Abstract
Parkinson's disease (PD) is a neurodegenerative disorder involving motor and non-motor symptoms that reduce quality of life. Non-motor symptoms, including depression, anxiety, fatigue, and sleep disturbances, are often underrecognized despite their significant impact on daily functioning. This study aimed to examine the effects of three group-based rehabilitation interventions on emotional well-being in patients with moderate PD.
Forty-eight participants (Hoehn-Yahr stages 2.0–3.0) were randomly assigned to music therapy, dance training, physiotherapy, or control groups. Emotional states were assessed using the Emotional State Questionnaire (EST-Q2) before and after an eight-week intervention consisting of twice-weekly 60-minute sessions. Data were analyzed using paired t-tests and one-way ANOVA.
Music therapy demonstrated the broadest benefits, improving depression, anxiety, panic disorder, social phobia, and insomnia. Physiotherapy was most effective in reducing anxiety, asthenia, and insomnia, while dance training improved depression, asthenia, and insomnia. Group-based rehabilitation represents an effective complementary approach for alleviating emotional symptoms in patients with PD.
Keywords
Parkinson’s Disease, Emotional State, Music Therapy, Physiotherapy, Dance
Introduction
Parkinson's Disease (PD) is a progressive neurodegenerative disorder characterized by diverse motor and non-motor symptoms that significantly impact patients' quality of life [1,2]. While clinical practice traditionally focuses on cardinal motor symptoms — bradykinesia, rigidity, tremor, and postural instability [3–6] — the disease encompasses a considerably broader spectrum of manifestations. Non-motor symptoms, including cognitive impairments, mood disorders (particularly depression and anxiety), sleep disturbances, autonomic dysfunction, and sensory anomalies, can be equally debilitating yet often remain underrecognized and inadequately managed in clinical settings [7–9].
Research indicates that quality of life in PD is more significantly influenced by psychological factors related to coping with disease and disability than by illness severity itself [10–12]. Among non-motor symptoms, depression and anxiety have been most extensively studied [13]. Depressive disorders may affect up to 30.7% of PD patients [14], while fatigue is reported in 58% and chronic insomnia in 38% [15]. Motor symptoms such as tremors and dyskinesia demonstrate a bidirectional relationship with sleep disturbances, affecting both sleep duration and quality [16]. Anxiety disorders are reported to be even more prevalent than depression in PD, yet they frequently remain undiagnosed [17,18]. This underdiagnosis is partly attributed to PD-specific anxiety manifestations, which present with complex and heterogeneous symptomatology that often deviates from standard diagnostic criteria [19]. Among PD patients, 13.8% experience social phobia and 6.8% manifest panic disorder with or without phobia [20], while more recent studies suggest panic disorders may affect approximately 10–20% of patients [7,21], indicating a potential increase in recognition or diagnosis of these conditions.
The relationship between motor and non-motor symptoms in PD represents a complex, interdependent system. These symptoms interact in a bidirectional manner, creating a progressive cycle that significantly deteriorates patients' quality of life [22,23]. Depression and anxiety can diminish motivation and physical activity levels, subsequently exacerbating motor symptoms [24,25], while severe motor disorders in turn often lead to social isolation and increased emotional distress [26,27]. This intricate interplay underscores the necessity for comprehensive treatment approaches that simultaneously address both motor and non-motor manifestations.
Pharmacological interventions — including antidepressants and anxiolytics — remain the conventional approach to managing non-motor symptoms in PD. However, these treatments present significant limitations: long-term use can result in drug resistance, and antidepressant therapy often produces adverse effects while inadequately supporting daily functioning as the disease progresses [28,29]. These limitations have prompted growing research interest in non-pharmacological interventions as complementary or alternative strategies [30–32].
Non-pharmacological interventions, including physical exercise, music therapy, dance-based interventions, and cognitive-behavioral therapy, have shown promising effects on both motor and non-motor symptoms in PD patients [33,34]. Cognitive-behavioral therapy has demonstrated positive effects in reducing depression and significantly improving anxiety symptoms and motor functions [35,36]. Commonly utilized approaches also include physiotherapy, occupational therapy, speech therapy, and various forms of psychotherapy such as group psychotherapy and psychodrama [37]. Tailored physical activity has been shown to reduce stress and enhance quality of life [38], while rhythmic auditory stimulation is emerging as a potentially effective intervention for depression in PD [39]. Other non-pharmacological approaches — including acupuncture, hydrotherapy, and massage therapy — have shown potential benefits for pain and apathy [40,41].
Among these interventions, music therapy and physiotherapy have each attracted substantial research attention in PD. Music therapy facilitates movement, improves balance, gait, and quality of daily activities, and enhances cognitive abilities, mood, and motivation [42–45]. Physiotherapy similarly addresses both functional and emotional aspects of the disease, with tailored exercise programs demonstrating measurable gains in well-being [38]. Structured dance-based interventions have also gained considerable attention and have demonstrated benefits across both motor and non-motor domains, including mood, anxiety, depression, and overall quality of life [46]. The social and rhythmic dimensions of group dance are thought to contribute particularly to emotional well-being. Among the formats studied, Argentine tango has received the most extensive research attention and has shown efficacy for both motor and affective outcomes [47], though a growing body of work points to the potential of other formats as well.
It is important to note that the term "dance therapy" is used variably in the literature. In its strict sense, it refers to dance/movement therapy — a recognized psychotherapeutic discipline — but the term has also been widely applied to structured dance-based health interventions that do not conform to this clinical definition [48,49]. The present study uses the term dance training to clearly distinguish its intervention from clinical dance/movement therapy. The intervention draws on local folklore dance — a culturally familiar, accessible, and socially engaging movement form. Shared cultural familiarity may lower participation barriers, reinforce group cohesion, and enhance motivation, all of which could augment the therapeutic impact on emotional well-being.
Despite the promise of these individual approaches, significant gaps remain in our understanding of their effects on the emotional well-being of PD patients, particularly in group-based settings. Evidence regarding the effects of exercise on non-motor disorders and depressive symptoms remains controversial [50]. Most studies have focused on individual rather than group-based therapies, which provide additional social support and shared experiences that may independently enhance emotional outcomes [51]. Furthermore, therapeutic intervention research has predominantly concentrated on the motor aspects of PD [52], and the comparative efficacy of different group-based non-pharmacological interventions on emotional states has not been systematically evaluated.
This study addresses this research gap by investigating the effects of three group-based therapeutic interventions — music therapy, physiotherapy, and simplified dance training — on emotional states in individuals with moderate Parkinson's disease. We hypothesize that these interventions will demonstrate differential yet significant improvements across various emotional states, with the group setting providing synergistic benefits that amplify their individual therapeutic impact.
Material and Methods
Subjects
The study involved 64 Parkinson's Disease (PD) patients classified as Hoehn-Yahr stage 2.0–3.0 (moderate severity) recruited from the AS Confido Medical Center database. Potential participants were identified and invited to participate by a neurologist. Sixty individuals underwent a screening visit and met the following inclusion criteria: a diagnosis of clinically established PD according to the Movement Disorder Society (MDS) clinical diagnostic criteria. Following eligibility screening, participants were randomly assigned to intervention and control groups using a computer-generated randomization procedure implemented with the RAND function in Microsoft Excel.
A psychologist previously assessed the patients' cognitive abilities at the time of their entry into the study. All participants demonstrated the capacity to provide informed consent.
Clinical assessment
Participant eligibility was determined through a comprehensive neurological assessment. Disease severity was evaluated using the Hoehn and Yahr Scale (HY). Clinical evaluation included demographic data collection, disease history, current status, and detailed medication documentation.
All participants maintained their established medication regimens throughout the study period under the supervision of a single neurologist. Participants had no prior exposure to the study's therapeutic interventions. Assessments were conducted during the "ON" medication state at baseline and post-intervention. No changes were made to the medication intervention during the study for those recruited.
The study was approved by the Human Research Ethics Committee of the National Institute for Health Development of Estonia on June 16, 2022 (Approval No. 1100) and was conducted in accordance with the Declaration of Helsinki. The study was registered in the World Health Organization International Clinical Trials Registry Platform (Registration No. DRKS00039213). All participants provided written informed consent. Table 1 provides an overview of the participants' baseline characteristics.
|
Sample =48 |
Mean |
Median |
SD |
Minimum |
Maximum |
|
Height (cm) |
171.4 |
171.5 |
9.7 |
150 |
186 |
|
Weight (kg) |
76.5 |
75.1 |
15.4 |
50.0 |
123.5 |
|
Age 1 (yrs) |
68.6 |
71.0 |
10.2 |
48 |
87 |
|
Age 2 (yrs) |
64.0 |
67.0 |
10.3 |
42 |
81 |
|
Duration of illness (yrs) |
4.7 |
5.0 |
2.6 |
1 |
11 |
|
Hoehn ja Yahr |
2.3 |
2.5 |
0.4 |
2.0 |
3.0 |
|
LDDD |
414.2 |
400.0 |
170.2 |
100 |
880 |
|
Age 1: Age at inclusion in the study; Age 2: Age at diagnosis of Parkinson's; LDD: Levodopa dose at the time of the study. |
|||||
Assessment of emotional state
Data on emotional well-being were collected during a medical visit, alongside general information, both before and after the therapeutic intervention.
The Emotional State Questionnaire (EST-Q2), a validated and developed instrument in Estonia [53] was used for the assessment. This questionnaire includes the following subscales: depression (number of items = 8; score >11), generalized anxiety (number of items = 6; score >11), agoraphobia-panic (number of items = 5; score >6), social phobia (number of items = 2; score >3), asthenia (number of items = 4; score >6) and insomnia (number of items =3; score >5). These subscales reflect symptoms of depressive and anxiety disorders following ICD-10 and DSM-IV criteria. Additionally, they reflect general health problems arising from emotional states, not limited to specific mental health issues. Participants rated the frequency of these emotional state problems over the past four weeks using the following scale: 0 = not at all; 1 = rarely; 2 = sometimes; 3 = often; 4 = all the time. It is important to note that the EST-Q2 is not a diagnostic tool for mental disorders; rather, it helps identify symptoms that may indicate mental health problems or reflect general emotional stress. The EST-Q2 is considered suitable for screening the prevalence of depression and anxiety.
Therapeutic intervention procedures
Following initial testing, participants proceeded to their allocated intervention groups. The intervention groups included physiotherapy, music therapy, and dance training. All interventions were conducted twice weekly for 60-minute sessions over 8 weeks and were delivered by certified professionals with relevant clinical experience in their respective fields. The physiotherapist held a relevant degree and postgraduate qualification in neurological rehabilitation, with nearly 20 years of clinical experience in Parkinson's disease rehabilitation. The music therapist held a doctoral degree in music therapy and a Level 7 certification, with over 30 years of clinical practice experience. The dance training was led by a professional choreographer and folk dance educator with over a decade of academic teaching experience and recognized expertise in folk dance and with over 30 years of practice experience. Participants in the control group continued with their usual care without additional intervention. All intervention sessions were conducted by the same professionals, ensuring consistent delivery of the intervention in terms of session structure, exercise progression, and participant guidance. Participants in the control group continued with their usual care without additional intervention.
Music therapy
Music therapy uses evidence-based techniques, including neurological music therapy [54] and receptive relaxation methods [55], to achieve therapeutic goals in structured sessions. The session starts with a warm-up to establish a welcoming environment, followed by self-assessment scales to tailor the therapy. Physiological training includes Therapeutic Instrumental Music Performance (TIMP) to improve motor control and Patterned Sensory Enhancement (PSE) to guide movements using rhythmic and melodic elements.
Voice exercises, such as Therapeutic Singing (TS) and Vocal Intonation Therapy (VIT), enhance speech, articulation, and respiratory function through singing activities.
Cognitive training involves Musical Attention Control Training (MACT) to improve focus and Musical Executive Function Training (MEFT) to develop planning, memory, and problem-solving through structured musical tasks. The session ends with receptive relaxation techniques, followed by a final self-assessment and summary to consolidate progress.
Physiotherapy
Physiotherapy sessions focused on balance and breathing exercises. The intervention activities were selected based on the intervention components most frequently reported in the literature on balance and gait rehabilitation in individuals with Parkinson’s disease, ensuring consistency with previously established rehabilitation approaches [56–59].
Each session lasted 60 minutes and was structured into a warm-up (5 min), a main training phase (50 min), and a cool-down (5 min). The session commenced with general balance and coordination exercises. Each exercise was performed for 10 repetitions to support consistency and facilitate recall. Repetitions were counted aloud by the instructor. Exercises were initially performed at a comfortable pace, followed by a second set at an increased tempo to introduce progressive loading. Balance exercises incorporating vestibular system activation were then performed, including head movements with eyes open and closed. Exercise difficulty was adapted through multiple variations to accommodate individual differences in physical capacity.
Additional balance exercises emphasized movement accuracy and rhythmic control. The session concluded with breathing exercises combined with low-intensity whole-body movements to support relaxation and recovery.
Dance training
Dance training sessions focused on basic and simpler movements of Estonian folk and social dances. Given the long cultural traditions of folk dance in Estonia, it does not evoke uncertainty or aversion compared to classical dance styles. Participants learned Estonian folk and social dance techniques and dance coordination. During dance training, each participant with Parkinson’s disease was paired with a healthy volunteer partner. Partners were not changed throughout the training. Various movement directions were used, including rotational movements, movements in columns, circles, and formations with live music. Contra dances, based on paired movements, alternating step dances combining walking steps and foot stamps, using various dance techniques and formations, were employed. The goal of dance training was to enhance the ability to follow musical rhythm and meter, remember dance step combinations, and use spatial awareness to accommodate the movement of the partner and other couples.
Statistical analysis
Data analysis was performed using SPSS version 2.4.6. Descriptive statistics were calculated to summarize characteristics at baseline. To compare group differences before the intervention, one-way ANOVA with Bonferroni post hoc tests was performed. For within-group comparisons before and after the intervention, a paired sample Student's t-test was used. Statistical significance was set at p <0.05. The interpretation of effect sizes was based on Cohen’s guidelines [59], where values of 0.2 represent a small effect, 0.5 a medium effect, and 0.8 or higher a large effect.
Results
The final sample consisted of 60 patients assigned to therapy groups based on randomization. During the therapeutic interventions, three participants withdrew from the study due to health and family reasons. Five participants, who attended less than 75% of the planned activities, were excluded from the final sample. The final sample included 48 patients, comprising 21 men and 27 women. Figure 1 provides an overview of the formation of the final sample.
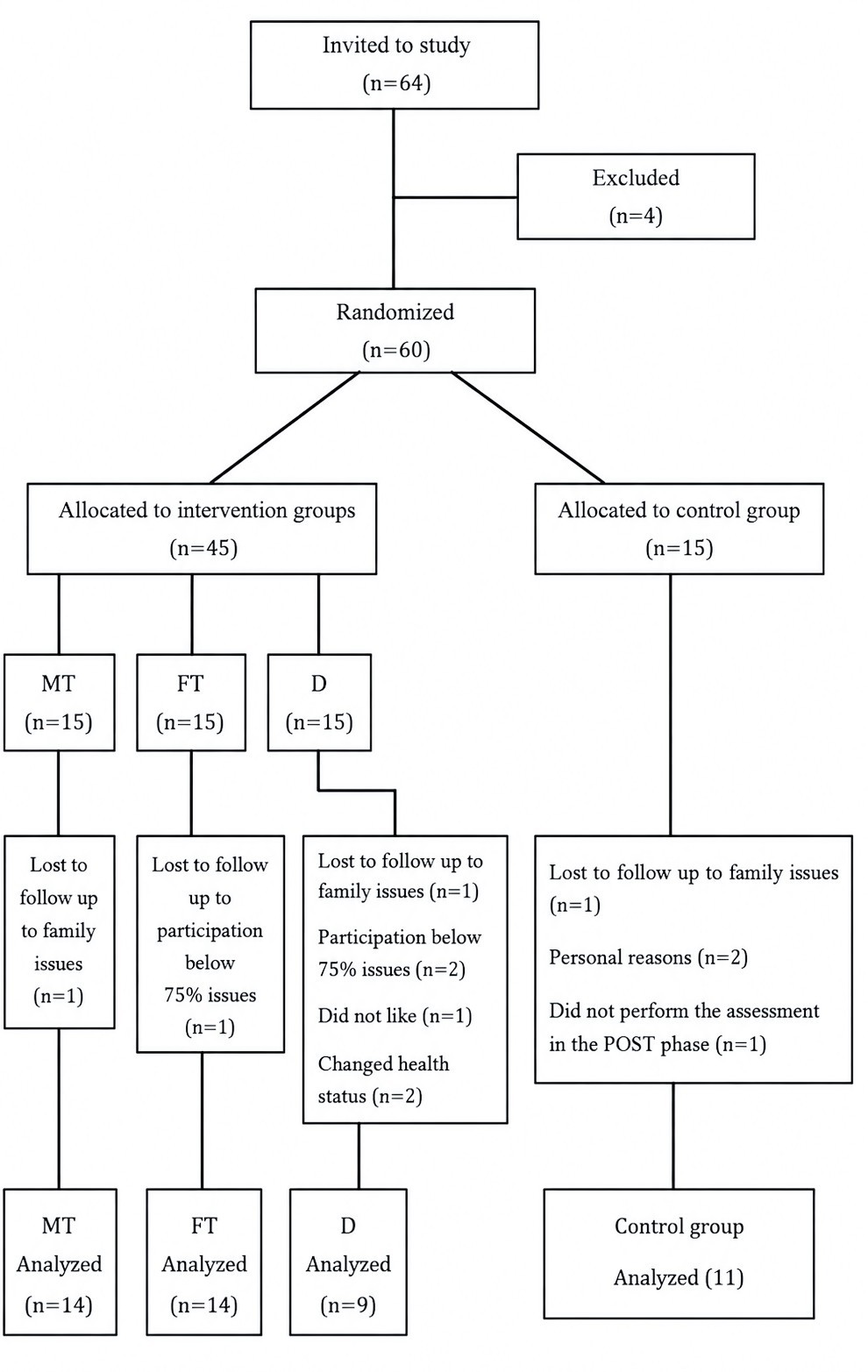
Figure 1. An overview of the formation of the final sample.
Before the intervention, there were no statistically significant differences in the psychological states of the participants between the groups, except for depression. Depression scores were statistically significantly lower in the music therapy group compared to both the dance therapy group (p = 0.022) and the control group (p = 0.020).
The study results indicated that the emotional state of patients with moderate Parkinson's disease improved following participation in group-based therapies. Positive effects on subjective self-assessment scales for depression reduction were observed in music therapy (p = 0.003; d= 1,29), dance training (p = 0.002; d=1,13), and physiotherapy (p = 0.012; d= 2,84). No corresponding changes were observed in the control group (Figure 2).
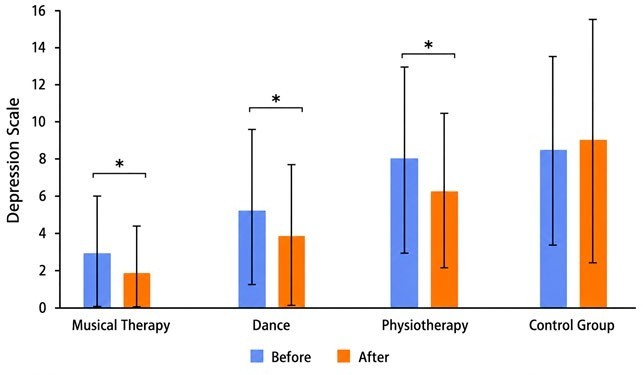
Figure 2. Effects of a group-based therapy intervention on depression.
A positive effect on the reduction of generalized anxiety was found in music therapy (p = 0.001; d= 1,92) and physiotherapy (p = 0.008; d=1,56). Dance training did not show a statistically significant effect on generalized anxiety (Figure 3).
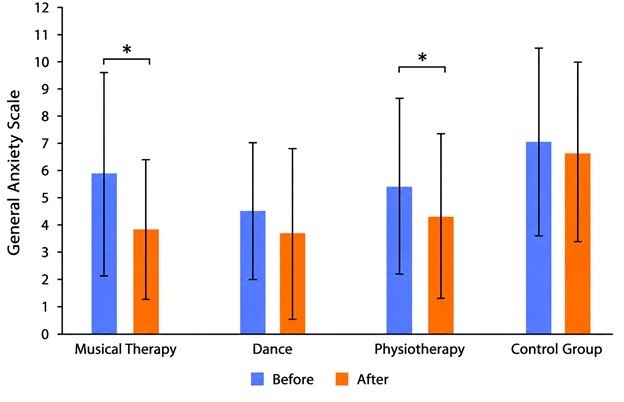
Figure 3. Effects of a group-based therapy intervention on generalized anxiety.
A statistically significant reduction in agoraphobia-panic disorder symptoms was observed in patients who participated in music therapy (p = 0.041; d= 0,43) and physiotherapy (p = 0.027; d= 0,63) (Figure 4).
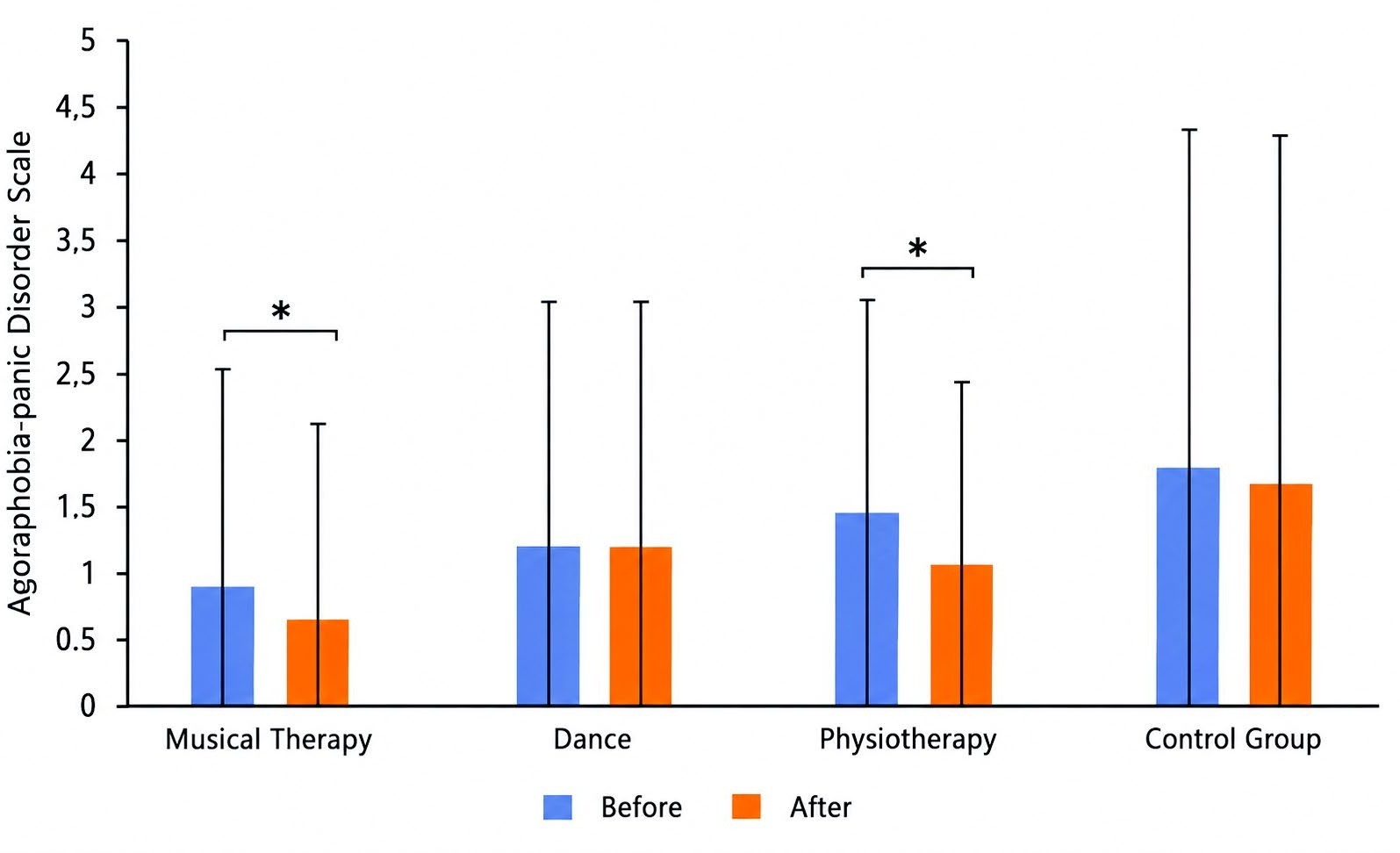
Figure 4. Effects of a group-based therapy intervention on agoraphobia-panic disorder.
A similar positive effect was observed in the reduction of social phobia symptoms, with statistically significant improvements found in music therapy (p = 0.006; d = 0,65) and physiotherapy (p= 0.028; d = 1.15) (Figure 5)
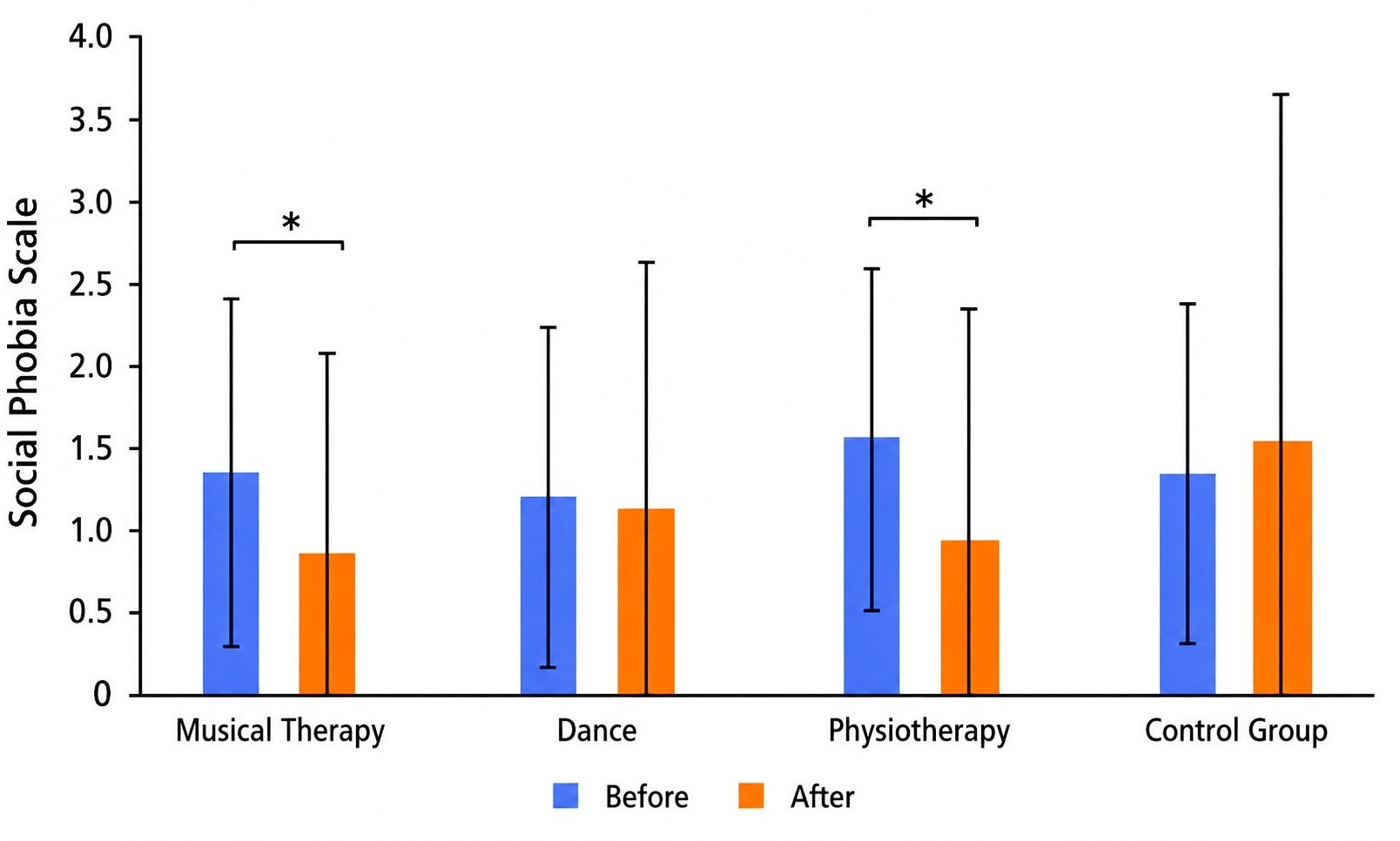
Figure 5. Effects of a group-based therapy intervention on social phobia.
Statistically significant effects on the reduction of asthenia and insomnia were observed for all three therapeutic interventions compared to the control group. Physiotherapy demonstrated the most significant effect (generalized asthenia: p = 0.000, d 0,95; insomnia: p= 0.000; d= 1,22) (Figures 6 and 7).
Based on the results of this study, music therapy emerged as the most effective intervention for several emotional states, significantly impacting depression, general anxiety, panic disorder, social phobia and insomnia. Physiotherapy proved to be the most effective for general anxiety, general asthenia, and insomnia. Dance training demonstrated significant effects on depression, general asthenia, and insomnia, but did not show a significant impact on the reduction of panic disorder and social phobia.
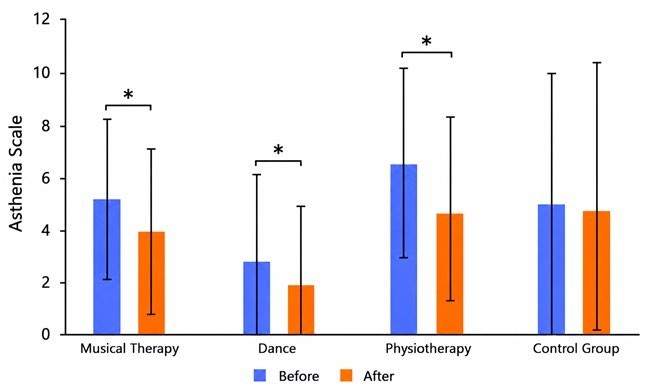
Figure 6. Effects of a group-based therapy intervention on asthenia.
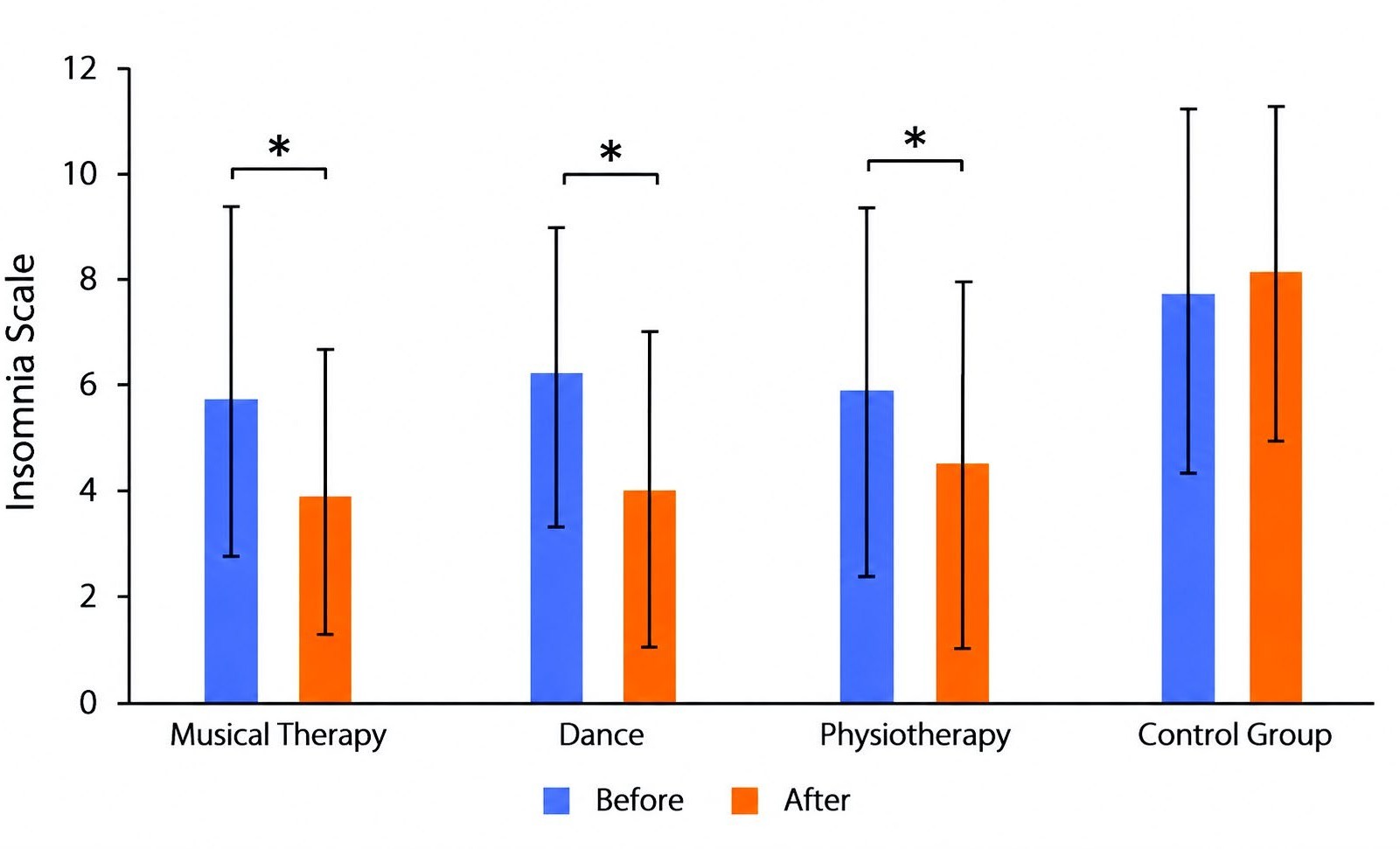
Figure 7. Effects of a group-based therapy intervention on insomnia.
Discussion
This study aimed to investigate the changes in the emotional well-being of patients with moderate Parkinson’s disease (PD) following the application of various group-based therapeutic interventions. The results revealed that participation in physiotherapy, music therapy, and dance training significantly improved the emotional state of these patients, reducing symptoms of depression, generalized anxiety, agoraphobia-panic disorder, social phobia, asthenia, and insomnia.
Impact on depression and anxiety
Music therapy demonstrated significant effectiveness in reducing symptoms of depression among participants. This finding aligns with previous studies that emphasize the therapeutic benefits of music in enhancing emotional well-being and alleviating depressive symptoms [43,60]. The structured use of musical elements during therapeutic sessions likely facilitated emotional expression and regulation, which is critical in managing depression [54]. Mechanisms of music therapy involve the activation of brain regions responsible for processing emotional information through auditory stimulation, promoting relaxation and mood improvement [61].
Participants in physiotherapy also showed significant improvements in depression symptoms. Schenkman et al. [62] highlighted the role of physical activity in the release of endorphins and the reduction of stress levels, which can alleviate depressive conditions. While dance training had a positive effect on depression, its impact was less pronounced compared to music therapy. Westheimer et al. [63] found that the social engagement and physical activity associated with dance support emotional well-being and reduce feelings of isolation, which are often linked to depression. Malouka et al. [43] suggested that while physical activity is beneficial, the additional emotional and cognitive engagement provided by music may enhance therapeutic outcomes. Hackney & Earhart [64] also demonstrated in their study that tango improved mood and reduced depressive symptoms.
Generalized anxiety
The study found that both music therapy and physiotherapy effectively reduced generalized anxiety, with music therapy having a slightly stronger impact. The rhythmic and melodic elements of music therapy may have contributed to anxiety reduction by promoting relaxation and regulating physiological responses, such as heart rate and breathing [55]. A meta-analysis of randomized controlled trials (32 RCTs with 1924 participants in total) shows that music therapy can significantly reduce anxiety [65].
Physiotherapy, which also showed a significant effect, is often associated with stress reduction through physical activity. However, the present findings suggest that not all forms of physical activity influence anxiety through identical mechanisms. One important distinction between the interventions may be the inclusion of structured breathing and regulation-focused elements. In this study, both physiotherapy and music therapy incorporated components that likely facilitated breathing control and enhanced body awareness, which are known to support autonomic regulation and contribute to anxiety reduction.
However, the dance training, although physically and rhythmically engaging, did not explicitly emphasize breathing techniques or mindfulness-related components. This difference may partly explain why dance did not produce a significant reduction in generalized anxiety. It is also possible that the cognitive and coordinative demands of learning movement sequences in dance may have reduced its potential for relaxation in this population.
These findings are consistent with previous research suggesting that the effects of dance interventions on anxiety in Parkinson’s disease are variable and may depend on the specific structure and therapeutic focus of the program [66–68]. Further research is needed to clarify which components of movement-based interventions are most effective in reducing anxiety in this population.
Panic disorder and social phobia
Both music therapy and physiotherapy significantly reduced symptoms of panic disorders and social phobia, reinforcing the notion that these treatments play a crucial role in managing anxiety-related conditions in PD patients [39]. Music therapy's ability to engage both cognitive and emotional processes may explain its effectiveness in reducing panic symptoms and helping patients manage their emotional responses to stress [42]. The findings regarding social phobia are particularly noteworthy, suggesting that these interventions may also improve social functioning, often compromised in PD due to anxiety and motor symptoms [46]. While the impact of physiotherapy on panic disorders and social phobia has been less studied, Brauer et al. [69] noted that physiotherapy promotes self-efficacy and social participation, potentially reducing anxiety. This study’s physiotherapy included balance exercises, which may have contributed to the emotional improvements observed. The effect of dance therapy on these emotional conditions remains limited, with most studies focusing on broader categories of anxiety. Conversely, dance training showed no statistically significant impact on these conditions, possibly due to its less targeted approach to addressing phobic symptoms and anxiety triggers. Further research is required to optimize dance therapy’s structure to achieve more robust outcomes in anxiety management.
Asthenia and insomnia
All three interventions—music therapy, physiotherapy, and simplified dance training—were effective in reducing symptoms of asthenia and insomnia, with physiotherapy showing the most significant impact. This supports previous research indicating that physical exercise can improve sleep quality and reduce fatigue in PD patients [42,50]. The incorporation of rhythmic physical activity in both physiotherapy and dance training may have contributed to better sleep habits and reduced fatigue by promoting a more regular sleep-wake cycle [40] Similarly, Comella [70] and King et al. [71] demonstrated improvements in both asthenia and sleep quality in their studies. The comparatively limited impact of dance training may reflect differences in physical intensity and the specific nature of exercises used, suggesting that tailored modifications to dance therapy protocols could enhance its efficacy in addressing these symptoms. Asthenia and insomnia have been less studied in the context of music therapy, although Gao et al. [72] found that slow-tempo music can improve sleep patterns in patients with neurological disorders.
Group-based interventions
The findings of the present study suggest that group-based interventions may play an important role in improving emotional well-being in patients with Parkinson’s disease. Improvements observed across multiple emotional domains, including depression, anxiety, and insomnia, may be partly explained by the social and interactive nature of group-based settings. Such environments provide structured social engagement and peer support, which may help reduce social isolation and enhance emotional regulation, both of which are particularly relevant in this population [73].
In addition, group-based interventions may exert their effects through different but complementary mechanisms depending on the modality. Physiotherapy may contribute through physical activation and improved self-efficacy, music therapy through emotional and cognitive engagement, and dance through the integration of movement, rhythm, and social interaction. These combined effects may explain the broad improvements observed in the present study.
Although statistically significant improvements were observed across several emotional domains, the clinical relevance of these findings should be interpreted cautiously. No established Minimal Clinically Important Difference (MCID) values are currently available for the EST-Q2, particularly in Parkinson's disease populations. Nevertheless, as the questionnaire captures patient-reported subjective emotional experiences, the observed changes may still reflect meaningful improvements in perceived well-being and emotional functioning. In the absence of MCID thresholds, effect sizes (Cohen's d) were used to contextualize the magnitude of observed changes, with several interventions demonstrating medium to large effects according to Cohen's criteria [59]. Establishing MCID values for the EST-Q2 in Parkinson's disease populations remains an important direction for future research.
Conclusion
In conclusion, the study’s findings support the effectiveness of group-based therapeutic interventions in improving the emotional well-being of patients with Parkinson’s disease. Physiotherapy, music therapy, and dance training provide significant emotional support in addition to alleviating physical symptoms, enhancing the overall quality of life for these patients. These findings suggest that such interventions should be part of comprehensive treatment protocols for PD patients. Future research should explore the long-term effects of these therapies and the potential synergies in combining different therapeutic modalities.
Furthermore, while the study provided valuable insights into the effectiveness of group-based therapies, it did not explore the potential benefits of combining these interventions. Previous research suggests that a multidisciplinary approach combining different therapies may offer greater benefits for both the emotional and physical health of PD patients [44]. Therefore, future studies should consider investigating the effects of combined therapeutic protocols.
Strengths
Variety of therapeutic interventions
The study evaluates several therapeutic interventions—music therapy, physiotherapy, and simplified dance training—which allows for a comprehensive comparison of different approaches. This broad approach helps to understand the varied effects of each treatment on emotional states related to Parkinson's disease (PD).
Use of validated instruments
The emotional state questionnaire (EST-Q2) used in this study is a validated and reliable tool for assessing a range of emotional states, including depression, anxiety, panic disorders, social phobia, asthenia, and insomnia within the Estonian population. This enhances the reliability of the results and ensures that the collected data is trustworthy and relevant [53].
Standardized intervention protocols
Interventions were conducted using standardized protocols, including treatment methods specific to each group. For example, music therapy includes evidence-based techniques such as Therapeutic Instrumental Music Performance (TIMP) and Vocal Intonation Therapy (VIT) [54]. This structured approach increases the reliability of the results by ensuring consistency across sessions. In physiotherapy, a balance development program was applied consistently throughout the intervention period.
Controlled conditions
The study controlled for potential confounding variables by ensuring that participants' treatment regimens remained unchanged and that none of the participants had previous experience with the forms of therapy applied. In the dance training, participants were paired with a healthy partner, who remained the same throughout the intervention. This likely reduces the risk of external factors influencing the results.
Comprehensive assessment
The study evaluated a wide range of emotional states and included both pre- and post-intervention assessments. This comprehensive evaluation provides a detailed picture of how each treatment affects various aspects of emotional well-being in PD patients.
Limitations
Despite promising results, the present study has several limitations. The sample size was relatively small — approximately 12 participants per group — which limits statistical power and generalizability. This is partly explained by Estonia's total Parkinson's disease population of approximately 3,500, which imposes inherent recruitment constraints on single-center studies; multicenter collaboration would be needed to achieve larger samples. A pre-existing baseline imbalance in depression scores — with the music therapy group scoring lower than both the dance training (p=0.022) and control groups (p=0.020) — further limits group comparability on this subscale, and the absence of post-intervention between-group comparisons restricts conclusions about relative intervention effectiveness. The eight-week intervention period and lack of long-term follow-up limit conclusions about the sustainability of the observed effects, particularly given that initial improvements may partly reflect transient dopaminergic responses to novel stimuli rather than lasting therapeutic change. Finally, the absence of an active control condition means that non-specific effects of group participation cannot be fully ruled out. Future studies should employ larger multicenter samples, longer follow-up periods, and active control conditions to better isolate the specific mechanisms of each therapeutic modality. Additionally, investigating the potential benefits of combined therapeutic protocols remains an important direction, as a multidisciplinary approach may offer greater benefits for both the emotional and physical health of PD patients.
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Funding Statement
This research was funded by the Tallinn University Research Fund under project number TF3720, approved by the decision of the Tallinn University Research Fund Council (decision no. 7.1-17/4, April 29, 2020).
Acknowledgements
The authors would like to thank all participants for their time, commitment, and willingness to take part in this study. We also acknowledge the healthcare professionals and therapists involved in the delivery of the music therapy, dance training, and physiotherapy interventions for their valuable support and cooperation. The authors are grateful to the institutions that facilitated participant recruitment and data collection. The authors also thank colleagues who provided methodological and practical support during the study.
References
2. Gómez-Esteban JC, Zarranz JJ, Lezcano E, Tijero B, Luna A, Velasco F, et al. Influence of motor symptoms upon the quality of life of patients with Parkinson's disease. Eur Neurol. 2007;57(3):161–5.
3. Dorsey ER, Sherer T, Okun MS, Bloem BR. The Emerging Evidence of the Parkinson Pandemic. J Parkinsons Dis. 2018;8(s1):S3–8.
4. Váradi C. Clinical Features of Parkinson's Disease: The Evolution of Critical Symptoms. Biology (Basel). 2020 May 19;9(5):103.
5. Majali MA, Sunnaa M, Chand P. Emerging Pharmacotherapies for Motor Symptoms in Parkinson's Disease. J Geriatr Psychiatry Neurol. 2021 Jul;34(4):263–73.
6. Deuel LM, Seeberger LC. Complementary Therapies in Parkinson Disease: a Review of Acupuncture, Tai Chi, Qi Gong, Yoga, and Cannabis. Neurotherapeutics. 2020 Oct;17(4):1434–55.
7. Chaudhuri KR. Thirty years of research on autonomic dysfunction, non-motor features, and endophenotypes in Parkinson disease. Clin Auton Res. 2021 Feb;31(1):37–9.
8. Seppi K, Ray Chaudhuri K, Coelho M, Fox SH, Katzenschlager R, Perez Lloret S, etal .the collaborators of the Parkinson's Disease Update on Non-Motor Symptoms Study Group on behalf of the Movement Disorders Society Evidence-Based Medicine Committee. Update on treatments for nonmotor symptoms of Parkinson's disease-an evidence-based medicine review. Mov Disord. 2019 Feb;34(2):180–98.
9. Ahmad MH, Rizvi MA, Ali M, Mondal AC. Neurobiology of depression in Parkinson's disease: Insights into epidemiology, molecular mechanisms and treatment strategies. Ageing Res Rev. 2023 Mar;85:101840.
10. Rosińczuk J, Kołtuniuk A. The influence of depression, level of functioning in everyday life, and illness acceptance on quality of life in patients with Parkinson's disease: a preliminary study. Neuropsychiatr Dis Treat. 2017 Mar 21;13:881–7.
11. Kim J, Criaud M, Cho SS, Díez-Cirarda M, Mihaescu A, Coakeley S, et al. Abnormal intrinsic brain functional network dynamics in Parkinson's disease. Brain. 2017 Nov 1;140(11):2955–67.
12. Balestrino R, Baroncini D, Fichera M, Donofrio CA, Franzin A, Mortini P, et al. Weight gain after subthalamic nucleus deep brain stimulation in Parkinson's disease is influenced by dyskinesias' reduction and electrodes' position. Neurol Sci. 2017 Dec;38(12):2123–29.
13. Zhang T, Yang R, Pan J, Huang S. Parkinson's Disease Related Depression and Anxiety: A 22-Year Bibliometric Analysis (2000-2022). Neuropsychiatr Dis Treat. 2023 Jun 29;19:1477–89.
14. Chendo I, Silva C, Duarte GS, Prada L, Vian J, Quintão ,et al. Frequency of Depressive Disorders in Parkinson's Disease: A Systematic Review and Meta-Analysis. J Parkinsons Dis. 2022;12(5):1409–18
15. Gulunay A, Cakmakli GY, Yon MI, Ulusoy EK, Karakoc M. Frequency of non-motor symptoms and their impact on the quality of life in patients with Parkinson's disease: a prospective descriptive case series. Psychogeriatrics. 2020 Mar;20(2):206-211.
16. Duarte Folle A, Paul KC, Kusters CD, Bronstein JM, Keener AM, Ritz B. Parkinson’s disease motor and non-motor features accompanying insomnia and excessive daytime sleepiness symptoms, a large population-based study. OBM Geriatrics. 2020 Aug;4(3):1–17.
17. Chen JJ, Marsh L. Anxiety in Parkinson's disease: identification and management. Ther Adv Neurol Disord. 2014 Jan;7(1):52–9.
18. Blundell EK, Grover LE, Stott J, Schrag A. The experience of Anxiety for people with Parkinson's disease. NPJ Parkinsons Dis. 2023 May 17;9(1):75.
19. Dissanayaka NN, White E, O'Sullivan JD, Marsh R, Pachana NA, Byrne GJ. The clinical spectrum of anxiety in Parkinson's disease. Mov Disord. 2014 Jul;29(8):967–75.
20. Broen MP, Narayen NE, Kuijf ML, Dissanayaka NN, Leentjens AF. Prevalence of anxiety in Parkinson's disease: A systematic review and meta-analysis. Mov Disord. 2016 Aug;31(8):1125–33.
21. Bloem BR, Okun MS, Klein C. Parkinson's disease. Lancet. 2021 Jun 12;397(10291):2284–303.
22. Santos‐García D, de Deus Fonticoba T, Suárez Castro E, Aneiros Díaz A, McAfee D, Catalán MJ, et al. Non‐motor symptom burden is strongly correlated to motor complications in patients with Parkinson’s disease. European Journal of Neurology. 2020 Jul;27(7):1210–23.
23. Kurihara K, Nakagawa R, Ishido M, Yoshinaga Y, Watanabe J, Hayashi Y, et al. Impact of motor and nonmotor symptoms in Parkinson disease for the quality of life: The Japanese Quality-of-Life Survey of Parkinson Disease (JAQPAD) study. J Neurol Sci. 2020 Dec 15;419:117172.
24. Avanzino L, Lagravinese G, Abbruzzese G, Pelosin E. Relationships between gait and emotion in Parkinson's disease: A narrative review. Gait Posture. 2018 Sep;65:57–64.
25. Kang MY, Ellis-Hill C. How do people live life successfully with Parkinson's disease? J Clin Nurs. 2015 Aug;24(15-16):2314–22.
26. Brandt L, Liu S, Heim C, Heinz A. The effects of social isolation stress and discrimination on mental health. Transl Psychiatry. 2022 Sep 21;12(1):398.
27. Heusinkveld LE, Hacker ML, Turchan M, Davis TL, Charles D. Impact of Tremor on Patients With Early Stage Parkinson's Disease. Front Neurol. 2018 Aug 3;9:628.
28. Ray Chaudhuri K, Poewe W, Brooks D. Motor and Nonmotor Complications of Levodopa: Phenomenology, Risk Factors, and Imaging Features. Mov Disord. 2018 Jul;33(6):909–19.
29. Chen R, Berardelli A, Bhattacharya A, Bologna M, Chen KS, Fasano A, et al. Clinical neurophysiology of Parkinson's disease and parkinsonism. Clin Neurophysiol Pract. 2022 Jun 30;7:201–27.
30. Wamelen DJV, Rukavina K, Podlewska AM, Chaudhuri KR. Advances in the Pharmacological and Non-pharmacological Management of Non-motor Symptoms in Parkinson's Disease: An Update Since 2017. Curr Neuropharmacol. 2023;21(8):1786–805.
31. Zhang Y, Liu S, Xu K, Zhou Y, Shen Y, Liu Z, et al. Non-pharmacological therapies for treating non-motor symptoms in patients with Parkinson's disease: a systematic review and meta-analysis. Front Aging Neurosci. 2024 Apr 26;16:1363115.
32. Jiang X, Zhang L, Liu H, Su H, Jiang J, Qiang C, et al. Efficacy of non-pharmacological interventions on depressive symptoms in patients with Parkinson's disease: a study protocol for a systematic review and network meta-analysis. BMJ Open. 2023 May 2;13(5):e068019.
33. Rafferty MR, Schmidt PN, Luo ST, Li K, Marras C, Davis TL, et al; all NPF-QII Investigators. Regular Exercise, Quality of Life, and Mobility in Parkinson's Disease: A Longitudinal Analysis of National Parkinson Foundation Quality Improvement Initiative Data. J Parkinsons Dis. 2017;7(1):193–202.
34. Moratelli JA, Lima AG, Alexandre KH, Fausto DY, Haas AN, de Azevedo Guimarães AC. Evidence of physical activity interventions on non-motor symptoms of people with Parkinson’s disease: An umbrella review. Sport Sciences for Health. 2024 Jun;20(2):321–36.
35. Alnajjar AZ, Abouelmagd ME, Krayim A, AbdelMeseh M, Bushara N, Nabil Y. Efficacy of cognitive behavioral therapy for anxiety and depression in Parkinson's disease patients: an updated systematic review and meta-analysis. Neurol Sci. 2024 Nov;45(11):5277–90.
36. Luo F, Ye M, Lv T, Hu B, Chen J, Yan J, et al. Efficacy of Cognitive Behavioral Therapy on Mood Disorders, Sleep, Fatigue, and Quality of Life in Parkinson's Disease: A Systematic Review and Meta-Analysis. Front Psychiatry. 2021 Dec 13;12:793804.
37. Zarotti N, Eccles FJR, Foley JA, Paget A, Gunn S, Leroi I, et al. Psychological interventions for people with Parkinson's disease in the early 2020s: Where do we stand? Psychol Psychother. 2021 Sep;94(3):760–797.
38. Vescovelli F, Cesetti G, Sarti D, Ruini C. Adapted Physical Activity Can Increase Life Appreciation in Patients with Parkinson's Disease. Int J Aging Hum Dev. 2024 Mar;98(2):221–42.
39. Wang L, Peng JL, Ou-Yang JB, Gan L, Zeng S, Wang HY, et al. Effects of Rhythmic Auditory Stimulation on Gait and Motor Function in Parkinson's Disease: A Systematic Review and Meta-Analysis of Clinical Randomized Controlled Studies. Front Neurol. 2022 Apr 15;13:818559.
40. Mele B, Ismail Z, Goodarzi Z, Pringsheim T, Lew G, Holroyd-Leduc J. Non-pharmacologic interventions to treat apathy in Parkinson's disease: A realist review. Clin Park Relat Disord. 2021 May 25;4:100096.
41. Qureshi AR, Jamal MK, Rahman E, Paul DA, Oghli YS, Mulaffer MT, et al. Non-pharmacological therapies for pain management in Parkinson's disease: A systematic review. Acta Neurol Scand. 2021 Aug;144(2):115–31.
42. Koshimori Y, Thaut MH. Rhythmic auditory stimulation as a potential neuromodulator for Parkinson's disease. Parkinsonism Relat Disord. 2023 Aug;113:105459.
43. Malouka S, Loria T, Crainic V, Thaut MH, Tremblay L. Auditory cueing facilitates temporospatial accuracy of sequential movements. Hum Mov Sci. 2023 Jun;89:103087.
44. Machado Sotomayor MJ, Arufe-Giráldez V, Ruíz-Rico G, Navarro-Patón R. Music Therapy and Parkinson's Disease: A Systematic Review from 2015-2020. Int J Environ Res Public Health. 2021 Nov 4;18(21):11618.
45. Saluja A, Goyal V, Dhamija RK. Multi-Modal Rehabilitation Therapy in Parkinson's Disease and Related Disorders. Ann Indian Acad Neurol. 2023 Jan;26(Suppl 1):S15–25.
46. Moţ RD, Almăjan-Guţă B. Dance therapy for Parkinson's disease: a systematic review. Timisoara Physical Education and Rehabilitation Journal. 2022;15(28):55–65.
47. Lötzke D, Ostermann T, Büssing A. Argentine tango in Parkinson disease--a systematic review and meta-analysis. BMC Neurol. 2015 Nov 5;15:226.
48. Hackney ME, Earhart GM. Effects of dance on movement control in Parkinson's disease: a comparison of Argentine tango and American ballroom. J Rehabil Med. 2009 May;41(6):475–81.
49. Rios Romenets S, Anang J, Fereshtehnejad SM, Pelletier A, Postuma R. Tango for treatment of motor and non-motor manifestations in Parkinson's disease: a randomized control study. Complement Ther Med. 2015 Apr;23(2):175–84.
50. Cusso ME, Donald KJ, Khoo TK. The Impact of Physical Activity on Non-Motor Symptoms in Parkinson's Disease: A Systematic Review. Front Med (Lausanne). 2016 Aug 17;3:35.
51. Ferrusola-Pastrana A, Fullerton CL, Meadows SN. Group-based exercise for Parkinson's: a qualitative study of participants and partners' perceptions of an exercise class delivered through a community-university collaboration. BMC Geriatr. 2024 Jun 4;24(1):488.
52. Ferrazzoli D, Ortelli P, Cucca A, Bakdounes L, Canesi M, Volpe D. Motor-cognitive approach and aerobic training: a synergism for rehabilitative intervention in Parkinson's disease. Neurodegener Dis Manag. 2020 Feb;10(1):41–55.
53. Aluoja A, Shlik J, Vasar V, Luuk K, Leinsalu M. Development and psychometric properties of the Emotional State Questionnaire, a self-report questionnaire for depression and anxiety. Nordic Journal of Psychiatry. 1999 Jan 1;53(6):443–9.
54. Thaut MH, McIntosh GC, Hoemberg V. Handbook of neurologic music therapy. Oxford; 2014.
55. McFerran K, Grocke D. Receptive music therapy: Techniques, clinical applications and new perspectives. Jessica Kingsley Publishers; 2022.
56. Khallaf M, Jaber H, Alameri M, Magdy D, Kamal H, Hassanin M, et al. Effect of Vestibular-Oriented Balance Training on Postural Control and Risk of Fall in Patients With Parkinson's Disease. Neurol Res Int. 2025 Feb 25;2025:6846267.
57. Martiš P, Bzdúšková D, Košutzká Z, Slobodová L, Straka I, Marček Malenovská K, et al. Supervised aerobic-strength exercise reduces postural sway and improves dual-task gait in Parkinson's disease. Sci Rep. 2025 Jul 1;15(1):20643.
58. Wang D, Cui WJ, Hou ZH, Gao Y. Effectiveness of different exercises in improving postural balance among Parkinson's disease patients: a systematic review and network meta-analysis. Front Aging Neurosci. 2023 Jul 17;15:1215495.
59. Cohen J. Statistical Power Analysis for the Behavioral Sciences (2nd Edition).1988.
60. Tang Q, Huang Z, Zhou H, Ye P. Effects of music therapy on depression: A meta-analysis of randomized controlled trials. PLoS One. 2020 Nov 18;15(11): e0240862.
61. Raglio A, Bellandi D, Baiardi P, Gianotti M, Ubezio MC, Zanacchi E, et al. Effect of Active Music Therapy and Individualized Listening to Music on Dementia: A Multicenter Randomized Controlled Trial. J Am Geriatr Soc. 2015 Aug;63(8):1534–9.
62. Schenkman M, Moore CG, Kohrt WM, Hall DA, Delitto A, Comella CL, et al. Effect of High-Intensity Treadmill Exercise on Motor Symptoms in Patients With De Novo Parkinson Disease: A Phase 2 Randomized Clinical Trial. JAMA Neurol. 2018 Feb 1;75(2):219–226.
63. Westheimer O, McRae C, Henchcliffe C, Fesharaki A, Glazman S, Ene H, et al. Dance for PD: a preliminary investigation of effects on motor function and quality of life among persons with Parkinson's disease (PD). J Neural Transm (Vienna). 2015 Sep;122(9):1263–70.
64. Hackney ME, Earhart GM. Health-related quality of life and alternative forms of exercise in Parkinson disease. Parkinsonism Relat Disord. 2009 Nov;15(9):644–8.
65. Lu G, Jia R, Liang D, Yu J, Wu Z, Chen C. Effects of music therapy on anxiety: A meta-analysis of randomized controlled trials. Psychiatry Res. 2021 Oct;304:114137.
66. McKee KE, Hackney ME. The effects of adapted tango on spatial cognition and disease severity in Parkinson's disease. J Mot Behav. 2013;45(6):519–29.
67. Carapellotti AM, Rodger M, Doumas M. Evaluating the short-term effects of dance on motor and non-motor outcomes in people living with Parkinson's: A crossover study. PLoS One. 2025 Jul 31;20(7):e0328293.
68. Ismail SR, Lee SWH, Merom D, Megat Kamaruddin PSN, Chong MS, Ong T, et al. Evidence of disease severity, cognitive and physical outcomes of dance interventions for persons with Parkinson's Disease: a systematic review and meta-analysis. BMC Geriatr. 2021 Sep 22;21(1):503.
69. Brauer SG, Lamont RM, O'Sullivan JD. A physiotherapy group exercise and self-management approach to improve physical activity in people with mild-moderate Parkinson's disease: a randomized controlled trial. Trials. 2024 Jan 22;25(1):76.
70. Comella CL. Sleep disorders in Parkinson's disease: an overview. Mov Disord. 2007 Sep;22 Suppl 17: S367–73.
71. King LA, Salarian A, Mancini M, Priest KC, Nutt J, Serdar A, et al. Exploring outcome measures for exercise intervention in people with Parkinson's disease. Parkinsons Dis. 2013;2013:572134.
72. Gao D, Long S, Yang H, Cheng Y, Guo S, Yu Y, et al. SWS Brain-Wave Music May Improve the Quality of Sleep: An EEG Study. Front Neurosci. 2020 Feb 11;14:67.
73. Tomlinson CL, Herd CP, Clarke CE, Meek C, Patel S, Stowe R, et al. Physiotherapy for Parkinson's disease: a comparison of techniques. Cochrane Database Syst Rev. 2014 Jun 17;2014(6):CD00281.