2020 | Circular on the curfew of people under the age of 18 and 65 and over to 81 provincial governorships. Our citizens aged 65 and over are between 14.00-20.00 on Sunday, May 31, and children and young people between the ages of 0-18 on Wednesday, 03 June and Friday, 05 June, 14.00- Between 20.00 hours was decided to be limited to walking distance, to obey the distance rule and to wear a mask. |
| 30.05.2020 | Travel restrictions in 15 provinces have been terminated on May 31st at 24:00 and 81 provincial governorships have been granted permissions for restaurants, cafes, etc. workplaces, parks, picnic areas; reported in the circular on recreation areas and clothing markets |
| 31.05.2020 |
The curfew restrictions applied in 15 provinces were terminated as of May 31 at 24:00 and military discharge procedures were initiated |
| 01.06.2020 |
Ministry of national defense appointment, assignment and personnel recruitment activities were initiated |
| 05.06.2020 |
Summons to the ministry of national defense started |
| 13.06.2020 | It was reported that the circular of measures to be applied in the wedding ceremonies to 81 provincial governorships will serve as of 15 June. National Defense University military student candidate selection exam was held |
| 18.06.2020 | A circular on LGS and YKS measures was issued to 81 provincial governorships 2019-2020 academic year has been ended |
| 19.05.2020 | Curfews to be applied between 22.05.2020 24.00 and 26.05.2020 24.00 have been published The curfew restriction circular sent to 81 provincial governorships by our ministry was reported |
| 20.06.2020 | Ministry of National Defense paid military service started High school entrance exam (LGS) on 20 June, the LGS exam was held across the country on 20 June 2020. Curfew restriction applied during the exam |
| 24.06.2020 | Measures to be applied in wedding ceremonies stated that the decision was taken that wedding halls can start to serve in accordance with the rules determined as of July 1, 2020 |
| The curfews to be applied in 81 provinces within the scope of YKS measures will be made on 27-28 June. Higher education institutions exam was held on 27-28 June 2020. A curfew was imposed during the exam. | |
| 18.06.2020 | Circular on LGS and YKS measures was issued to 81 provincial governors |
| 26.06.2020 | Internet cafes, halls, and electronic game places circular to 81 provincial governorships were decided to operate from 1st July |
| 04.07.2020 | A circular on the measures to be taken regarding amusement parks and theme parks was issued to 81 provincial governorships |
| 07.07.2020 | All governors in Turkey coronavirus were decided to make the control measures |
| 21.07.2020 | In 81 provincial governorships, the circulars were sent about working hours of workplaces to restaurants, restaurants, cafes, coffeehouses etc. |
| Coronavirus measures were audited under the management and coordination of governors across the country | |
| 24.07.2020 | Ayasofya Mosque was opened and approximately 350 people attended the opening according to social distance rules |
| 29.07.2020 | Ministry of health decided to disclose only the number of cases by making patient case distinction |
| 30.07.2020 03.08.2020 | No curfew restriction was imposed on Eid al-Adha |
| 04.08.2020 | Additional circular on "COVID-19 measures" sent to 81 provincial governorships |
| 05.08.2020 | The most comprehensive coronavirus audit will be carried out in 81 provinces with the motto "for health, for all" in a controlled social life period |
| 06.08.2020 | It was decided to implement coronavirus controls measures throughout Turkey |
| 07.08.2020 | Engagement, wedding, coastal zone inspections circular was sent to 81 provincial governorships |
| 10.04.2020 | Trainings for associations are made available on the website of the interior affairs e-academy and the general directorate of civil society relations. |
| 14.08.2020 | A circular on isolation measures was notified to 81 provincial governorships |
| 18.08.2020 | It was decided to conduct coronavirus control in 81 provinces |
| It has been reported that private schools can be opened with distance education | |
| 22.08.2020 | Notifications started to come to the isdem practice implemented by our ministry within the scope of COVID-19 measures |
| 22.08.2020-26.09.2020 | 6,110,397 inspections were carried out within the scope of coronavirus measures |
| 25.08.2020-02.09.2020 | A circular was sent to 81 provincial governorships regarding events such as weddings, henna nights, engagements |
| 26.08.2020 | With the circular published by the presidency on August 26, rotation, flexible and remote work in public institutions and organizations was allowed |
| 31.08.2020 | It was decided to open schools with distance education |
| 05.09.2020 | Göztepe assoc.prof. dr.Suleyman Yalçin City Hospital was opened. |
| 08.09.2020 | Additional circular on coronavirus measures sent to 81 provincial governorships |
| 11.09.2020 | Dormitory requirement was imposed for those who escaped from isolation |
| 12.09.2020 | HES code obligation circular for intercity buses was sent to 81 provincial governorships |
| 15.09.2020 | Publicly accessible recreation and entertainment places circular was sent to 81 provincial governorships |
| 21.09.2020 | It was determined that face-to-face education could be started gradually and limited in classes and the gap would be eliminated through distance education, live lessons and eba TV. |
| 23.09.2020 | HES application was created |
| 24.09.2020 | A circular was sent to 81 provincial governorships on informing the contacts correctly |
| 30.09.2020 | Two circulars on HES code were sent to 81 provincial governorships |
| Comprehensive audit of the entire Turkey coronavirus was decided to carry out | |
| Explaining the distinction of patient and case definitions, Mr. KOCA said, "The number of new patients that are announced every day and that we focus on should be an issue of attention." | |
| 02.10.2020 | Konya City Hospital was opened. |
| In line with the relevant letter of the Ministry of Health and the recommendation of the coronavirus science board, the events to be organized by non-governmental organizations, professional organizations and higher organizations, associations, and cooperatives as of 02.10.2020 until 01.12.2020 will be postponed, taking into account the seasonal effects | |
| 05.10.2020 | The Minister of National Education, Ziya SELÇUK announced that as of October 12; all primary schools, village schools, 8th and 12th grades and schools for children with special needs will be opened. |
| 12.10.2020 | School buses and drivers were inspected |
| 18.10.2020 | An additional circular on the coronavirus outbreak was sent to 81 provincial governorships. It was decided to conduct a COVID-19 audit on a separate issue every day in the next 7 days. |
| 04.11.2020 |
Coronavirus additional measures circular was issued |
| 05.11.2020 | New period circular on coronavirus inspections were published |
| 06.11.2020-13.11.2020 | Coronavirus epidemic audits were performed daily by the audit team with approximately 42,407 personnel; 67,689 intercity public transportation vehicles, 152,261 urban public transportation vehicles, 73,847 commercial taxis, 12,627 marketplaces (district market, high society market, etc.) 500,863 crowded streets, boulevards and workplaces on the streets were checked |
| 13.11.2020 | Tekirdag City Hospital was opened |
| 10.11.2020 | 65 age restrictions imposed in Istanbul and Ankara A restriction was imposed on those aged 65 and over from going out to the streets except between 10.00-16.00. |
| 11.11.2020 | Additional circular on coronavirus measures was issued |
| 17.11.2020 | It was decided that all schools will continue online with distance education until the end of the semester. |
| 18.11.2020 | Coronavirus epidemic in line with new measures; people over the age of 65 will be able to go out between 10.00-13.00 and young people under 20 between 13.00-16.00. The working hours of businesses such as shopping centers, markets, restaurants, and hairdressers will be open between 10.00-20.00. Only take-away service will be applied in restaurants and cafes. It was decided to close the cafes and cinemas. Sports competitions will continue to be played without an audience. Carpet pitches will be closed, smoking will not be allowed in streets and squares and flexible working hours will be arranged in a way that will not create intensity in public and private sector workplaces. |
| 24.11.2020 | Ministry of Health announced that 12,000 health personnel will be appointed |
| 25.11.2020 | Turkey's Health Minister Fahrettin Koca said that they would begin to include asymptomatic cases. On 25 November 2020, 28,351 new positive cases and 6,814 new patients were announced. |
| 27.11.2020 | A circular was sent to 81 provincial governorships to postpone events with broad participation. Due to the increase in the coronavirus epidemic, the activities (including general assembly meetings) to be organized by the general assemblies of associations, non-governmental organizations, professional organizations and higher organizations of public institutions, unions and cooperatives were postponed for 3 months |
| 28.11.2020 | With the circular on restaurants in accommodation facilities, restaurants, patisseries, cafes, cafeterias can be opened between 10:00 and 20:00 only to provide take-away service. Restaurants or online food order companies stated that package service can be provided after 20:00 only by phone or by online order. |
| 01.12.2020 |
Countrywide on weekends until a new decision is made which includes the curfew will start at 21:00 on Fridays, cover all of Saturdays and Sundays, and finish at 05:00 on Mondays. As the first application, a curfew will be imposed for all our citizens, starting at 21:00 on Friday, 04.12.2020, and ending at 05.00 on Monday, 07.12.2020, and the practice will continue in the same way on the following weekends. |
| On 26th, 27th, 28th, and 29th November 2020, 24,695 audit teams and 8,168 marketplaces where 80,637 personnel were employed were inspected. 116,854 public transportation vehicles were inspected. | |
| 20 million doses in December 2020, 20 million doses in January 2021 and 10 million doses in February 2021, a total of 50 million doses of vaccine was signed with the Chinese government. | |
| 02.12.2020 | Restriction measures were increased. General curfew will be applied every weekday between 21:00 and 05:00 in the morning. On weekends, an uninterrupted restriction will be applied from 21.00 on Fridays to 05.00 on Mondays. Sectors such as production, supply, logistics, health, agriculture, and forestry are out of the scope. Businesses such as markets, grocery stores, greengrocers and places that provide home delivery services are excluded from the weekend restrictions within the specified hours. Restaurants will not be able to serve other than take-away service. The number of people who can attend weddings and funerals will not exceed 30. Shopping malls will apply the HES code. Activities such as mevlid, condolence and New Year's Eve celebrations where communities come together are prohibited. People over the age of 65 and under the age of 20 are prohibited from using public transportation. |
| 07.12.2020 | Close contacts remain in quarantine for 10 days. The quarantine of people who do not develop any symptoms during the quarantine period ends at the end of the 10th day without PCR, but these people continue the measures to be followed in the community. In addition, quarantine can be terminated at the end of the 7th day, according to the PCR test result for people who are in close contact and who do not develop symptoms during the follow-up. PCR test can only be done by taking samples at home after the 5th day at the earliest, if the capacity is suitable. Quarantine is terminated at the end of the 7th day in people who have a negative PCR test and do not develop symptoms. Quarantine cannot be ended before 7 days in close contacts. Employees can return to work on the 8th day. This practice is not applied in areas where high-risk people (elderly nursing homes, prisons, people with low immunity, etc.) are cared for, but these people continue the precautions to be followed in the society. |
| 10.12.2020 | Turkey Republic Health Ministry reported for the first time the total number of positive patients - 1,748,567. |
A struggle ground for the COVID-19 outbreak was prepared with the Science Board, which was found to operate by focusing on the process management and anti-virus experiences of countries which started to pass through this process earlier in coordination with the world, by focusing on recognizing/identifying the virus before facing the case, experiencing the decontamination process, and possible diagnosis-treatment methods scenarios.
By 31st December 2020, the total number of COVID-19 cases were 2,208,652 and number of deaths are 20,881 and recovered patients are 2,100,650. Graphs of COVID-19 cases and deaths number in Turkey were shown in Figures 2 and 3.
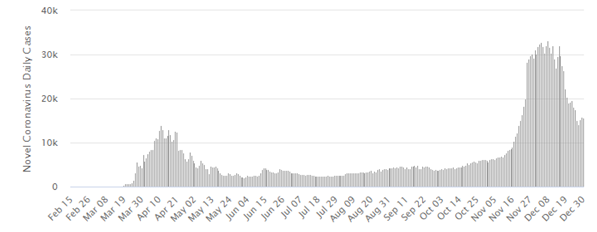
Figure 2. COVID-19 daily cases in Turkey [30].
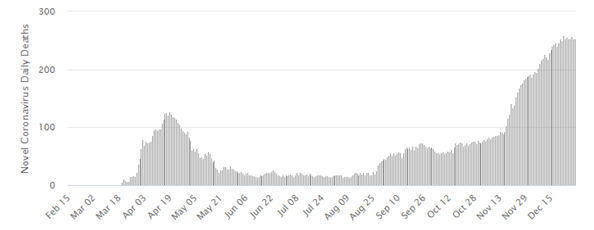
Figure 3. COVID-19 daily deaths in Turkey [31].
After the increase in the number of cases in Europe and then the first case seen in Turkey, it is clear that the measures taken both before and after the first case in our country are inadequate. When analyzing countries such as South Korea, China etc. which make decisions quickly and effectively in the fight against the virus as well as apply methods such as patient follow-up, quarantine, high number of tests and screening of the society in terms of viruses, we think that there are insufficient practices in the struggle in our country due to the lack of adequate and effective quarantine methods and insufficient number of tests.
In addition to these deficiencies, pandemics science committee should be created early, executing in the balance of political and scientific decision, after the start of the increasing cases increasing the number of tests, better implementation of Filiation and Isolation Tracking System (FITAS) and making the broadcasts that provide public awareness in everyday television can be considered as the direction in which Turkey was successful.
There are two approaches in disaster response, namely policy oriented and risk oriented. It has attempted to provide these balances in Turkey, early science: establishing in the struggle to be successful, a strong health system, more intense than made up for the number of maintenance units and the community that the young population has been active in confining the number of deaths can say.
In this review, we briefly evaluated the epidemic management policies implemented by the government in 3 stages. While addressing the practices applied in our country before the case was seen in Phase I and II. At the stage, we examined the restrictions and measures applied gradually after the first case was seen. In stepping into an epidemiologically successful process, III. We slowly lost control of the epidemic course with the controlled social life policy implemented at the first stage. As a result of the opening of Hagia Sophia in July, 24,350 people came together, we think that the spread of cases from Istanbul to other provinces in out-of-town transportation, which was not applied on July 28, before the quarantine period of those who had the risk of contamination completed, had a great effect. While only the number of patients was announced as of 29 July (total number of tests: 4,711,095 – total number of patients: 228,924 – total number of deaths: 5,659 – pneumonia rate in patients: 9.4% – the number of seriously ill patients: 542 – total number of recovered patients: 212,557 – number of positive patients for today: – not certain. – number of patients for today: 942 – number of tests for today: 45,712 – number of deaths for today: 14 – number of recovered patients for today: 996), it was stated that the number of positive cases was not announced as of September 30 (total number of tests: 10,380,261 – total number of patients: 318,663 – total number of deaths: 8,195 – pneumonia rate in patients: 6.4% – the number of seriously ill patients: 1516 – total number of recovered patients: 279,749 – number of positive patients for today: – not certain. – number of patients for today: 1.391 – number of tests for today: 112,098 number of deaths for today: 65 – number of recovered patients for today: 1,245). The positive cases were announced together with the number of patients on 25th November (total number of tests: 17,733,520 – total number of patients: 467,730 – total number of deaths: 12,840 – pneumonia rate in patients: 3.4% – the number of seriously ill patients: 4,641 – total number of recovered patients: 385,480 – number of positive patients for today: 28,351 – number of patients for today: 6,814 – number of tests for today: 164,547 number of deaths for today: 168 – number of recovered patients for today: 3.911). III. In the normalization process shown chronologically in the table, the epidemic management is desired to be taken under control again with the measures that were re-implemented in November. On 31st December in Turkey, General Coronavirus Table shows (total number of tests: 24,504,567 – total number of positive patients : 2,208,652 – total number of deaths: 20.881 – pneumonia rate in patients: 3.8% – the number of seriously ill patients: 3,918 – total number of recovered patients: 2,100,650. As of January, with the arrival of the vaccine to begin in Turkey and we thought we will be successful if applied early and can get the epidemic under control again [11].
Pandemic and Lessons Learned
This epidemic experiencing has caused the weakening of humanity that dominates all over the world. All the countries of the world have been weak in predicting and taking precautions against this global epidemic. Even, more importantly, it was disappointing in terms of the solidarity of the countries. The general belief is that nothing can be the same as before after the pandemic. “New normal” process, which will make its impact felt in many areas such as economy, education, mental health of people, eating habits, ways of working, health system, hygiene behaviors, will start. Research shows that people are already experiencing an increase in sleep disorders and anxiety levels.
When this epidemic is considered, it is seen that it does not affect all individuals in the society equally. When the mortality and hospitalized patient rates are analyzed, it is seen that individuals aged 65 and over are at great risk. Strict measures and practices aimed at protecting the elderly can also lead to some social problems. For example, it can also lead to misperception among elderly people that they are undesirable, and that this virus is specifically aimed at eliminating the elderly population that does not produce. In contrast, we understood how important the elderly is for our society. We have learned how important their experience and encouragement are in our success.
We have seen how important government agencies are in outbreaks. In this regard, some strategic and security institutions should be state-owned. Governments need to develop very rigorous policies, especially in food security and healthcare. The fact that state institutions are strong and effective is crucial for the rapid fulfillment of the basic needs of the people and the rapid implementation of land making mechanisms. There are such rules in both public and civil life, which are never seen as stretchable. But this virus showed us that all the rules in life are not more important than human life.
Due to this epidemic, we see that thousands of daily flights stop all over the world for a few months. Nobody could have imagined such a situation before the epidemic. Furthermore, we could not have predicted that some factory chimneys would not smoke, the number of vehicles that release thousand tons of carbon dioxide in our cities would fall to a minimum and would even bottom up with long home quarantines. Nobody could have predicted such a process all over the world. At a local level, such processes could be predicted. But an epidemic on this scale frankly caught all countries unprepared.
After the epidemic, we have seen that the unplanned development of cities, which we regard as an indisputable fact, is no longer a sustainable phenomenon. Increasing overpopulation in cities has made us more vulnerable to disasters. Additionally, our home life, which has become insignificant in urbanization and city life in the last century, has become our refuge today.
Due to the COVID-19 epidemic, the behaviors of people in the face of the curfew on certain days have brought the hidden fears in their memories to the fore stemming from the past disasters. For example, people's experiences in times of famine in the past have led them to unconsciously run markets and take more than they need. Even if there are global common aspects of risk perception, awareness, and struggle, they show some changes by country to country. The cultural structure is strongly connected with socio-economic characteristics. Nevertheless, international protocols should be implemented to combat global disasters such as pandemics. Lack of science-based decisions, lack of coordination and lack of proactive approaches ensure that the struggle fails. First, good hygiene and a robust immune system is the key in dealing with the disease. In addition, working from home, online education, online meetings are the concepts that have become more effective in our lives in this process [32].
Disaster risk assessment is a standard approach in risk reduction strategies. Sendai Declaration (2015-2030) promotes a pluralist approach to risk analysis [33]. It is important to increase multilateral cooperation and resilience of systems in the fight. It is certain that COVID-19 will be a very expensive lesson/bitter experience [34]. A strong and social health system is critical in the fight . Moreover, these days when long-term global recession is on the agenda, it is very important to start developing early improvement plans on issues such as economy, tourism, education and return to social life, etc. [35].
Discussion and Conclusion
Governments' attitudes towards a pandemic risk and their decisions can directly affect public health and cause the collapse of the health system. The first statements of the US President and the Prime Minister of England will be referred to as unsuccessful examples of managing risk in the future. Both heads of state had to revise their risk plans after these imprudent statements. In this process, it is very important that all countries should leave political concerns aside in the fight against outbreaks and be transparent, in order to combat the pandemic and to reveal the extent of the outbreak. When will the pandemic we are suffering end, and can we return to our previous life? Can we travel freely without a mask? It is very difficult to answer these questions already [21] . For example, the Spanish Flu, which emerged in Europe in 1918 and seen in many parts of the world, caused the deaths of millions of people (approximately 50 million). This number of deaths is even more than the losses in the First World War that continued at that time. We should not forget the experiences we have gained in Spanish Flu. For example, it is understood that more people died in the second wave due to the fact that the outbreak, that occurred in March, could not be controlled or some measures were loosened or not taken seriously (Figure 4) [36]. Therefore, we must be prepared for the second and third wave possibilities in order to avoid experiencing sufferings/pains of the past. However, for some reason, although we express the concepts such as “nothing will be the same as before” or “new world order”, it is seen that the old disasters are only remembered when they are repeated. Nowadays, it is told that there will be many changes and transformations in the future. Yet, it is very difficult to estimate the extent of these changes and transformations. Social events in our lives do not give precise results like mathematical equations.
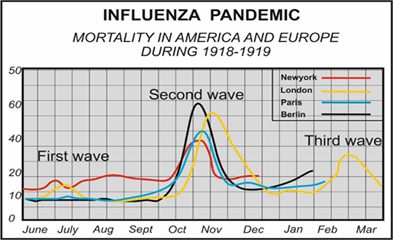
Figure 4. Deaths in America and Europe between 1918-1919 [37].
As a result, it seems impossible for this epidemic to end suddenly and to return to our previous habits and lives. Now we all need to be prepared for changes in our working life, habits, and education life. Additionally, in the new world order, all societies need to adapt quickly to change and transformation and create projections suitable for this change and transformation in their education. Lastly, global policies for this post-epidemic period need to be established.
References
2. Vellingiri B, Jayaramayya K, Iyer M, Narayanasamy A, Govindasamy V, Giridharan B, et al. COVID-19: A promising cure for the global panic. Science Of The Total Environment. 2020 Jul 10;725:138277.
3. Chen H, Guo J, Wang C, Luo F, Yu X, Zhang W, et al. Clinical characteristics and intrauterine vertical transmission potential of COVID-19 infection in nine pregnant women: a retrospective review of medical records. The Lancet. 2020 Mar 7;395(10226):809-15.
4. Wu Z, McGoogan JM. Characteristics of and important lessons from the coronavirus disease 2019 (COVID-19) outbreak in China: summary of a report of 72 314 cases from the Chinese Center for Disease Control and Prevention. JAMA. 2020 Apr 7;323(13):1239-42.
5. Varol N, KIRIKKAYA EB. Afetler karşısında toplum dirençliliği. Resilience. 2017;1(1):1-9.
6. Carroll D, Daszak P, Wolfe ND, Gao GF, Morel CM, Morzaria S, Pablos-Méndez A, Tomori O, Mazet JA. The Global Virome Project. Science. 2018 Feb 23;359(6378):872-4.
7. Smith KF, Goldberg M, Rosenthal S, Carlson L, Chen J, et al. Global rise in human infectious disease outbreaks. Journal Of The Royal Society Interface. 2014 Dec 6;11(101):20140950.
8. Peters A, Vetter P, Guitart C, Lotfinejad N, Pittet D. Understanding the emerging coronavirus: what it means for health security and infection prevention. Journal Of Hospital Infection. 2020 Apr 1;104(4):440-8.
9. James S, Sargent T. The Economic Impact of SARS and Pandemic Influenza. SARS in Context: Memory, History, Policy, ed. Jacalyn Duffin And Arthur Sweetman. McGill-Queen's Press. Retrieved on Mar. 2006;1:2020.
10. World Bank. 2014-2015 West Africa Ebola crisis: impact update. World Bank Fisc. Rep., 2016.
11. ARTİK Y, CESUR N, KENAR L, ORTATATLI M. Biological disasters: An overview of the COVID-19 pandemic in the first quarter of 2021. Afet Ve Risk Dergisi. 2021;4(2):163-82.
12. Schumaker E. Japanese expert who sneaked onto Diamond Princess cruise ship describes ‘zero infection control’ for coronavirus,” ABS News [Press release]. https//abcnews. go. com/Health/japanese-expert-sneaked-diamond-princess-describes-infection-control/story, 2020.
13. Djalante R, Shaw R, DeWit A. Building resilience against biological hazards and pandemics: COVID-19 and its implications for the Sendai Framework. Progress In Disaster Science. 2020 Apr 1;6:100080.
14. Artik Y, Varol N, Cesur NP. Hospital Disaster and Emergency Plan in Biological Disasters (HDEP): Coronavirus (SARS-CoV-2) COVID-19 Pandemic System Model Example. Journal Of Contemporary Studies In Epidemiology And Public Health. 2022;3(1).
15. European Commission. Coronavirus: EU Mobilises € 10 Million for Research.
16. Sohrabi C, Alsafi Z, O'neill N, Khan M, Kerwan A, Al-Jabir A, Iosifidis C, Agha R. World Health Organization declares global emergency: A review of the 2019 novel coronavirus (COVID-19). International Journal of Surgery. 2020 Apr 1;76:71-6.
17. Tan W, Zhao X, Ma X, Wang W, Niu P, Xu W, et al. A novel coronavirus genome identified in a cluster of pneumonia cases—Wuhan, China 2019− 2020. China CDC Weekly. 2020 Jan 1;2(4):61-2.
18. Artik Y, Cesur NP. General evaluation of COVID-19 diagnosis methods. Cohesive J Microbiol Infect Dis. 2022 Feb 7;5(5):000621.
19. Wang W, Xu Y, Gao R, Lu R, Han K, Wu G, et al. Detection of SARS-CoV-2 in different types of clinical specimens. JAMA. 2020 May 12;323(18):1843-4.
20. Guo L, Ren L, Yang S, Xiao M, Chang D, Yang F, et al. Profiling early humoral response to diagnose novel coronavirus disease (COVID-19). Clinical Infectious Diseases. 2020 Jul 28;71(15):778-85.
21. Ai T, Yang Z, Hou H, Zhan C, Chen C, Lv W, et al. Correlation of chest CT and RT-PCR testing in coronavirus disease 2019 (COVID-19) in China: a report of 1014 cases. Radiology. 2020 Aug 1.
22. Artik Y, Cesur NP, Laçin NT. SARS-CoV-2 Mutations, Diagnosis and Their Concern. Archives Of Molecular Biology And Genetics. 2022;1(2):57-65.
23. Manski CF, Molinari F. Estimating the COVID-19 infection rate: Anatomy of an inference problem. Journal Of Econometrics. 2021 Jan 1;220(1):181-92.
24. Di Mascio D, Khalil A, Saccone G, Rizzo G, Buca D, Liberati M, et al. Outcome of coronavirus spectrum infections (SARS, MERS, COVID-19) during pregnancy: a systematic review and meta-analysis. American Journal Of Obstetrics & Gynecology MFM. 2020 May 1;2(2):100107.
25. Artik Y, Coşğun AB, Cesur NP, Hızel N, Uyar Y, Sur H, et al. Comparison of COVID‐19 laboratory diagnosis by commercial kits: Effectivity of RT‐PCR to the RT‐LAMP. Journal of Medical Virology. 2022 May;94(5):1998-2007.
26. Komurcu SZ, Artik Y, Cesur NP, Tanriverdi A, Erdogan DC, Celik S, et al. The evaluation of potential global impact of the N501Y mutation in SARS‐COV‐2 positive patients. Journal of Medical Virology. 2022 Mar;94(3):1009-19.
27. Artik Y, Kurtulmus MS, Cesur NP, Komurcu SZ, Kazezoglu C, Kocatas A. Clinic Evaluation of The Destrovir Spray Effectiveness in SARS-CoV-2 Disease. Electronic Journal Of General Medicine. 2022 Apr 1;19(2).
28. Fiore JR, Centra M, De Carlo A, Granato T, Rosa A, Sarno M, et al. Results from a survey in healthy blood donors in South eastern Italy indicate that we are far away from herd immunity to SARS‐CoV‐2. Journal of Medical Virology. 2021 Mar;93(3):1739-42.
29. Kwok KO, Lai F, Wei WI, Wong SY, Tang JW. Herd immunity–estimating the level required to halt the COVID-19 epidemics in affected countries. Journal of Infection. 2020 Jun 1;80(6):e32-3.
30. https://www.who.int/emergencies/diseases/novel-coronavirus-2019
31. https://www.worldometers.info/coronavirus/country/turkey/
32. Mart Komurcu SZ, Artik Y, Uyar Y, Hizel N, Sur H, Kocadag ZA, Dogan S, et al. The effect of q-RT-PCR analysis method on saline gargle samples in SARS-CoV-2 clinical diagnostic methods. ELECTRON J GEN MED. 2022;19 (6):em418.
33. Mart Komurcu SZ, Artik Y, Cesur NP, Kazezoglu C, Sutasir YT. Evaluation of SARS-CoV-2 patients with annual RT-PCR analysis results. Journal of Clinical and Experimental Investigations. 2022;13(4):em00804.
34. Yasamineh S, Kalajahi HG, Yasamineh P, Gholizadeh O, Youshanlouei HR, Matloub SK, et al. Spotlight on therapeutic efficiency of mesenchymal stem cells in viral infections with a focus on COVID-19. Stem Cell Research & Therapy. 2022 Dec;13(1):1-23.
35. Hashemi B, Akram FA, Amirazad H, Dadashpour M, Sheervalilou M, Nasrabadi D, et al. Emerging importance of nanotechnology-based approaches to control the COVID-19 pandemic; focus on nanomedicine iterance in diagnosis and treatment of COVID-19 patients. Journal Of Drug Delivery Science and Technology, 2021 p.102967.
36. Ansart S, Pelat C, Boelle PY, Carrat F, Flahault A, Valleron AJ. Mortality burden of the 1918-1919 influenza pandemic in Europe. Influenza And Other Respiratory Viruses. 2009 May;3(3):99-106.
37. Nicholls H. Pandemic influenza: the inside story. PLoS Biology. 2006 Feb;4(2):e50.
38. Republic of Turkey, Ministry of Health COVID-19 Regulations.
39. Republic of Turkey, Ministry of Interior COVID-19 Regulations.
40. Republic of Turkey, Ministry of Interior COVID-19 Regulations: