Abstract
Three quarters of all medical errors stem from cognitive error, rather than the systemic errors that most efforts address. This narrative/conceptual review posits that many clinicians are not fully aware of or sufficiently focused on the innate cognitive processes our brains use for clinical reasoning. References refer largely to standardized reviews or peer reviewed research: data that exceeds individual experience or opinion. Unsupervised, all humans revert to these ancient methods of estimation that were not selected for modern complex medical decision making. Clinicians must appreciate dual processing theory and the limitations of the various methods of clinical reasoning, in order to maximize our problem-solving skill and find ideal clinical outcomes. Our brains default inversely to more or less complex methods to process the amount of uncertainty they confront. We can utilize the most effective method, abductive reasoning, only by gathering as much data as possible, thereby reducing uncertainty to its lowest levels. Even expert clinicians not giving sufficient attention to reflection and feedback ultimately reinforce their error-laden processes. Overconfidence, intuition, reasoning across scales, and our innate preference for mechanistic explanations over clear outcome data add to cognitive error and diminished outcomes. We must strive to identify our method of reasoning at all times, form new clinical questions to fill information gaps, and utilize impasses as new sources of data to remodel our diagnoses and treatment plans, while developing and adding to our clinical and communication skills. Humbly seeking multilevel feedback, and learning from review of our own work are essential. Only by anticipating, recognizing, and countering these very human errors can we reduce treatment failure and suboptimal outcomes, and increase professional satisfaction.
Introduction
Medical error is most often presumed to result from systemic errors of commission and omission: e.g., interventions on the wrong limb, delivery of the wrong medication, failure to provide an ordered treatment, misinterpretation of orders. The Swiss Cheese Model (Figure 1), for example, is an oft applied method to ensure that redundancy and duplication in a large medical system will ultimately catch every error before it impacts a patient. Medical error, though, most commonly results not from systemic shortcomings, but from individual, very human cognitive mistakes that are unexpected, unrecognized, and therefore persist uncorrected. 75% of all medical errors are cognitive [1,2]. Knowledge of how our brains form concepts, assess, judge, and calculate will aid the medical professional in anticipating, assessing, and correcting the common cognitive errors that so easily derail desirable outcomes for our patients. This commentary offers a narrative/conceptual review of the topic. While such an approach may suffer from selection bias, and the lack of standardized method may make it difficult to reproduce or verify, the references selected refer largely to standardized reviews or peer reviewed research, and data that exceeds individual experience or opinion. The intention is to provide clinicians targeted tools to reduce poor adherence, treatment failure, suboptimal outcomes, and professional dissatisfaction.
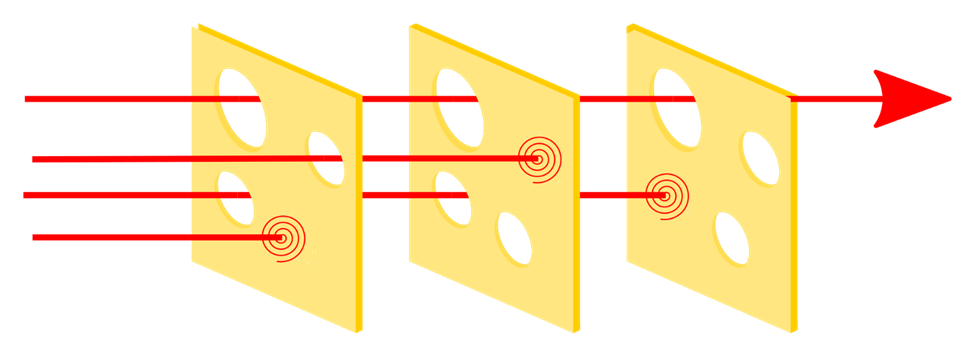
Figure 1. Swiss cheese model of human error trapping. The Swiss Cheese model of human error trapping attempts to block an error in one level of a system by adding safeguards at other levels. In this analogy, an arrow would theoretically not be able to travel through similarly placed holes in each slice of cheese as these would be blocked in at least one slice. The holes are not allowed to remain in the same location throughout the system. In practice, clinicians and administrators identify a shortcoming and install backup systems as multiple layers of defense in an effort to prevent it from affecting final clinical outcomes. Having each staff member confirm a patient’s identity is one example. (By User: Ben Aveling - File:Swiss cheese model.svg, CC BY-SA 4.0, https://commons.wikimedia.org/w/index.php?curid=133912327).
Conceptual Structure and Brain Function
Our brains are not tabula rasae, blank slates upon which experience will write [3]. Rather, the study of language acquisition indicates that innate cognitive structures exist in our brains, composed of neural assemblages that that “learn” and create meaning as they fit to our experiences [4,5]. Events, i.e. episodic memories, are stored in the neocortex; when called upon, the hippocampus constructs and reconstructs a sequential order of these events for us to “recall” utilizing time and place cells [6]. Repetitive experiences of episodic memory, each recreated “anew” and more often influenced by significance, inference, and experience than original content and order, become “facts” for us. In other words, our memories are not fixed copies from an internal hard drive, but variable as they are irretrievably linked with imagination and social exigency [7]. As a result, our memories of “facts” have more coherence than correspondence, fitting with our concepts and images of ourselves more than accurately matching original events [8].
The data we gather from patients is manipulated into concepts we utilize to make judgements and predictions. Due to the “cognitive miser function,” however, our brains exert the least cognitive effort possible to form these and solve problems [9]. Shortcut estimates, called heuristics [10], are automatically applied to project probable scenarios into the future. We remember these concepts, such as diagnoses, rather than raw data or events, so they are not often consciously confirmed [11]. Once a diagnosis has been made, we ignore symptoms that do not fit and “recall” ones that did not actually exist [12,13].
Dual Processing Theory
Popularized as fast (Type I) and slow (Type II) thinking, we can apply two types of cognitive processing to problem solving. Type I results from the innate cognitive mechanisms described above. It is ancient and may have evolved to help homo sapiens remove ourselves from danger and socialize, thus enhancing gene propagation [14]. Utilizing judgment based entirely on individual experience [15], this form of cognitive processing was not selected to solve the complex medical dilemmas we face today.
Type II has been developed through cultural, not biological evolution, and encompasses the scientific method: representing underlying principles, utilizing logic and providing abstract reasoning and hypothetical thinking. It calculates rather than estimates, considering the pooled experience of humankind (i.e., statistics) [9,14,16,17].
These two systems compete to control inference and our actions. While they may provide a check on each other’s conclusions (e.g., ruling out an impossible body weight or lifespan calculation) [18], conscious use of Type II processing can temporarily suppress, but never eliminate, Type I conclusions [14,16]. As we humans have less capacity to utilize Type II, even the most intelligent, educated, and experienced clinicians most commonly default to Type I [9,19].
Type I processing often provides quicker answers, unless repetitively used Type II methods become encoded as Type I perceptual chunks, a process our brains use to extend their limited processing ability beyond serial attention [20]. Type I processing, unchecked by Type II, also results in a far greater number of cognitive errors [9]. The more trusted Type II, though, must rely on accurate data and validated methods or risk resulting in more serious consequences [18].
Success in modern medical practice requires analysis of decontextualized data, which Type I did not evolve to interpret: numerically presented information which exceeds the experience of a single provider [15]. Type II processing is required to manage this probabilistic information displayed in non-frequentist terms, e.g., making the best decisions about diagnosis and treatment selection, initially and over time [14].
Ambiguity and Uncertainty
Ambiguity, the multiple possible states of an event or medical presentation, is inherent in medicine; uncertainty, therefore can never be eliminated in clinical situations or decisions. Clinicians, as a group, however, discount unspecified probabilities and avoid both acknowledging and sharing our uncertainty, further increasing our cognitive error [21]. In all cases we must consider not only the amount of ambiguity in each case, but also our degree of awareness of our uncertainty in order to choose and employ the most error-free method of clinical reasoning [22,23].
When we face a high level of uncertainty about a diagnosis or effective treatment plan, our minds default to eristic reasoning. Hedonistic urges, including wishful thinking, loss aversion, a preference for the status quo, overconfidence, and the endowment effect (subjectively valuing our own possessions or ideas more highly than their objective worth), will direct our judgement and conclusions [24–27]. Ironically, in the absence of sufficient data to utilize higher level reasoning, this approach is even considered logical, as we have little else to guide us.
When we confront a case with moderate uncertainty, we unconsciously rely on heuristics, in-bred estimations linked to Type I reasoning. Again, these may well be faulty predictions as they rely solely on individual (and usually recent) experience without considering broader data. As only one example of these many shortcuts, when one patient has symptoms similar to another’s, the representativeness heuristic [28] leads us to quickly apply the same diagnosis to both cases, inadequately considering a full differential diagnosis.
When we gather enough data to proceed with low uncertainty, we can then utilize the most effective method of clinical reasoning: abductive. This approach forms a hypothesis, tests it, then reformulates the original hypothesis in light of the information gathered from the test (e.g., treatment failure, new laboratory or physical data, poor treatment tolerance). This remodeling is key to preventing us from persisting with a diagnosis that defies response to our treatments. As Box and Draper wisely inform us “Essentially, all models are wrong, but some are useful…The practical question is how wrong do they have to be to not be useful” [29].
We can become more aware of which method of reasoning we have automatically turned to: eristic methods may be identified by what are usually considered non-logical approaches (e.g., beliefs, strong emotions, economic gain, prejudice); heuristics through cues (e.g., analogy, past performance), truth seeking attempts, and notable consideration of outcome consequence; and abductive reasoning by our utilization of broad data and stochastic, analytic methods, employing a creative, iterative hypothesis competition [27,30].
Changes in Medical Reasoning Across a Career
Medical practitioners often attempt various forms of reasoning as our careers evolve. Early on, we often struggle with hypothetical-deductive and inductive reasoning, finding it hard to form adequate hypotheses and to account for negative data. We also struggle to actively suppress incorrect information we learned alongside the correct [31–33]. After around six years of practice, we evolve into expert mode, utilizing illness scripts which link the conditions for a disorder (e.g., age, lifestyle, heredity, medical history, etc.) to the consequences of that illness (e.g., symptoms or functionality and their clinical course) [34,35].
The change unfortunately also represents a return to Type I pattern matching, in which unstructured, random, and atypical case information is poorly remembered. This reinforces a narrowing of our focus and promotion of confirmation bias – “seeing” mostly what we have seen before and expect to see again. Additionally, we develop a harmful bias towards positive feedback on our professional performance [36]. As a result, “expert” clinicians are as likely to make cognitive errors as more inexperienced practitioners [13,37,38]. While clinical experience can add to the reasoning powers of medical providers, without awareness of these processes, conscious reflection, and feedback it reinforces conceptual error and lowers our clinical performance [20].
Common Sources of Error
Overconfidence is a risk in all professions. In medicine, particularly, we overestimate our abilities and suppress awareness of our errors, leading to incomplete evaluations, fewer requests for consultation, and unrealistic acceptance of lower complexity thinking [39]. Errors often result from employing simpler, rather than more complex cognitive strategies [40]. In fact, our clinical encounters have become even more complex during the past few decades: more treatments have become available and medical comorbidities have increased as many patients live longer lives [41].
Intuition is commonly involved in expert decision making, as feelings become integrated into illness-scripts [42]. Decisions based on intuition carry a strong emotional impact for the clinician and easily compete with choices that rely less on it [43]; when intuitive answers come to us easily, this unfortunately bolsters overconfidence in our decisions [44]. Such bias gives providers a more personal sense of involvement than Type II processing might, resulting in more positive feelings when an intuitive choice is correct, than when a non-intuitive choice is confirmed [43]. As a group, we make diagnoses too quickly and then cherry-pick data to fit our initial impressions, instead of seeking explanations for the complete results of broad and thorough assessments.
Further, we prefer and usually restrict ourselves to observable scales in creating and employing our clinical narratives. This leads to error as we fail to allow for emergent properties (those that cannot be explained by lower levels of complexity; e.g., “life” from chemistry, or “mind” from neurons). We particularly exhibit this bias when we choose to follow presumed or even theoretical mechanistic explanations of disease, illness, and therapeutics over clear and undeniable outcome data [45,46]. We cannot predict response to an intervention based on its structure or plausibility, but only on demonstration of its clinical efficacy.
Methods That Reduce Cognitive Error
We will never be free from cognitive error, nor from uncertainty. With effort, though, we can reduce the impact of overconfidence and, conversely, indecision in our clinical problem solving [47,48]. Uncertainty is distinct from indecision – the former is inevitable, the latter misleading and harmful to patients. To strike the right cognitive balance, we must always identify the method of reasoning we are using, make sure it fits the amount of data we have, and always work to increase our volume of information so that we can eventually and effectively utilize abductive reasoning.
We must identify gaps in our data – in our own knowledge base, as well as in the clinical information we obtain from and about patients. We must help patients learn to be searchers alongside us, as we both try to find answers to well-framed, yet still outstanding, clinical questions. Improving our communications skills leads to enhanced adherence and outcomes [49,50]. We must be able to explain our uncertainty, while providing a well-reasoned method for reducing it. We need to take time to review our records of past and current cases, identifying mistakes, successful approaches, and developing new insights we can apply. We must utilize feedback from others: patients, staff, and peers, alike, by listening and asking for it. We must complete full semi-structured assessments at each patient contact in an effort to identify all comorbidities that so often derail full clinical responses, especially with long-term patients. Templates are often helpful. We must then preserve and account for all of our data. Electronic medical records make it too easy to copy previously obtained data; we must record all the details of new, thorough assessments at each visit in order to find the answers to ambiguous presentations, treatment failures, and suboptimal outcomes.
It is essential to adopt humility, recognizing and responding positively to clinical impasses, as new data from our iterative hypothesis competition help us remodel our clinical understanding of patients’ situations. We must avoid rapid diagnosis whenever it is safe and reasonably possible, always developing a meaningful and useful differential diagnosis, and routinely make time for review and reflection. Whenever possible, we need to develop and add to our clinical skills, as we seldom recommend treatments we cannot provide, and may not adequately consider diagnoses that require them [51].
|
|
|
|
|
|
|
|
Conclusion
Unrecognized suboptimal cognitive acts lead to faults in diagnostic reasoning and mistakes, resulting in increased patient harm [52]. Treatment failure, failure to treat, and acceptance of suboptimal outcomes worsen prognosis, morbidity, and mortality. Our cognitive errors may result from knowledge gaps, faulty data gathering, or incorrect information processing [53]. We must improve our quality of care by learning our brains’ default functions when not guided by conscious oversight: the innate mechanisms that distort our assessments and conclusions and misdirect the care we intend to provide. Given the high degree of cognitive error in our field, this is an ethical imperative. Research shows that application of the insights and methods described above results in better clinical outcomes and professional satisfaction. Future research to quantify the effect of each technique on treatment success may provide even greater motivation and justification for adoption by students and practicing clinicians.
References
2. O'Sullivan ED, Schofield SJ. Cognitive bias in clinical medicine. J R Coll Physicians Edinb. 2018 Sep;48(3):225–32.
3. Pinker S. The Blank Slate: The Modern Denial of Human Nature. New York: Viking; 2002.
4. Pinker S: The Stuff of Though: Language as a Window into Human Nature. New York: Penguin Group (USA) Inc., 2007. pp. 153–233.
5. Steven Pinker. Language as a Window into Conceptual Structure [Video]. Lecture given during The Shalem Center’s Psycho-ontology Conference; December 2011. Published July 25, 2012. Accessed June 7, 2022. Available from: https://www.youtube.com/watch?v=d02BbdFZJrs
6. Lisman J, Buzsáki G, Eichenbaum H, Nadel L, Ranganath C, Redish AD. Viewpoints: how the hippocampus contributes to memory, navigation and cognition. Nat Neurosci. 2017 Oct 26;20(11):1434–47.
7. Moscovitch M. Memory and Working-with-Memory: A Component Process Model Based on Modules and Central Systems. J Cogn Neurosci. 1992 Summer;4(3):257–67.
8. Conway MA. Memory and the self. J Mem Lang. 2005;53(4):594–628.
9. Croskerry P. Clinical cognition and diagnostic error: applications of a dual process model of reasoning. Adv Health Sci Educ Theory Pract. 2009 Sep;14 Suppl 1:27–35.
10. Hjeij M, Vilks A. A brief history of heuristics: how did research on heuristics evolve?. Humanit Soc Sci Commun. 2023 Feb 17;10(1):64.
11. Van den Bergh O, Walentynowicz M. Accuracy and bias in retrospective symptom reporting. Curr Opin Psychiatry. 2016 Sep;29(5):302–8.
12. Arkes HR, Harkness AR. Effect of making a diagnosis on subsequent recognition of symptoms. J Exp Psychol Hum Learn. 1980 Sep;6(5):568–75.
13. Boshuizen HP, Gruber H, Strasser J. Knowledge restructuring through case processing: The key to generalise expertise development theory across domains?. Educ Res Rev. 2020 Feb 1;29:100310.
14. Stanovich KE. Who Is Rational? Studies of Individual Differences in Reasoning. Mahwah, NJ: Lawrence Erlbaum Associates; 1999.
15. Cosmides L, Tooby J. Are humans good intuitive statisticians after all? Rethinking some conclusions from the literature on judgment under uncertainty. cognition. 1996 Jan 1;58(1):1–73.
16. Evans JS. In two minds: dual-process accounts of reasoning. Trends Cogn Sci. 2003 Oct;7(10):454–9.
17. Sloman SA. The empirical case for two systems of reasoning. Psychol Bull. 1996 Jan;119(1):3.
18. Sundh J, Collsiöö A, Millroth P, Juslin P. Precise/not precise (PNP): A Brunswikian model that uses judgment error distributions to identify cognitive processes. Psychon Bull Rev. 2021 Apr;28(2):351–73.
19. Evans JSBT, Over DE. Rationality and Reasoning. London: Psychology Press/Taylor & Francis Group; 1996.
20. Tay SW, Ryan P, Ryan CA. Systems 1 and 2 thinking processes and cognitive reflection testing in medical students. Can Med Educ J. 2016 Oct 18;7(2):e97–103.
21. Redelmeier DA, Koehler DJ, Liberman V, Tversky A. Probability judgement in medicine: discounting unspecified possibilities. Med Decis Making. 1995 Jul-Sep;15(3):227–30.
22. Cioffi J. Situating uncertainty in clinical decision making. Academia Letters. 2021;3641.
23. Putman HP. Thinking Again: Reducing Cognitive Errors in Psychiatric Practice. 1st ed. Washington, DC: American Psychiatric Association Publishing; 2025. p. 112–4, 180–2.
24. Berthet V. The Impact of Cognitive Biases on Professionals' Decision-Making: A Review of Four Occupational Areas. Front Psychol. 2022 Jan 4;12:802439.
25. Gunaydin G, Selcuk E, Yilmaz C, Hazan C. I Have, Therefore I Love: Status Quo Preference in Mate Choice. Pers Soc Psychol Bull. 2018 Apr;44(4):589–600.
26. Kahneman D, Knetsch JL, Thaler RH. Anomalies: The endowment effect, loss aversion, and status quo bias. Journal of Economic perspectives. 1991 Feb 1;5(1):193–206.
27. Kurdoglu RS, Jekel M, Ateş NY. Eristic reasoning: Adaptation to extreme uncertainty. Front Psychol. 2023 Feb 9;14:1004031.
28. Tversky A, Kahneman D. Judgment under Uncertainty: Heuristics and Biases. Science. 1974 Sep 27;185(4157):1124–31.
29. Box GPE, Draper NR. Empirical Model-Building and Response Surfaces. 1st ed. New York: Wiley; 1987. p. 71.
30. Kurdoglu RS, Ates NY, Lerner DA. Decision-making under extreme uncertainty: eristic rather than heuristic. Int J Entrep Behav Res. 2023 Mar 31;29(3):763–82.
31. Badenhorst E, Mamede S, Hartman N, Schmidt HG. Exploring lecturers' views of first-year health science students' misconceptions in biomedical domains. Adv Health Sci Educ Theory Pract. 2015 May;20(2):403–20.
32. Foisy LM, Potvin P, Riopel M, Masson S. Is inhibition involved in overcoming a common physics misconception in mechanics?. Trends Neurosci Educ. 2015 Mar 1;4(1-2):26–36.
33. Shtulman A, Valcarcel J. Scientific knowledge suppresses but does not supplant earlier intuitions. Cognition. 2012 Aug;124(2):209–15.
34. Einhorn HJ. Expert judgment: Some necessary conditions and an example. J Appl Psychol. 1974 Oct;59(5):562.
35. Guida A, Gobet F, Tardieu H, Nicolas S. How chunks, long-term working memory and templates offer a cognitive explanation for neuroimaging data on expertise acquisition: a two-stage framework. Brain Cogn. 2012 Aug;79(3):221–44.
36. Trapp S, Guitart-Masip M, Schröger E. A link between age, affect, and predictions? Eur J Ageing. 2022 Jul 5;19(4):945–52.
37. Frensch PA, Sternberg RJ. Expertise and intelligent thinking: when is it worse to know better? In: Sternberg RJ, editor. Advances in the Psychology of Human Intelligence. Vol 5. Mahwah, NJ: Lawrence Erlbaum Associates; 1989. p. 157–89.
38. Sternberg RJ, Frensch PA. On being an expert: a cost-benefit analysis. In: Hoffman RR, editor. The Psychology of Expertise: Cognitive Research and Empirical AI. London: Taylor & Francis; 1992. p. 191–203.
39. Cassam Q. Diagnostic error, overconfidence and self-knowledge. Palgrave Communications. 2017 Apr 11;3(1):17025.
40. Elstein AS, Schwartz A. Clinical problem solving and diagnostic decision making: selective review of the cognitive literature. BMJ. 2002 Mar 23;324(7339):729-32.
41. Lenze EJ. Managing Older Adults with Mental Illness [Lecture]. Geriatric Research Award Lecture presented at: American College of Psychiatrists Annual Meeting; 2024 Feb 24; New Orleans, LA.
42. Chassy P, Lahaye R, Didierjean A, Gobet F. Intuition in chess: a study with world-class players. Psychol Res. 2023 Nov;87(8):2380–9.
43. Kirkebøen G, Nordbye GHH. Intuitive Choices Lead to Intensified Positive Emotions: An Overlooked Reason for "Intuition Bias"? Front Psychol. 2017 Nov 7;8:1942.
44. Simmons JP, Nelson LD. Intuitive confidence: choosing between intuitive and nonintuitive alternatives. J Exp Psychol Gen. 2006 Aug;135(3):409–28.
45. Claridge JA, Fabian TC. History and development of evidence-based medicine. World J Surg. 2005 May;29(5):547–53.
46. Lombrozo T. Simplicity and probability in causal explanation. Cogn Psychol. 2007 Nov;55(3):232–57.
47. Lam JA, Feller E. Are We Right When We're Certain? Overconfidence in Medicine. R I Med J (2013). 2020 Mar 2;103(2):11–2.
48. Seidl E, Seidl O. Do my feelings fit the diagnosis? Avoiding misdiagnoses in psychosomatic consultation services. J Healthc Risk Manag. 2021 Oct;41(2):9–17.
49. Ranjan P, Kumari A, Chakrawarty A. How can Doctors Improve their Communication Skills? J Clin Diagn Res. 2015 Mar;9(3):JE01–4.
50. Stewart MA. Effective physician-patient communication and health outcomes: a review. CMAJ. 1995 May 1;152(9):1423–33.
51. Penner JC, Schuwirth L, Durning SJ. From Noise to Music: Reframing the Role of Context in Clinical Reasoning. J Gen Intern Med. 2024 Apr;39(5):851–7.
52. Zwaan L, Thijs A, Wagner C, van der Wal G, Timmermans DR. Relating faults in diagnostic reasoning with diagnostic errors and patient harm. Acad Med. 2012 Feb;87(2):149–56.
53. Duong QH, Pham TN, Reynolds L, Yeap Y, Walker S, Lyons K. A scoping review of therapeutic reasoning process research. Adv Health Sci Educ Theory Pract. 2023 Oct;28(4):1289–310.