Abstract
Background: Lumbar and cervical disc herniations and bulges are common causes of pain and disability, with conservative, non-invasive treatments recommended as first-line interventions. Intervertebral Differential Dynamics (IDD) Therapy is a form of targeted spinal decompression that aims to reduce disc pressure and promote healing. While some studies question the efficacy of traction-based therapies, others suggest potential benefits. This study evaluated the impact of IDD Therapy on pain and functional disability in patients with MRI-confirmed disc pathology.
Methods: A retrospective cohort study was conducted at a single institution on 21 patients (47 disc levels) treated between June 2024 and July 2025. All patients completed 30 sessions of IDD Therapy using the Accu-Spina device. Inclusion criteria required MRI-confirmed lumbar or cervical disc bulges or herniations and complete pre- and post-treatment outcome data. Visual Analog Scale (VAS) and Oswestry Disability Index (ODI) scores were used to assess pain and functional status. Paired t-tests and Cohen’s d were used to analyze treatment effects.
Results: Mean VAS scores decreased from 5.8 to 1.5 (p < .0001; Cohen’s d = 2.16), and ODI scores improved from 18.5 to 6.5 (p < .0001; Cohen’s d = 1.69), indicating large and statistically significant improvements in pain and function. No adverse events were reported.
Conclusion: IDD Therapy was associated with significant short-term reductions in pain and disability among patients with disc bulge or herniation. While these findings are promising, further randomized, controlled trials with larger cohorts and long-term follow-up are warranted.
Keywords
IDD Therapy, Disc Herniation, Disc Bulge, Vertebral Axial Decompression, Clinical Outcomes, VAS, ODI
Introduction
Disc herniations and bulges are highly prevalent, with symptomatic lumbar disc herniation affecting up to 403 million people or 5.5% of the world population and representing a leading cause of disability and healthcare utilization worldwide [1]. Conservative, non-operative treatments – such as physical therapy, NSAIDs, and epidural injections – are widely recommended as the first-line approach for lumbar disc herniation with radiculopathy unless there is evidence of neurological impairment [2].
Traction-based techniques are common, non-invasive options used to treat disc herniations and bulging discs in the spine. Surgical options including spine fusions are associated with increased risk [3,4]. Historically, literature has not been conclusive in showing whether traction-based therapies provide benefit over sham treatment [5,6]. However, several previous studies have demonstrated improvements in pain, function disability, and imaging findings following non-surgical decompression and traction-based intervention for intervertebral disc pathologies [7,8]. More recent investigations revealed potential clinical benefit of targeted decompression therapies in carefully selected patient populations [9,10].
Intervertebral Differential Dynamics (IDD) therapy is one such type of traction therapy that is unique in that it uses different waveforms of decompression to target individual vertebral disc levels so that therapy can be more precisely directed [11]. Waveform characteristics and direction of traction are modified through patient positioning and restraints to target specific levels of the spine without stressing nearby tissues. The waveforms are delivered in a cyclical manner, alternating between high and low tension to selectively unload vertebral discs while minimizing paraspinal muscle guarding [8]. This oscillatory mechanism promotes healing by creating negative pressure in the disc space, allowing for nutrient uptake which enhances tissue healing [12].
The primary objective of this study was to quantify clinical outcomes of patients undergoing IDD therapy with the primary diagnosis of disc bulge or disc herniation. VAS and ODI scores are validated outcome measures widely used in spine research and clinical practice to quantify pain and functional disability, making them appropriate for assessing IDD therapy outcomes [13,14]. Visual analogue scale (VAS) scores and Oswestry Disability Index (ODI) forms from before and after therapy completion were compared to calculate subjective improvement in pain and function. We hypothesized that patients completing a full course of IDD therapy would experience reduction in pain and disability as measured by VAS and ODI scores.
Methods
Study design
An Institutional Review Board-approved retrospective cohort study was conducted on patients who completed the entire IDD Therapy protocol during the period of June 1, 2024, to July 1, 2025. Patients had a primary diagnosis of cervical or lumbar disc bulges or herniations which were verified by MRI prior to the start of treatment. The treatments were conducted at a single institution, Spine Restoration, a private clinic, in Marion, IN. To be included, patients must have had 30 treatments within a 3-month time period as per the inclusion/exclusion criteria, been over 18 years of age, not had previous surgery to the treatment area, and had a primary diagnosis of cervical disc bulge, cervical disc herniation, lumbar disc bulge, or lumbar disc herniation. Exclusion criteria included patients with active malignancy or pregnancy and patients with incomplete VAS and ODI data. A complete list of inclusion and exclusion criteria is displayed in Table 1. During the time indicated, 21 patients met inclusion/exclusion criteria with 47 levels being assessed. Two of the patients had pathology at both lumbar and cervical levels. Treatment protocols were individualized based on each patient’s level and severity of pathology and were conducted in accordance with the IDD Therapy Treatment Protocols developed by C. Norman Shealy, MD, PhD (Appendix 1). Starting tension was calculated utilizing the formulas in the protocols. Patients were reassessed prior to each treatment session by a Doctor of Chiropractic Medicine. Initial distraction forces were determined using the starting tension formulas outlined in Shealy’s protocol. Distraction tension was increased by five pounds for lumbar pathologies and two pounds for cervical pathologies only when post-treatment and inter-treatment visual analogue scale (VAS) scores did not increase and when radicular symptoms demonstrated centralization. Tension was progressively increased throughout the course of care until the target tension defined by Shealy’s protocol was achieved or until symptom resolution occurred. The study was conducted according to the Declaration of Helinski and its subsequent amendments. The study was approved by the Institutional Review Board of Indiana University School of Medicine (No. 24292) and individual consent for the study was waived.
|
Inclusion Criteria |
|
|
|
|
Exclusion Criteria |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Data collection and analysis
VAS and ODI data as well as demographic information was tracked in an electronic medical system. Demographic information is displayed in Table 2. VAS and ODI data were collected prior to the patients’ first treatment session and at the start of each session thereafter. Outcome measures were completed by the patient in a private setting prior to seeing the clinician. Patients recorded their current VAS pain scores, and the ODI was given via the standard, unmodified questionnaire. The outcome measures were written on paper by patients and later transferred to the electronic medical records system by office staff. Blinding of outcome data to the treating clinician was not possible due to scores being critical in distraction tension determination. Again, outcome measures were completed prior to interaction with the clinician.
|
Cohort Characteristics |
N |
Mean ± SD or % |
|
Demographics |
||
|
Age (years) |
21 |
50.8 ± 15.5 |
|
Female (%) |
11 |
52.3 |
|
Treatment Details |
||
|
Treatment Level |
|
|
|
C3–C4 |
3 |
14.3 |
|
C4–C5 |
3 |
14.3 |
|
C5–C6 |
3 |
14.3 |
|
C6–C7 |
4 |
19.0 |
|
L2–L3 |
2 |
9.5 |
|
L3–L4 |
8 |
38.1 |
|
L4–L5 |
14 |
66.7 |
|
L5–S1 |
10 |
47.8 |
|
Levels per Patient |
21 |
2.1 ± 1.4 |
|
Abbreviations: SD, Standard Deviation |
||
Pre-treatment MRIs were completed on each patient to confirm their diagnosis. Post-therapy MRIs were also obtained to monitor for changes in objective findings, results which are planned to be shared in a later publication.
The online calculator Statistics Kingdom was used to carry out all statistical analysis [15]. Paired-samples t-test was used to compare pre-treatment and post-treatment VAS and ODI scores. Effect sizes were calculated using Cohen’s d to evaluate the magnitude of treatment effects. A significance threshold of p <.05 was used for all comparisons.
Bias
Bias was minimized by having the same practitioner complete each therapy session per protocol. Additionally, inclusion and exclusion criteria were arranged to reduce confounding.
Results
A total of 21 patients met inclusion criteria, with 47-disc levels treated due to bulge or herniations. Of these, 34 were lumbar and 13 were cervical pathologies. Two patients underwent therapy for both cervical and lumbar disc disease.
Pain outcomes
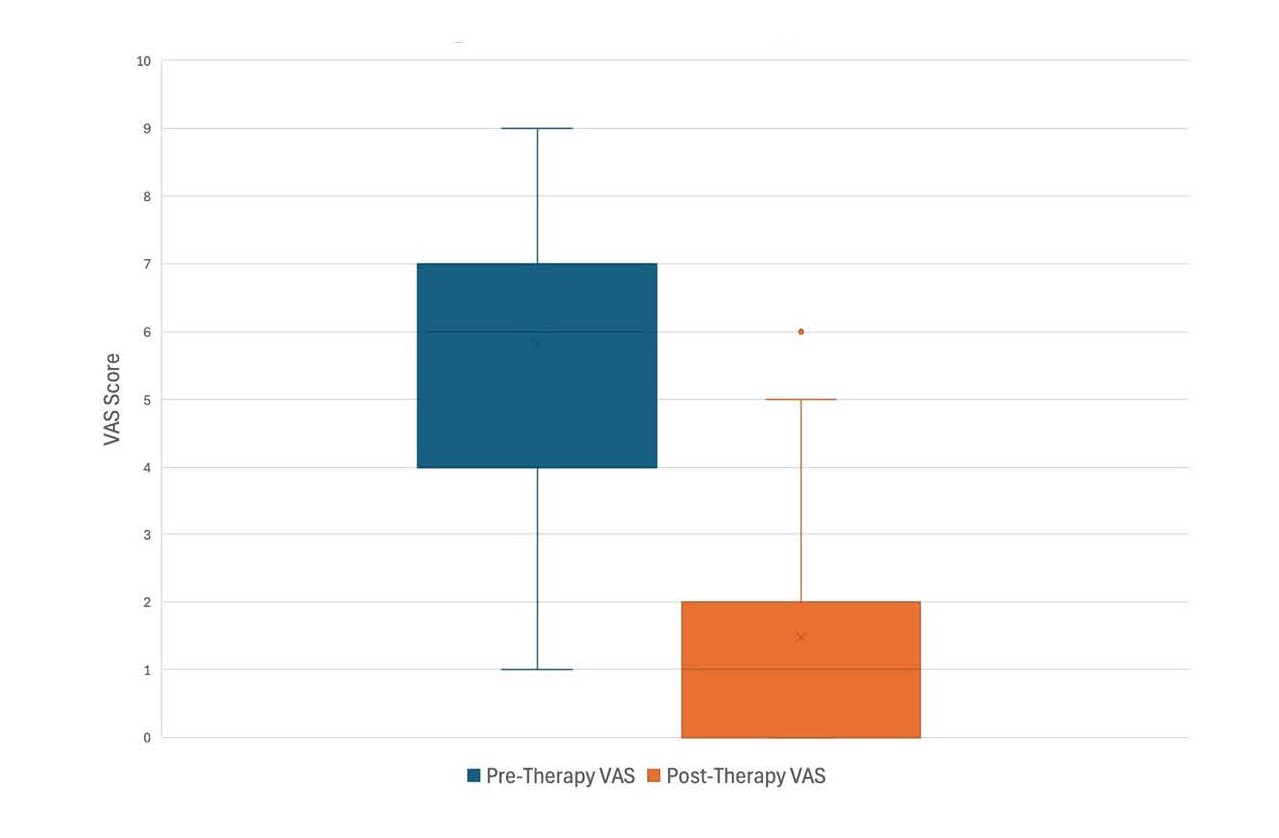
Pre-treatment VAS scores had a mean of 5.8 ± 1.9 and post-treatment scores had a mean of 1.5 ± 1.8. This resulted in a reduction of 4.3 (t21=10.4; p<0.001), with a large effect size (Cohen’s d = 2.16) (Table 3 and Figure 1).
|
Outcome Measure |
Pre-Treatment (Mean ± SD) |
Post-Treatment (Mean ± SD) |
Mean Difference |
t (df) |
p-value |
Cohen’s d |
|
VAS |
5.8 ± 1.9 |
1.5 ± 1.8 |
4.3 |
10.4 (22) |
<0.001 |
2.16 |
|
ODI |
18.5 ± 7.2 |
6.5 ± 6.1 |
12.0 |
8.2 (22) |
<0.001 |
1.69 |
|
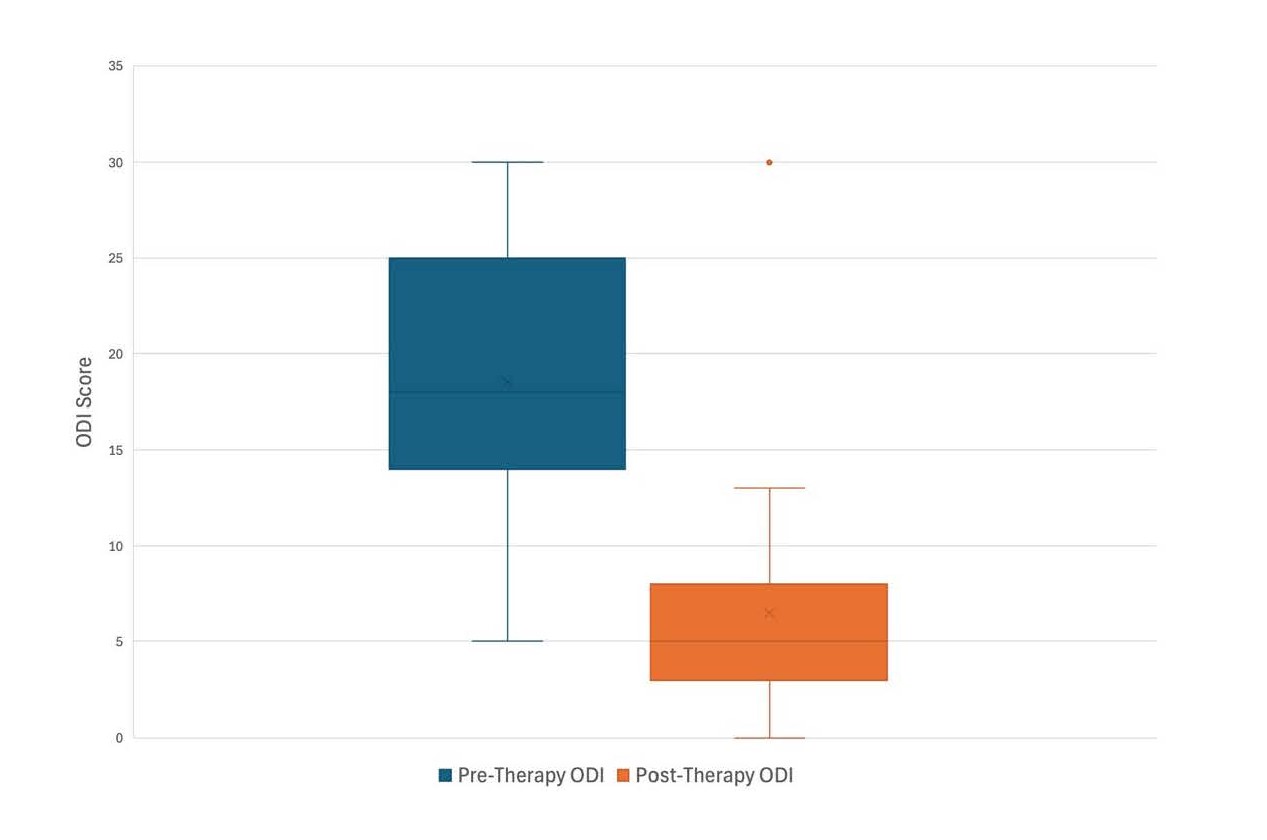
Pre- and post-treatment Visual Analogue Scale (VAS) and Oswestry Disability Index (ODI) scores with statistical analysis. Values are presented as mean ± standard deviation. Paired-samples t-tests demonstrated significant reductions in both pain and disability scores with large effect sizes (Cohen’s d). |
||||||
Pre-treatment cervical VAS scores had a mean of 7.0 and a standard deviation of 1.8, and post-treatment scores had a mean of 2.0 and a standard deviation of 1.4. This reduction was statistically significant with a t statistic of 7.1 and p = .006, indicating a large difference between conditions.
Pre-treatment lumbar VAS scores had a mean of 5.6 and a standard deviation of 1.9, and post-treatment scores had a mean of 1.4 and a standard deviation of 1.9. This reduction was statistically significant with a t statistic of 8.6 and p<.0001, indicating a large difference between conditions.
Functional outcomes
Oswestry Disability Index (ODI) scores improved from a pre-treatment mean of 18.5 ± 7.2 to a post-treatment mean of 6.5 ± 6.1. This resulted in a difference of 12.0 (t22=8.2; p<0.001), with a large effect size (Cohen’s d = 1.69) (Table 3 and Figure 2).
Pre-treatment cervical ODI scores had a mean of 23.3 and a standard deviation of 6.2, and post-treatment scores had a mean of 5.5 and a standard deviation of 3.3. This reduction was statistically significant with a t statistic of 8.8 and p = .003, indicating a large difference between conditions (Table 4).
|
Outcome Measure |
Pre-Treatment (Mean ± SD) |
Post-Treatment (Mean ± SD) |
Mean Difference |
t (df) |
p-value |
|
VAS |
7.0 ± 1.8 |
2.0 ± 1.4 |
5.0 |
7.1 |
0.006 |
|
ODI |
23.3 ± 6.2 |
5.5 ± 3.3 |
17.8 |
8.8 |
0.003 |
|
Pre- and post-treatment Visual Analogue Scale (VAS) and Oswestry Disability Index (ODI) scores with statistical analysis for patients with cervical pathologies. Values are presented as mean ± standard deviation. Paired-samples t-tests demonstrated significant reductions in both pain and disability scores. |
|||||
Pre-treatment lumbar ODI scores had a mean of 17.5 and a standard deviation of 7.1, and post-treatment scores had a mean of 6.7 and a standard deviation of 6.6. This reduction was statistically significant with a t statistic of 6.7 and p<.0001, indicating a large difference between conditions (Table 5).
No adverse events were reported during the treatment period.
|
Outcome Measure |
Pre-Treatment (Mean ± SD) |
Post-Treatment (Mean ± SD) |
Mean Difference |
t (df) |
p-value |
|
VAS |
5.6 ± 1.9 |
1.4 ± 1.9 |
4.2 |
8.6 |
<0.001 |
|
ODI |
27.5 ± 7.1 |
6.7 ± 6.6 |
20.8 |
6.7 |
<0.001 |
|
Pre- and post-treatment Visual Analogue Scale (VAS) and Oswestry Disability Index (ODI) scores with statistical analysis for patients with lumbar pathologies. Values are presented as mean ± standard deviation. Paired-samples t-tests demonstrated significant reductions in both pain and disability scores. |
|||||
Discussion
This retrospective cohort study demonstrated that patients with MRI-confirmed lumbar or cervical disc pathology who completed a full course of IDD Therapy experienced statistically and clinically significant improvements in both pain and function. On average, VAS scores decreased by 4.3 points, while ODI scores decreased by 12.0 points. With both measures having a Cohen’s d value >1.5, effect sizes were large suggesting the observed changes are not only statistically meaningful but also clinically relevant. Importantly, these findings exceed the minimal clinically important difference (MCID) for VAS scores which has been established to be 2.3 points in lumbar pathologies [16]. This indicates that these results are not only statistically significant, but clinically meaningful.
These findings are consistent with prior reports that IDD therapy may provide sustained benefits in patients with disc-related pathology. Shealy et al. [11] reported IDD therapy improved long-term pain scores, with our results reinforcing the potential efficacy of this approach with different pain scoring tools and a narrower patient cohort. However, other studies, such as a randomized controlled trial by Schimmel et al. [6], found no benefit of IDD therapy over sham interventions, especially when paired with a graded exercise program. The discrepancy may reflect differences in patient characteristics, efficacy of the sham intervention, or variations in the specific therapy protocol. Our study, which required completion of all 30 sessions and verified diagnoses with MRI, may have increased uniformity and contributed to more consistent improvements.
The improvements observed in this study are notable when compared to outcomes following surgical interventions. Lumbar fusion, while effective for select patients, carries the risk of complications such as adjacent segment degeneration and need for revision surgery, while in other patients provides no significant improvements in pain or disability related outcomes [1,2]. In contrast, in our patient group, IDD therapy was a well-tolerated, non-invasive therapy with no reported adverse effects. Although long-term durability of outcomes was not assessed here, the immediate reductions in pain and disability suggest that IDD therapy may represent a valuable first-line option for certain patients.
Patients undergoing lumbar and cervical treatments were noted to have similar mean differences in VAS and ODI. Patients with cervical pathologies saw a larger difference in VAS scores (5.0 vs 4.8), while patients with lumbar pathologies had greater improvements in ODI scores (20.8 vs 17.8). Directly comparing lumbar and cervical results were not an objective of this study. There were significantly less patients who underwent cervical treatments as compared to lumbar treatments so a direct comparison would be underpowered and potentially unreliable. Future studies with more even treatment groups would be necessary to draw conclusions between the two.
This study has several limitations. Due to the retrospective design of the study and its lack of randomization, selection bias is a factor. Additionally, the lack of a control group makes it difficult to determine causality. This study also has a relatively small sample size, especially for cervical pathologies, which limits its generalizability. During our analysis, we did not stratify herniation versus bulge pathology due to the limited number of enrolled patients, and future work should explore whether outcomes differ by lesion type. Post-treatment MRI findings, which may provide objective evidence of structural improvement, are being analyzed and will be reported separately. Moreover, patients’ schedules made it difficult to require treatment frequency. Although the patients had to come in 30 times over the span of three months, the variability of the visits could affect the clinical response and outcome of the study by introducing heterogeneity. Further studies should aim to standardize visit frequency.
Future studies should include larger, prospective cohorts with randomization against standard conservative therapy or sham treatment and standardize treatment frequency. Incorporating long-term follow-up would also help determine whether the benefits observed here are durable over time.
Conclusion
This study demonstrates that IDD Therapy significantly reduces pain and disability in patients with MRI-confirmed disc bulges or herniations, offering a non-invasive alternative to surgery with no reported adverse effects. The large effect sizes suggest clinically meaningful benefits, supporting IDD Therapy as a viable conservative treatment option. While further randomized studies are needed, these findings highlight the potential role of targeted decompression therapy in improving outcomes for patients with disc-related spinal conditions.
Conflicts of Interest
The authors have no conflicts of interest to disclose.
Funding Statement
No funding was used for the creation of this study or the writing of the manuscript.
Acknowledgements
None.
References
2. Jin H, Lopez AM, Romero FG, Hoang R, Ramesh A, Bow HC. A Systematic Review of Treatment Guidelines for Lumbar Disc Herniation. Neurospine. 2025 Jun;22(2):389–402.
3. Wang T, Ding W. Risk factors for adjacent segment degeneration after posterior lumbar fusion surgery in treatment for degenerative lumbar disorders: a meta-analysis. J Orthop Surg Res. 2020 Dec 3;15(1):582.
4. Xu W, Ran B, Luo W, Li Z, Gu R. Is Lumbar Fusion Necessary for Chronic Low Back Pain Associated with Degenerative Disk Disease? A Meta-Analysis. World Neurosurg. 2021 Feb;146:298–306.
5. Clarke J, van Tulder M, Blomberg S, de Vet H, van der Heijden G, Bronfort G. Traction for low back pain with or without sciatica: an updated systematic review within the framework of the Cochrane collaboration. Spine (Phila Pa 1976). 2006 Jun 15;31(14):1591–9.
6. Schimmel JJ, de Kleuver M, Horsting PP, Spruit M, Jacobs WC, van Limbeek J. No effect of traction in patients with low back pain: a single centre, single blind, randomized controlled trial of Intervertebral Differential Dynamics Therapy. Eur Spine J. 2009 Dec;18(12):1843–50.
7. Macario A, Richmond C, Auster M, Pergolizzi JV. Treatment of 94 outpatients with chronic discogenic low back pain with the DRX9000: a retrospective chart review. Pain Pract. 2008 Jan-Feb;8(1):11–7.
8. Apfel CC, Cakmakkaya OS, Martin W, Richmond C, Macario A, George E, et al. Restoration of disk height through non-surgical spinal decompression is associated with decreased discogenic low back pain: a retrospective cohort study. BMC Musculoskelet Disord. 2010 Jul 8;11:155.
9. Adar S, Apaydın O, Dündar U, Toktas H, Yesil H, Eroglu S, et al. Comparison of the Effectiveness of Traditional Motorized Traction and Non-surgical Spinal Decompression Therapy Added to Conventional Physiotherapy for Treatment of Chronic Low Back Pain. Cureus. 2024 Sep 17;16(9):e69610.
10. Connolly J, Luginsland L, Welsh S, Bexley JA, Pirone J, Martin WR, et al. Clinical And Imaging Outcomes Of Non-Surgical Spinal Decompression For Lumbar Intervertebral Disc Lesions: A Case Series. J contemp chiropr. 2025;8(1):81–7.
11. Shealy CN, Koladia N, Wesemann MM. Long-term effect analysis of IDD therapy in low back pian: a retrospective clinical pilot study. Am J Pain Manage. 2005;15:93–7.
12. IDD Therapy [cited 2025 September 19]. Available from: https://iddtherapy.com/.
13. Koivunen K, Widbom-Kolhanen S, Pernaa K, Arokoski J, Saltychev M. Reliability and validity of Oswestry Disability Index among patients undergoing lumbar spinal surgery. BMC Surg. 2024 Jan 3;24(1):13.
14. Adhikari P, Çetin E, Çetinkaya M, Nabi V, Yüksel S, Vila Casademunt A, et al. Ability of Visual Analogue Scale to predict Oswestry Disability Index improvement and surgical treatment decision in patients with adult spinal deformity. Brain Spine. 2022 Aug 28;2:100934.
15. Statistics Kingdom. Paired t test calculator - dependent t-test [Internet]. Australia: Statistics Kingdom www.statskingdom.com. Available from: https://www.statskingdom.com/paired-t-test-calculator.html.
16. Sabourin S, Tram J, Sheldon BL, Pilitsis JG. Defining minimal clinically important differences in pain and disability outcomes of patients with chronic pain treated with spinal cord stimulation. J Neurosurg Spine. 2021 Jun 4;35(2):243–50.