Abstract
With a global increase in the occurrence of Autism Spectrum Disorder (ASD), there is an increase in the need for special educational techniques. The traditional method has done a great deal in teaching children with ASD. However, children diagnosed with ASD still have issues identifying objects, shapes, colors, etc. This study develops an application using the design thinking approach to help children diagnosed with ASD identify their drug. The design thinking approach is used in the development of the application. The data used were retrieved from interviews with medical professionals, parents, and guardians of children diagnosed with ASD using the empathy approach. The data was analyzed and used to define a problem statement. Edutainment was introduced as a medium to drive learning, and hence, took the form of a game. A prototype of the application was built using Flutter SDK (Software Development Kit) and Firebase real-time database and tested on five children diagnosed with ASD. The results show that for every second interaction the children had with the application, as the time spent decreased, the total score increased. In the first level, the average score of all five children increased from 16.2 to 30 to 23.4. This indicated that the children were learning and proved to be a great medium for teaching children with ASD. In conclusion, the research work provided a learning platform for children diagnosed with ASD, which will be highly useful for further development of the children.
Keywords
Design thinking, Autism spectrum disorder, Applied behavioral analysis, E-learning, Edutainment, Flutter SDK, and Firebase real-time
Introduction
Autism Spectrum Disorder (ASD) is a heterogeneous developmental condition that involves continuous challenges in social interaction, verbal and nonverbal communication, and restricted or repetitive behaviors; hence, it can be termed as a neuro developmental disability that is manifested in an individual. The effects of ASD and the severity of symptoms vary in each person [1]. Autism is a social and communication disorder typically associated with Restricted Interest and Repetitive Behavior (RIRB) [2]. Autism has a prevalence of over half a million people in the UK [2] and is also thought to affect approximately 1–2% of individuals around the globe [3]. Incidence rates of autism have been progressively increasing as awareness has increased. Autism is deemed to be a hidden disability, indicating that the need for additional support is not instantly apparent. Various educational and emotional interventions are currently available to support autistic individuals [2]. More often than not, children with ASD can show momentary behaviors of severe agitation known as behavioral crisis. They tend to engage in disturbing activities, which at times lead to self-inflicted injuries. These agitations vary from one patient to another in terms of magnitude, duration, and frequency [3]. Design thinking is an analytic and creative process that allows a person to create and prototype models, gather feedback, and redesign [4].
Research has shown that an average of one in 160 children has ASD. More recent studies show that the global occurrence of ASD is increasing. This can be attributed to improved awareness, better diagnosis methods, and tools etc. [4].
The root cause of ASD is unknown, but it is believed that both genetic and environmental factors are involved [5]. There is no cure for ASD. However, early diagnosis and treatment can substantially improve the development of a child diagnosed with ASD [1]. Also, it has been revealed that individuals with ASD have impaired executive functions (i.e., a collection of brain processes that account for the normal functioning of human activity). In contrast to a typically developing human being, impairments are seen in their inability to appreciate social situations, recall and recognize written and spoken words, provide a logically sound narrative to a story [2]. Also in [6], an attempt was made using relevant data (drawing of waves) from individuals suffering from Parkinson’s Disease and non -patient of the disease to design and implement a system for early detection of the disease.
Methodology
The study employed the use of design thinking to address the challenges peculiar to drug identification for children with ASD. The process as shown in (Figure 1), ranges from data collection using the empathy approach, problem definition, idea creation, prototype development and testing among the user for feedback in order to fine-tune the performance of the product developed.
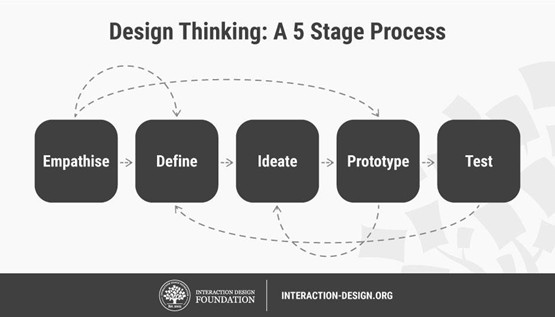
Figure 1. The 5 stage process of Design Thinking as described by [5].
Empathy
This involves gathering knowledge or data from medical professionals or consultants, teachers, parents, and guardians. It is necessary to empathize with patients about what they are facing and understand their point of view to fully tackle the problem. This was done using both structured and semi-structured interviews with care takers of children diagnosed with ASD. Relevant information about the drugs used, their administration, their effect and the learning structure in place for patients with ASD were captured. The new-found knowledge provides a clean slate to be able to define the problem.
Problem definition
In this stage, enough data has been gathered from the empathic approach to the extent that it is very possible to fully define the problem. Analysis, observation and terms are now collated into a dataset. The definition of the problem also involves the fact that there is a need for Autism Spectrum Disorder patients to learn how to identify their drugs. The data to be used as a prerequisite for building the new system are gotten from different sources. These sources include hospitals, parents, guardians, articles, journals, books, and autistic patients. Since not all autistic patients exhibit the same disability, some others do not have issues identifying, administering and/or remembering their prescribed drugs. The problem can be defined by identifying which particular disorder in the autism spectrum requires patients not to be able to identify their prescribed medication.
Idea creation
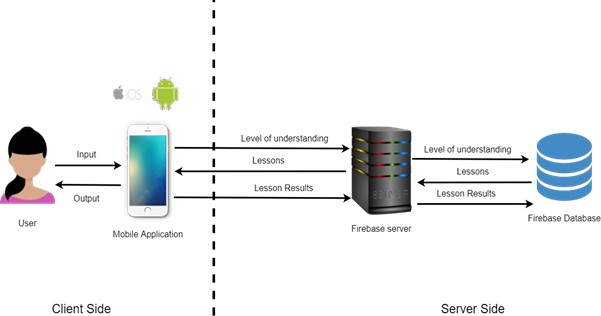
This involves brainstorming on possible solutions to the defined problem. Several interesting design ideas were shared over multiple thought sessions. The use of paper sketches, scenarios and mini prototypes were useful in illustrating and visualizing ideas. Figure 2 shows the proposed system architecture. The user inputs data which is used to determine the child’s level of understanding. Based on the level of understanding, appropriate lessons are displayed for the user. The results of lessons taken is also stored in the database.
Prototype Development and Experimental Setup
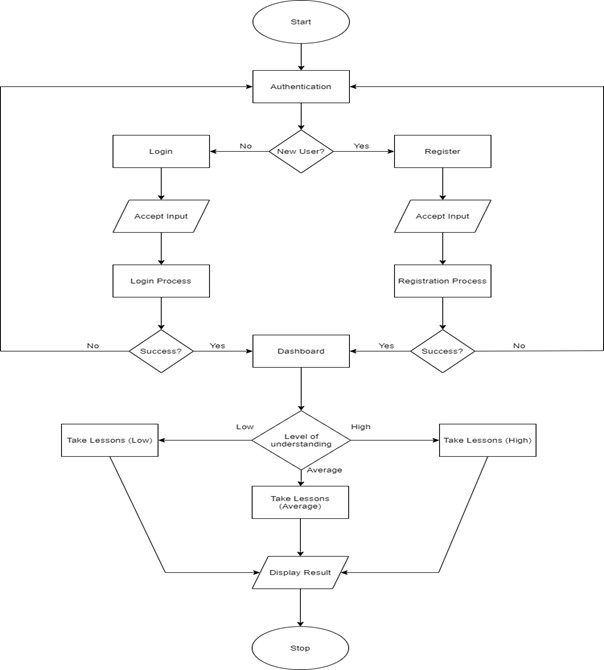
The ideas generated in the previous sections were implemented as prototypes for proper evaluation and improvement. The aim of this is to have a better understanding of the limitations inherent to the solution and problems at hand. The flow chart of the proposed system is shown in (Figure 3). A mobile application will be developed for the system. The mobile application will be developed using Android Studio, Flutter Software Development Kit (SDK), Android Emulator and Firebase real-time database. The user will interact with the user interface of the application to achieve tasks. Each lesson is presented as a game in which the students are shown an image of a drug and asked to select the same image from a variety of options.
Child’s details page
The user is expected to provide information about the child that will be learning on the application. This information includes full name, date of birth, and level of understanding (low, average and high). The purpose of this page is to gather information about the child that is learning. Information provided in this section determines the level of difficulty of lessons.
Caretaker details page
The user is expected to provide information about themselves. This information includes full name, email address, and relationship with a child (parent, sibling, medical professional, and guardian). The purpose of this page is to gather information about the caretaker of the child.
History page
This page shows a child’s history data in the kid’s arena. These data include the level, difficulty, score and time taken to finish that particular lesson. The purpose of this page is to have an overview of the child’s performance.
Child’s arena page
The child’s arena page presents the child with three (3) levels of lessons. While the first level is always unlocked, subsequent levels are locked until the child gets fifteen (15) out of a possible thirty (30) stars in each level.
Lessons page
Learning occurs on the lessons page. In teaching children diagnosed with autism spectrum disorder, the concept of edutainment is introduced. Each lesson is presented in the form of a game in which the children are shown an image of a drug and are asked to choose the same image from among the available possibilities. As shown in Figure 4, there are several variations of the lessons. Figure 4a depicts a lesson that consists just of a drug image. Figure 4b depicts a lesson in which an image of a drug is juxtaposed with an image of the sun, suggesting dawn. Figure 4c depicts a lesson with a drug image and another image of the joint moon and sun denoting afternoon. Figure 4d depicts a lesson with a drug image juxtaposed against a moon image to symbolize night. Figure 4e depicts a lesson with an image of a drug alongside images of the sun and moon, indicating that the drug should be taken in the morning and at night. Figure 4f depicts a lesson with an image of a drug alongside images of the sun, joint moon and sun, and moon, indicating that the drug should be taken in the morning, afternoon, and night. For each question in the application, the drug's color changes. This is to avoid the children becoming habituated to a specific color. Three (3) stars are given to a child who selects the proper option on the first try. When a child selects the correct answer on the second try, he or she receives two (2) stars. When a child chooses the correct option on the third or subsequent tries, he or she receives only one star. When a child selects the incorrect option, a sound is heard to inform them that they have chosen the incorrect option. Each lesson is timed, and once a certain amount of time has passed, a prompt appears on the screen, showing the correct response to the child. Children whose caregivers have determined that they have a low level of comprehension receive the prompt every 30 seconds, while those with a medium or high level of knowledge receive the prompt every 45 and 60 seconds, respectively. When a child completes a level with a minimum of 15 of 30 stars, he or she obtains a milestone badge. When the user clicks the "cancel" text, the user is prompted to input the arena pin.

Experimental Results
The mobile application developed was tested on children diagnosed with autism spectrum disorder at a special needs school in Lagos, Nigeria. A total of five students aged between 4 and 16 interacted with the application. Amongst this five, 2 were female and 3 were male. The teachers at the school identified all the children’s level of understanding as low. Each child attempted all three levels in a single round and had a total of two rounds. Two hours elapse between round 1 and 2. Some children were unable to complete all the rounds due to loss of interest or a behavioral crisis. The summary of each child’s performance during the test period is shown in Table 1.
|
Child |
Details |
Level 1 |
Level 2 |
Level 3 |
|
Child 1 |
Difficulty: Low Age: 12 Sex: Male |
Round 1 Score: 26/30 Time: 1 min 32 sec |
Round 1 Score: 24/30 Time: 1 min 55 sec |
Round 1 Score: 22/30 Time: 2 mins 38 sec |
|
|
|
Round 2 Score: 30/30 Time: 0 min 57 sec |
Round 2 Score: 28/30 Time: 0 min 47 sec |
Round 2 Score: 27/30 Time: 1 min 4 sec |
|
Child 2 |
Difficulty: Low Age: 10 Sex: Male |
Round 1 Score: 14/30 Time: 4 min 12 sec |
Round 1 Score: 12/30 Time: 6 min 27 sec |
Round 1 Unable to complete |
|
|
|
Round 2 Score: 19/30 Time: 3 min 44 sec |
Round 2 Unable to complete |
Round 2 Unable to complete |
|
Child 3 |
Difficulty: Low Age: 16 Sex: Female |
Round 1 Score: 18/30 Time: 0 min 47 sec |
Round 1 Score: 18/30 Time: 2 mins 13 sec |
Round 1 Score: 19/30 Time: 2 mins 49 sec |
|
|
|
Round 2 Score: 28/30 Time: 0 min 50 sec |
Round 2 Score: 23/30 Time: 1 min 55 sec |
Round 2 Score: 26/30 Time: 1 min 31 sec |
|
Child 4 |
Difficulty: Low Age: 5 Sex: Male |
Round 1 Score: 16/30 Time: 2 mins 21 sec |
Round 1 Score: 17/30 Time: 4 mins 41 sec |
Round 1 Unable to complete |
|
|
|
Round 2 Score: 26/30 Time: 1 min 39 sec |
Round 2 Score: 19/30 Time:12 mins 12 sec |
Round 2 Unable to complete |
|
Child 5 |
Difficulty: Low Age: 4 Sex: Female |
Round 1 Score: 12/30 Time: 3 mins 14 sec |
Round 1 Score: 11/30 Time: 5 mins 22 sec |
Round 1 Unable to complete |
|
|
|
Round 2 Score: 14/30 Time: 3 mins 11 sec |
Round 2 Unable to complete |
Round 2 Unable to complete |
The summary data presents us with key metrics which are used to gain insight on the data retrieved from testing. These metrics include levels, rounds, age, sex, difficulty, score, and time. Levels and rounds are further grouped into a single metric called category with L1R1 indicating Round 1 Level 1 and vice versa.
Figure 5 shows the comparison between score by category and child. The chart shows an increase in scores at the second round of testing. This indicates that there was an improvement in the children’s ability to identify their drugs at the second trial. The average score of all five children increased from 16.2 over 30 – 23.4 at the first level. The average score of all three children that completed the second level increased from 19.7 over 30 –22.3. The average score of the two children that completed the third level increased from 20.5 over 30 – 26.5.
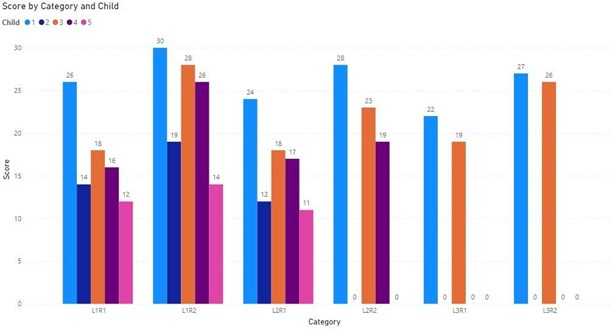
Figure 5. Comparison between score by category and child.
Figure 6 shows the comparison between time by category and child. The chart shows a decrease in time taken during the second round of testing. This indicates that there was an improvement in the children’s ability to identify their drugs faster at the second trial. The average time of all five children increased from 145.2 seconds (2 minutes 42 seconds) – 124.2 seconds (2 minutes 7 seconds) at the first level. The average time spent in both the second and third levels was reduced at the second trial. The chart also shows that as the levels increased, so also did time spent.
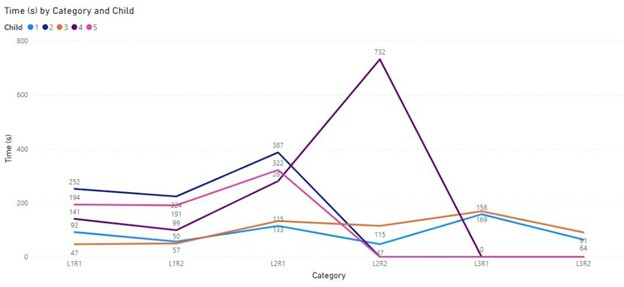
Figure 6. Comparison between time by category and child.
Figure 7 shows the comparison between round, time, and score. The chart shows an increase in scores at the second round of testing. This indicates that there was an improvement in the children’s ability to identify their drugs at the second trial.
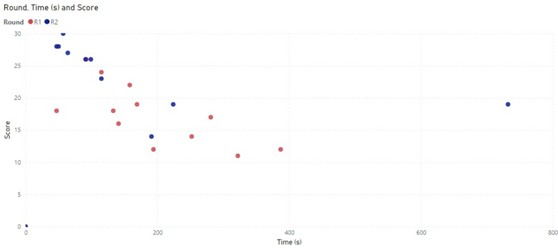
Figure 7. Comparison between round, time and score.
Figure 8 shows the comparison between scores by age. The chart shows both an increase and decrease in score as age increases. This indicates age is not necessarily a determinant factor in the children’s ability to identify their drugs.
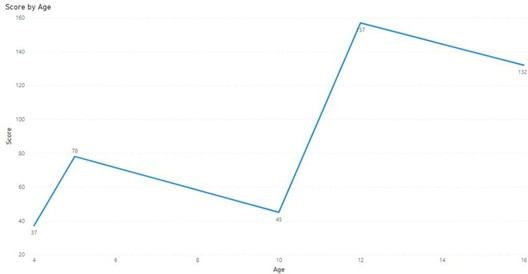
Figure 8: Comparison between score by age.
Figure 9 shows the comparison between time by age. The chart shows both an increase and decrease in time as age increases. This indicates age is not necessarily a determinant factor in the speed in which the children are able to identify their drugs.
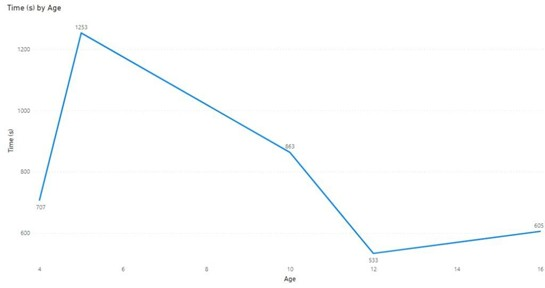
Figure 9. Comparison between time by age.
Figure 10 shows the comparison between time by sex and category. The chart shows the females achieved a higher score in a shorter time. This indicates that the females did better than the males.
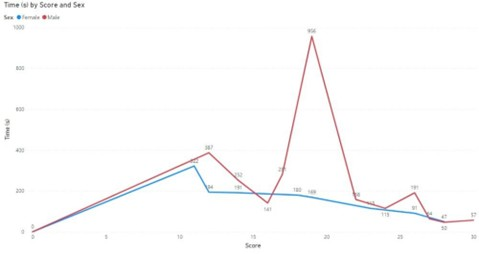
Figure 10. Comparison between time by sex and Score.
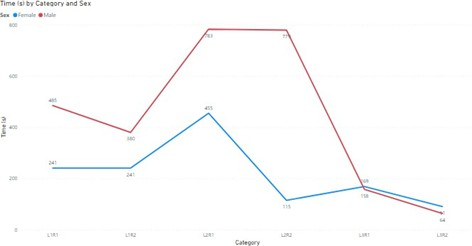
Figure 11. Comparison between time by sex and category.
Conclusion
The study has been able to successfully employ a design thinking approach to understand the requirements of children diagnosed with autism spectrum disorder. The approach has been able to create a human-centered technologically driven solution. Testing the proposed solution had shown an increase in the children’s ability to identify their drugs correctly and faster.
References
2. Cornett KA, Miora DS, Fass T, Dixon D. Memory Functioning for Personally Experienced and Witnessed Events in Children with Autism and the Implications for Educators, Mental Health Professionals, and the Law. Journal of Applied Research on Children. 2013;4(2):6.
3. Howe C, Eggett A, Old K, Davidson LA. Groupwork for Children with Autism Spectrum Disorder Ages 11-16: An Integrated Approach. Routledge; 2018 Oct 24.
4. Howlin P. Autism spectrum disorders. Psychiatry. 2006 Sep 1;5(9):320–4.
5. Stoppler M. Autism: Symptoms, Signs, Causes & Treatment. MedicineNet; 2019. Available from: https://www.medicinenet.com/autism_symptoms_and_signs/symptoms.htm.
6. Olanloye DO, Halleluyah OA, Ibitoye A, Emuoyibofarhe ON, John O. An Image Based Parkinson’s Disease Detection System Using Machine Learning Approach. Lautech Journal of Computing and Informatics. 2023 Aug 31;3(1):1–12.
7. Mandal A. Autism History. Autism History. 2014;9–10.
8. Mottron L. Autism spectrum disorder. Handb Clin Neurol. 2020;174:127-136.
9. Elmarakbi N, Robson H, Currie L. Creative Design Activities To Support The Complex Learning Enviroment Of The Classroom For Children With Autism Spectrum Disorder (ASD). In DS 117: Proceedings of the 24th International Conference on Engineering and Product Design Education (E&PDE 2022), London South Bank University in London, UK. 8th-9th September 2022.
10. Razzouk R, Shute V. What is design thinking and why is it important? Review of Educational Research. 2012 Sep;82(3):330–48.
11. Tonello L, Giacobbi L, Pettenon A, Scuotto A, Cocchi M, Gabrielli F, et al. Crisis Behavior in Autism Spectrum Disorders: A Self‐Organized Criticality Approach. Complexity. 2018;2018(1):5128157.
12. Yu Siang T, Friis Dam R. 5 Stages in the Design Thinking Process. Interaction Design Foundation; 2020 (accessed Feb. 01, 2021). Available from: https://ixdf.org/literature/article/5-stages-in-the-design-thinking-process.