Abstract
Background: Post-COVID syndrome (PCS) affects about 10% of COVID-19 patients, causing persistent symptoms such as chronic fatigue, cognitive impairments, and depression. These symptoms reduce quality of life and work capacity and are therefore targeted in specialized rehabilitation programs. A rehabilitation center in Germany developed a four-week group-based PCS rehabilitation program focusing on energy management. This study provides insights into PCS rehabilitation and evaluates both rehabilitants’ and employees’ satisfaction with the program, as well as suggestions for improvement.
Methods: This study follows a prospective observational design using a mixed-methods approach. PCS rehabilitants completed questionnaires at the beginning and end of rehabilitation, assessing, among other things, satisfaction with rehabilitation and aspects of the rehabilitation process. Survey responses were analyzed descriptively. Semi-structured interviews were conducted with six employees and eight rehabilitants to explore the satisfaction with the rehabilitation approach from both perspectives. Interviews were analyzed using a deductive-inductive content analysis.
Results: In total, we received at least one questionnaire from 128 of 147 rehabilitants (87.1%). Although responses varied regarding the achievement of personal rehabilitation goals and changes in general health, more than 77% of rehabilitants rated the rehabilitation overall as “very good” or “good”. Interview results confirmed general approval of the concept and its adaptation, though further improvements were suggested. Transfer of learned skills into daily life remained a key challenge.
Conclusions: The PCS rehabilitation concept appears to be a suitable and generally well-accepted setting for post-COVID rehabilitants. However, it requires a highly individualized approach. Key elements (should) include pacing, self-management, empathetic care, and stimulus reduction. Screening of the potential rehabilitants and stronger integration of the home environment after the rehabilitation are essential to ensure long-term sustainability of outcomes.
Keywords
Post-acute COVID-19 syndrome, Rehabilitation, Evaluation study, Health care surveys, Interview, Patient reported outcome measures, Fatigue, Return to work
List of Abbreviations
B-IPQ: Brief Illness Perception Questionnaire; CFIR: Consolidated Framework for Implementation Research; DRV: German Pension Insurance (“Deutsche Rentenversicherung“); DSQ-PEM: DePaul Symptom Questionnaire - Post-Exertional Malaise; EQ-VAS: EuroQol Visual Analogue Scale; EQ-5D-5L: European Quality of Life – 5 Dimensions – 5 Levels; FSMC: Fatigue Scale for Motor and Cognitive Functions; IMET: Index for Measuring Participation Restrictions; PCS: Post-COVID Syndrome; PHQ-4: Patient Health Questionnaire-4; SPE: Subjective Prognosis of gainful Employment
Introduction
After a COVID-19 infection, about 10% of patients develop post-COVID syndrome (PCS), characterized by persistent or recurring symptoms lasting more than 12 weeks that impair daily functioning [1–5]. Symptoms vary widely, including chronic fatigue, cognitive impairments, and depression, which significantly reduce quality of life and work ability [2,3,5]. Because there is currently no causal drug therapy available, and (acute) treatment options remain limited, medical rehabilitation is indicated [6]. Due to the high prevalence, the variety of symptoms, and the severity of symptoms, specialized rehabilitation programs are needed [2,3,5,7].
In Germany, medical rehabilitation is part of the healthcare system funded by health or pension insurance [8,9]. It aims at restoring functional capacity, participation in daily life, and work ability [10]. A rehabilitation center in Germany developed a specific PCS concept in which groups of about ten participants complete a four-week rehabilitation program. Rehabilitants’ satisfaction and treatment outcomes are well-established key criteria within the quality assurance program of the German Pension Insurance [10]. Given the novelty of the PCS concept, it is of particular interest to examine to what extent the concept fulfils these quality criteria. Beyond its relevance within the German rehabilitation system, it enhances understanding of patients’ experiences and perceived benefits of multidisciplinary post-COVID rehabilitation, while also informing quality assurance and the further development of rehabilitation programs. Moreover, the findings may offer transferable insights into effective treatment components of post-COVID rehabilitation of international relevance.
Therefore, this study aims to present insights into PCS rehabilitation, to examine satisfaction levels, and to provide suggestions for improvement from the perspective of rehabilitants and employees.
Methods
Design
This prospective observational study was designed as a mixed methods study. It includes questionnaire surveys among rehabilitants at two time points (T): at the beginning (T0) and end of rehabilitation (T1), as well as interviews with rehabilitants and employees (Figure 1).
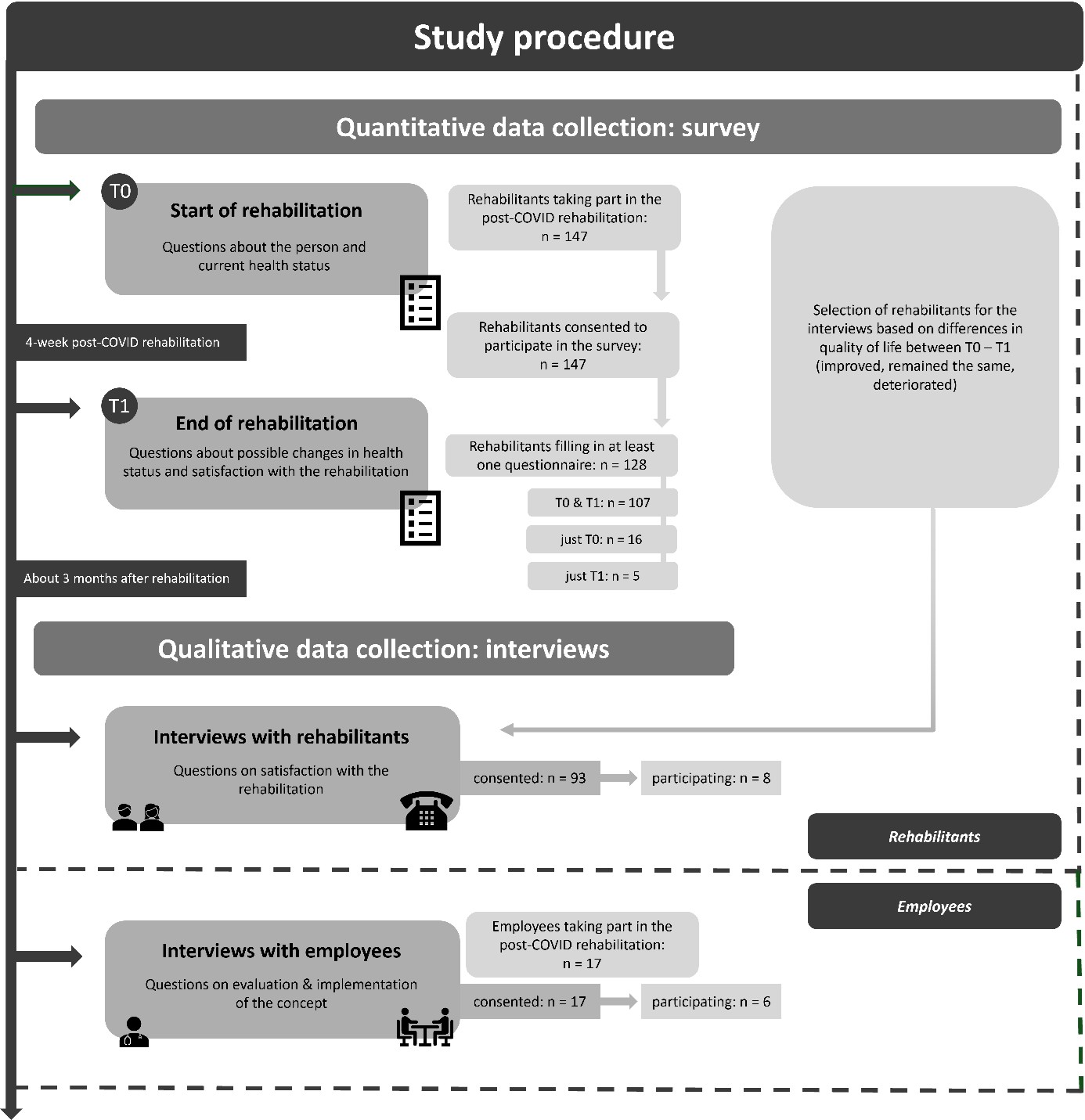
Figure 1. Study procedure.
Intervention
The four-week post-COVID rehabilitation program includes about ten rehabilitants starting and completing rehabilitation together, predominantly inpatient (or full-day outpatient). The focus is on energy management and pacing to aid self-management. Energy management and pacing are self-regulation strategies in which rehabilitants balance physical, cognitive, and emotional activity with adequate rest to avoid exacerbation of symptoms. Therapies for practicing energy management and pacing include e.g. occupational therapy (2 times per week, 30–60 minutes) and ergometer training (daily, 30 minutes). Therapy plans also include e.g. seminars on “COVID & Psyche” and “COVID & Cognition”. Further components of the rehabilitation plan can be found in the two sample treatment plans in the appendix (see Appendix I). Most therapies are group-based. Another feature is the principle of consistent therapists of whom one acts as contact person.
Participants
Patients suffering from PCS who had received approval from the German Pension Insurance for rehabilitation were able to begin their rehabilitation. Inclusion criteria for participation in the post-COVID rehabilitation program included, age ≥18 years, and key symptoms warranting referral. At the rehabilitation center referred to in the study, PCS rehabilitation as a standalone concept is part of the neurology department.
All rehabilitants taking part in the post-COVID rehabilitation were asked to participate in the survey.
Interviewees were selected based on changes in quality of life (EQ-VAS, range: 0–100) between the beginning (T0) and the end of rehabilitation (T1). If the score increased by one point or more from T0 to T1, these rehabilitants were classified as having improved (n=4, interviewees had increased scores of +26, +20, +17, and +17). If the score decreased by one point or more between T0 and T1, these rehabilitants were classified as deteriorated (n=2, interviewees had decreased scores of -20, and -5). If rehabilitants had exactly the same score at T0 and T1, they were classified as having remained the same (n=2, interviewees had 0 and 0). Due to limited financial resources (e.g., for expense reimbursements), the number of interviews was determined in advance in the project proposal. Four individuals who had improved were selected because it was assumed that this would allow us to determine what had helped them, and to identify potential areas for improvement for those who had deteriorated or remained unchanged. For practical reasons, the interviews were conducted in a concentrated period of time, which is why only four cohorts were eligible. Most importantly, however, no more than four months had passed since the rehabilitation, so that the memories could be as fresh as possible.
The selection of employees was drawn by occupational group to get different perspectives.
Because the PCS team at the rehabilitation center consists of only 17 members in total, the selection was limited. Where possible age and gender were taken into account.
Data collection
Questionnaires
Two questionnaires were developed for the measurement times T0 and T1 for this project. The final versions consisted of 76 items in total at T0 and 67 items in total at T1. Both questionnaires (T0 and T1) are structured in such a way that they consist of various instruments that have been compiled into a single questionnaire (see Table 1).
|
Topic(s) |
Instrument(s) |
Abbreviation(s) |
Reference |
T0 |
T1 |
|
Sociodemographic data |
--- * |
--- |
--- |
X |
|
|
Employment status |
Subjective prognosis of gainful employment |
SPE |
11 |
X |
X |
|
State of health / Quality of life |
European Quality of Life – 5 Dimensions – 5 Levels |
EQ-5D-5L |
12–14 |
X |
X |
|
Health impairments |
Index for Measuring Participation Restrictions Patient Health Questionnaire-4 |
IMET PHQ-4 |
15 16, 17 |
X X |
X |
|
Fatigue |
Fatigue Scale for Motor and Cognitive Functions |
FSMC |
18 |
X |
X |
|
Post-exertional malaise |
DePaul Symptom Questionnaire - Post-Exertional Malaise |
DSQ-PEM |
19, 20 |
X |
X |
|
Illness perceptions |
Brief Illness Perception Questionnaire |
B-IPQ |
21 |
X |
X |
|
Rehabilitation goals |
--- * |
--- |
--- |
X |
|
|
Aspects of the rehabilitation process |
Inpatient Somatic Care Questionnaire |
--- |
22 |
|
X |
|
* Created specifically for this study. |
|||||
In addition to demographic and employment-related questions, the paper-based questionnaires included validated German versions of standardized instruments assessing quality of life, health impairments, fatigue, post-exertional malaise, illness perceptions, rehabilitation goals, and aspects of the rehabilitation process [11–22].
Further, rehabilitants had the opportunity to describe suggestions of improvement for the rehabilitation concept in a free text section. This paper focuses on all aspects of the rehabilitation process including satisfaction, while results on rehabilitation outcomes are to be published elsewhere.
Data collection was conducted between October 2023 and December 2024. English versions of the questionnaires are available in the appendix (see Appendix II & III).
Outcomes and operationalization
Rehabilitation goals and rehabilitation process
The questionnaire covered aspects such as the rehabilitation plan and goals, as well as rehabilitants’ satisfaction with and evaluation of the overall rehabilitation experience. To assess the rehabilitation process, the survey included questions about the quality and extent of services received. Therefore, parts of a questionnaire on rehabilitation quality from the German Pension Insurance were used [22].
Interviews
Semi-structured individual interviews were conducted with employees and rehabilitants. Employees were interviewed at the rehabilitation center during working hours in August 2024 without compensation regarding the implementation of the rehabilitation concept. Information such as occupational group, age, and gender was documented.
Rehabilitants were invited to share their personal experiences of the program. Due to the wide geographic distribution of rehabilitants' residences, interviews were conducted via telephone within three months after rehabilitation, in September and October 2024. Rehabilitants received a 30-euro allowance for participation.
Two interview guides were created for this study (see Appendix IV & V). The interviews were conducted by research staff members of the study’s project team. The interviewers are not employed at the rehabilitation center and have experience conducting interviews. All interviews were audio-recorded and pseudonymously transcribed.
Data analysis
Questionnaires
Participant characteristics and survey responses were analyzed descriptively using absolute and relative frequencies for categorical variables. All analyses were conducted using IBM SPSS Statistics, Version 29 (IBM Corp., Armonk, NY, USA).
Rehabilitants had the opportunity to express suggestions for improvement in free text sections of the T0 and T1 questionnaires. These responses were clustered.
Interviews
We employed a combined deductive-inductive content analysis approach based on Kuckartz and Rädiker (2022) with MAXQDA 24, a software program used in research for qualitative and mixed-methods data analysis [23,24]. Initially, the five main categories were developed deductively from the Consolidated Framework for Implementation Research (CFIR): 1. characteristics of the concept, 2. environment, 3. location, 4. characteristics of those involved, and 5. implementation process [25]. Subcategories were then formed inductively, with the coding scheme being continuously refined. Two researchers were involved throughout the analysis. Portions of the data were coded independently and discrepancies discussed in consensus meetings. In case there were disagreements at a consensus meeting, a third researcher was brought in. The final category system was defined with detailed descriptions and anchor examples (see Appendix VI). Reporting followed the COREQ and STROBE checklists [26].
Ethics and data security
The study has been approved by the responsible Medical Ethics Committee (No. 2023-148). All participants provided informed consent. All data were pseudonymized before data handling.
Results
Questionnaires
Response proportions and responder characteristics
Of the 147 rehabilitants taking part in the post-COVID rehabilitation 128 (87.1%) filled in at least one questionnaire (T0, T1, or both), while 107 out of 147 (72.8%) rehabilitants filled in both, the T0 and T1 questionnaire. As not all rehabilitants answered every question, the percentages in the tables (and in the text) refer to the group size mentioned in the title of the table.
Mean age of the rehabilitants was about 50 years (range: 21–68 years) and two third (67.8%, n=82) were female (Table 2). Almost 70% suffered from pre-existing disease (66.9%, n=79). Most commonly named pre-existing diseases were obesity (“yes”: 29.5%, n=36), heart disease (“yes”: 23.8%, n=29), and mental illness (“yes”: 23.0%, n=28) and lung disease (“yes”: 23.0%, n=28).
|
Variable |
Characteristics |
n (%) |
|
Age (in years) (n=120) |
Mean (SD) Range |
49.4 (11.3) 21–68 |
|
Gender (n=121) |
Female Male Diverse |
82 (67.8) 37 (30.6) 2 (1.7) |
|
Job training (n=119) |
No formal professional qualification Apprenticeship Advanced vocational school / Technical college University (of applied sciences) |
4 (3.4) 71 (59.7) 22 (18.5) 22 (18.5) |
|
Persons in household (n=117) |
1 2 3 4 5 or more |
30 (25.7) 52 (44.4) 15 (12.8) 14 (12.0) 6 (5.2) |
|
Pre-existing disease (n=118) |
Yes No |
79 (66.9) 39 (33.1) |
|
Rehabilitation basis (n=127) |
Inpatient All-day outpatient |
120 (94.5) 7 (5.5) |
|
a numbers (%) of participants. Numbers differ per variable, due to missing values. |
||
Rehabilitant’s feedback on the post-COVID rehabilitation concept
Table 3 shows rehabilitants’ answers on questions concerning the post-COVID rehabilitation concept. More than half of the rehabilitants (54.1%, n=60) stated that the care and the treatments they received during rehabilitation were just right for them. Two thirds (“rather yes” or “yes”: 67.9%, n=76) agreed that the rehabilitation center had the right care, treatments, and advice for their complaints. Answers concerning achieving your personal rehabilitation goals with the help of the rehabilitation program, show one third each: "no" and "rather no": 35.7%, n=36; "partly": 33,7%, n=34; "yes" and "rather yes": 30.7%, n=31. This also applies to the extent your overall health state changed as a result of the rehabilitation ("strongly deteriorated" and "deteriorated": 35.7%, n=40; "remained the same": 33.9%, n=38; "strongly improved" and "improved": 30.4%, n=34). The timing of the rehabilitation stay in relation to the recovery process was as “far too late” or “too late” by more than half of the rehabilitants (50.9%, n=31) assessed. Three quarters of the rehabilitants (77.0%, n=87) rated the rehabilitation program as “very good” or “good”.
|
Question
|
Categories (n (%)) |
|
||||
|
Far too little |
Too little |
Just right |
Too much |
Far too much |
n= |
|
|
How would you rate the scope of the services (care, treatments and counseling) during rehabilitation? The care and my treatments at the rehabilitation clinic were… |
1 (0.9) |
19 (17.1) |
60 (54.1) |
26 (23.4) |
5 (4.5) |
111 |
|
|
No |
Rather no |
Partly |
Rather yes |
Yes |
|
|
How would you rate the quality of the services (care, treatments and counseling) during rehabilitation? The rehabilitation clinic had the right care, treatments and advice for my complaints. |
2 (1.8) |
5 (4.5) |
29 (25.9) |
35 (31.3) |
41 (36.6) |
112 |
|
My physicians and therapists discussed the goals of my rehabilitation with me right at the beginning. |
6 (5.3) |
8 (7.1) |
28 (24.8) |
32 (28.3) |
39 (34.5) |
112 |
|
My physicians and therapists discussed with me which treatments are best suited to achieve my rehabilitation goals. |
5 (4.5) |
19 (17.1) |
31 (27.9) |
29 (26.1) |
27 (24.3) |
111 |
|
My physicians and therapists have encouraged me to deal with the consequences of my illness for my private and professional life. |
0 (0.0) |
7 (6.9) |
24 (23.8) |
24 (23.8) |
46 (45.5) |
101 |
|
My physicians and therapists have shown me how I can better deal with the consequences of my illness for my private and professional life. |
0 (0.0) |
12 (10.7) |
24 (21.4) |
35 (31.3) |
41 (36.6) |
112 |
|
My physicians and therapists have asked me about possible psychological problems in connection with my illness and its treatment. |
7 (6.3) |
16 (14.3) |
24 (21.4) |
26 (23.2) |
39 (34.8) |
112 |
|
Do you think you have achieved your personal rehabilitation goals with the help of the rehabilitation program? |
14 (13.9) |
22 (21.8) |
34 (33.7) |
22 (21.8) |
9 (8.9) |
101 |
|
|
Strongly deteriorated |
Deteriorated |
Remained the same |
Improved |
Strongly improved |
|
|
In what way has your overall state of health changed as a result of rehabilitation? |
9 (8.0) |
31 (27.7) |
38 (33.9) |
27 (24.1) |
7 (6.3) |
112 |
|
|
Far too early |
Too early |
Just right |
Too late |
Far too late |
|
|
How do you rate the timing of your stay in rehabilitation in relation to your recovery process? b |
0 (0.0) |
6 (9.8) |
24 (39.3) |
22 (36.1) |
9 (14.8) |
61 |
|
|
Very bad |
Bad |
Partly |
Good |
Very good |
|
|
How would you rate the rehabilitation program overall? |
1 (0.9) |
3 (2.7) |
22 (19.5) |
59 (52.2) |
28 (24.8) |
113 |
|
a Numbers (%) of participants. Numbers differ per variable, due to missing values. b Question was added to the questionnaire at a later point in time. |
||||||
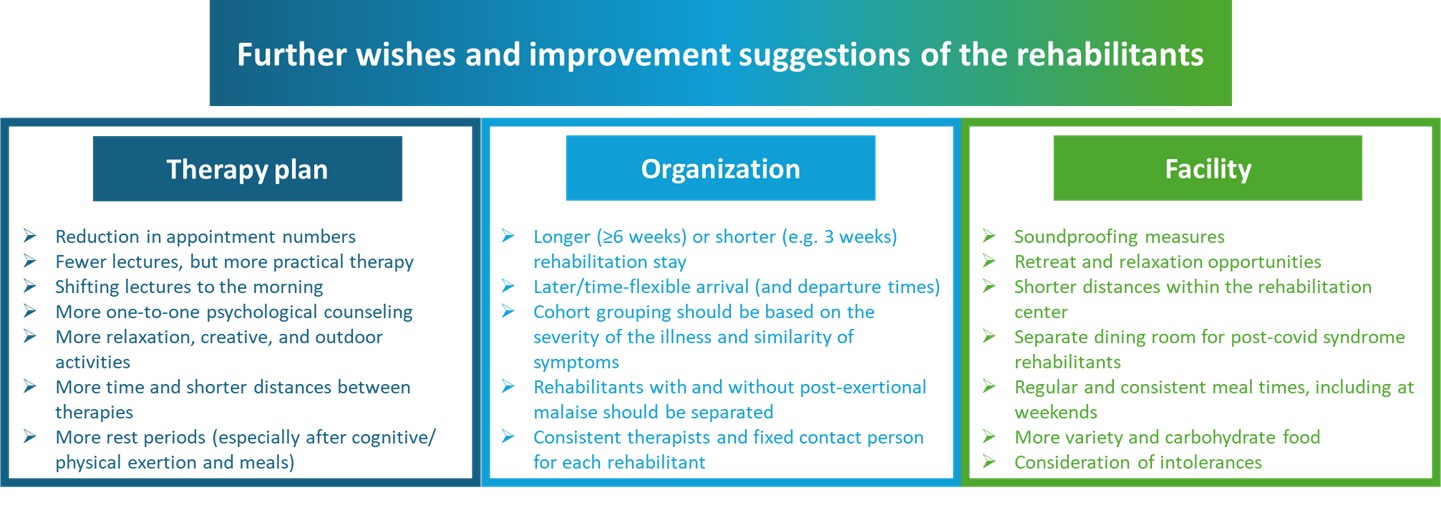
In addition, rehabilitants had the opportunity to express further wishes and suggestions for improvement in free text sections of the T0 and T1 questionnaires. Answers were described in Figure 2. For clarity, the responses were clustered. This resulted in three relevant key topics.
Interviews
Interviews lasted 31.2 (employees) and 36.5 (rehabilitants) minutes on average. The employees had a mean age of 43.3 years (range: 26–62 years), with women making up 66.7% of the group (n=4). Employees from different professions (neurology, psychology, physiotherapy, occupational therapy, nursing, and administration) participated. The rehabilitants averaged 41.8 years (range: 21–59 years), with 75.0% female (n=6). The results are presented according to the CFIR ([25], Table 4).
|
Characteristics of the concept |
Environment of the concept |
Location of the concept |
Characteristics of those involved in the concept |
Implementation process of the concept |
|
Concept adaptation Concept is continuously adapted in order to match the specific needs and wishes of the rehabilitants.
Concept feedback Employees received positive feedback with regard to the concept from the rehabilitants. The rehabilitants mentioned the challenge to apply the learned into everyday life. |
Society The environment is not fully post-COVID sensitized, which makes the implementation of the learned into everyday life difficult for the rehabilitants
Cost units Long waiting times for rehabilitation places causes expired cost coverages, which requires a reprocessing of the cost coverages.
Medical / therapeutic care Rehabilitants mentioned a lack of post-COVID-specific offers and that there is a lack of knowledge about the post-COVID syndrome. |
Employees The employees were praised for the empathy by the rehabilitants. The nursing staff were criticized for a lack of understanding. The changes in therapists (e.g. due to vacation/illness) were also denounced.
General conditions Employees criticized a lack of resources (time, rooms). The rehabilitants judged the arrival and departure modalities as badly, as well as the catering, long distances, and a lack of quiet rooms. In contrast, later breakfast times, separate dining rooms, ground-floor accommodation, blackout curtains, and chair glides were praised. |
Rehabilitants Rehabilitants found it difficult to implement what they have learned in rehabilitation into everyday life.
Post-COVID-Team Employees were motivated to adapt the concept. They were seen as competent and empathetic, which was praised by the rehabilitants. |
Time / eligibility of rehabilitation1 The right rehabilitation time is difficult to estimate and opinions differ about the optimal time. A pre-rehabilitation screening could be a solution, also to better address rehabilitation eligibility and thus be able to implement the concept more effectively.
Capacities & resources Employees described limited places for therapies and a lack of time. |
|
1 In order to implement the rehabilitation concept (successfully), the right rehabilitation time, as well as the rehabilitant's eligibility to undergo rehabilitation, must be determined. If rehabilitants participate in the program at an inappropriate time, they are not able to actively engage in rehabilitation and rehabilitation will not be successful. a Cursive only reported by rehabilitants - Underlined only reported by employees |
||||
Characteristics of the concept
Concept adaptation
The employees reported that the PCS concept is continuously being adapted in order to respond to the wishes, needs, and requirements of the rehabilitants.
“At some point, I heard a sentence, ’we're building the plane while flying it’. And that’s how it is.” (116)
Examples of improvements included the revision of a PCS rehabilitation flyer, later breakfast times, blackout curtains in rehabilitant rooms, and reducing dining room noise with felt chair glides. These were praised by the rehabilitants. Most importantly employees reported that many individualized therapy plan adjustments were made, requiring significant effort.
Therapies were rescheduled or supplemented (e.g., more heat treatment) and physician rounds were extended. However, neuropsychological diagnostic sessions were shortened from 90 to 60 minutes due to rehabilitant fatigue. Overall, the employees perceived a constant need for adaptation.
Concept feedback
The employees reported that they predominantly received positive feedback from the rehabilitants and that they were satisfied that such a rehabilitation exists.
"And like I said, the patients are, for the most part, very, very happy to be here." (112)
In Addition, the employees described that many rehabilitants specifically wanted to come to the rehabilitation center due to its good reputation. However, some rehabilitants might be dissatisfied. The employees identified the challenge that the rehabilitation does not correspond to the everyday life of the rehabilitants.
"Everyday life is not rehabilitation. Simulating that is also difficult." (114)
Feedback on the rehabilitation concept among rehabilitants varied. Some would not recommend the concept due to lack of health improvement and excessive demands causing setbacks. A lack of individual psychological support was mentioned negatively and overall, a desire for more individualized rehabilitation was expressed.
"Yeah, then the rehabilitation plans themselves. For me it felt like they could maybe be a little more tailored to each person's, yeah, symptoms." (126)
Furthermore, group constellations of two rehabilitants were sometimes problematic because of different performance levels. However, most rehabilitants appreciated the group format, valuing peer exchange. Another aspect that rehabilitants mentioned positively was the support provided by the therapists during the therapies. Seminars were perceived as helpful.
Environment of the concept
Society
Because society is not fully sensitized to the topic of PCS, it is sometimes difficult for the rehabilitants to implement what they have learned in rehabilitation at home.
"At home, it is often the case that, because you simply cannot see it [PCS], you are misunderstood." (23)
Therefore, it was suggested to create routines and to encourage exchange with peers. In order to cope well with the illness, it is important for the rehabilitants to sensitize their environment and create acceptance. Another wish was to inform employers and relatives about PCS.
Cost units
With regard to the interaction with the cost units (German Pension Insurance), it was reported by both employees and rehabilitants that, due to the long waiting times, cost coverage has in some cases expired, requiring additional effort to extend or modify it.
Medical and therapeutic care
Rehabilitants reported that medical and therapeutic care at home is challenging. Difficulties included insufficient (PCS-specific) services and a lack of training and awareness of PCS among physicians and therapists.
Location of the concept
Employees
Rehabilitants praised the competent, empathetic physicians and therapists who provided realistic assessments. Criticism was directed at nursing staff for a perceived lack of understanding, and changes in therapists were also seen as challenging. Besides, the cleaning staff were criticized for the cleanliness of the facilities by the rehabilitants.
General conditions
The arrival and departure procedures, which were very time-consuming, as well as catering, were criticized by the rehabilitants. A more flexible and quieter arrival and admission situation could reduce stress. Long distances within the rehabilitation center were noted.
"Well, I mean, personally, I find the distances really far." (122)
Characteristics of those involved in the concept
Rehabilitants
Pacing and energy management were taught during rehabilitation and were considered very important by the rehabilitants. Besides, the employees perceived a higher level of knowledge among those affected (compared to the first PCS rehabilitation cohorts). Sometimes this exceeds the employees’ scope of competence.
"Lately, we’ve been noticing more and more that the people affected have an extremely high level of knowledge. They really know their stuff and they also want very specific, expert answers from us." (116)
PCS team
Employees initially had to acquire PCS-specific knowledge independently due to the new condition, with many eager to improve and learn. In addition, all employees were motivated to adapt and further develop the concept.
“[...] but I think this team is especially productive and incredibly fast in adapting the concept. And everyone has good ideas, and yeah, it's kind of like swarm intelligence.” (116)
Although the rehabilitants described the physicians and therapists as being very competent and empathetic, as well as honest and supportive, some rehabilitants expressed dissatisfaction with certain staff members.
Implementation process of the concept
Time of rehabilitation/ eligibility for rehabilitation
On the part of the employees, the associated difficulty in estimating the right time for rehabilitation, were named above all.
"And it's always such a fine tightrope act — are they fit for rehabilitation, yes or no? Will they benefit from it?" (116)
This was also mentioned by the rehabilitants, but they disagreed on how they felt about the timing of rehabilitation. Some found it to be too late, others just right or too early. Employees thought it might be helpful to screen rehabilitate eligibility. This could enable rehabilitants to benefit optimally from the rehabilitation.
Capacities and resources
Capacity problems (limited rehabilitation places) and resources constraints (such as time and space capacities) played a decisive role for the employees, because they have an impact on the implementation of the therapies.
Discussion
This study presents insights into a newly developed PCS rehabilitation concept, examines satisfaction levels of the rehabilitants and employees, and provides improvement suggestions for PCS rehabilitation concepts.
Questionnaire results show that over 77% rated the rehabilitation as “very good” or “good”, overall. A heterogeneous picture emerged with regard to the achievement of personal rehabilitation goals and the change in general health status. Interview results show that rehabilitants are generally satisfied with the rehabilitation concept and its ongoing adaptation, although further adjustments were necessary. For the rehabilitants it is particularly challenging to transfer the skills learned during rehabilitation into everyday life.
Specification of the rehabilitation concept
The rehabilitation concept has been continuously adapted to the specific needs of PCS rehabilitants, which differ significantly from classic rehabilitative indications [27]. Instead of functional gain as e.g. in neurological rehabilitation settings [28], pacing, self-management strategies, activity reduction, and sufficient rest periods become central and are already part of the PCS concept. Structural factors (e.g., short distances within the rehabilitation center), opportunities for retreat between therapies and after meals, and a less stimulating environment (e.g., lower noise level) are components of a disease-specific setting and were mentioned by the rehabilitants. Such a specification of a rehabilitation setting was also found in a study on rehabilitation needs in COVID-19 survivors and has proven successful for this patient group [29]. Empathy and (disease-related) understanding of the PCS are also relevant. While the empathetic attitude of employees was highlighted positively, a lack of understanding was negatively rated by rehabilitants. Continuity and disease-specific trainings are essential for all employees.
Not all affected individuals benefited equally from rehabilitation, while other studies generally stated that those affected benefit [30]. The heterogeneous perception of the optimal time for rehabilitation and the partial lack of subjective improvement that were reported, argue for the need of screening [29,31]. This should assess both resilience and rehabilitation goals [32] in order to identify those rehabilitants who can benefit from rehabilitation and, if necessary, refer others to alternative care structures.
Discrepancy between rehabilitation setting and home environment
Rehabilitants reported, that transferring pacing strategies to everyday life is challenging. This discrepancy between the protected rehabilitation setting and the often poorly adapted home environment represents a significant obstacle to sustainable effects. Family members, employers, and other persons (e.g. health care providers) often have insufficient knowledge about PCS [33], especially invisible symptoms (e.g. fatigue). This can lead to a lack of understanding [33–35]. That might explain why rehabilitants reported that they want their relatives and employers to be better informed about the PCS, so that they can better support them.
In addition, many regions lack outpatient PCS-specific services that enable continuous support [34]. It seems sensible to supplement rehabilitation programs with structured educational materials for relatives and employers. Structured aftercare programs should be considered to support rehabilitants after discharge (e.g. telephone or digital follow-ups), support groups, or online coaching on self-management [36–38]. The study by Müller et al. (2025) also highlights the importance of an aftercare program, for example, to support self-management skills [36].
Strengths and limitations
One key advantage was the mixed methods approach. Questionnaire data helped identify rehabilitants with different rehabilitation experiences, and interviews offered valuable insights into the rehabilitation (process).
With a response proportion of 87% in the survey and a high participation willingness in interviews, a substantial proportion of rehabilitants were represented. Otherwise, it may reflect the high level of suffering of rehabilitants.
The possibility of selection bias cannot be entirely dismissed, as those with the most severe impairments might have been unable to take part. Furthermore, the selection of interview participants is limited to a small number of cohorts of rehabilitation patients and, among staff members, to the PCS team. Also, one rehabilitant selected for an interview was based on a deterioration of -5 (EQ-VAS, T0 and T1) which is below the minimal clinically important difference. The selection of interviewees may have resulted in selection bias, too.
Although the research was conducted within a single rehabilitation center, which may limit its generalizability, participants came from various parts of Germany. The variance among rehabilitants allows to gain helpful insights into a specific rehabilitation program of a novel disease, also relevant for the international rehabilitation audience.
Although evaluating intervention outcomes was not the primary objective of this study, it is notable that almost 36% of participants experienced deterioration in health status. This contrasts with the generally positive program ratings, with 77% evaluating the rehabilitation program as “good” or “very good” and only 3.6% as “very poor” or “poor”. Future research could examine whether the observed deterioration in condition was associated with dissatisfaction with the program.
Conclusion
PCS rehabilitation is a suitable and generally positively rated setting for post-COVID rehabilitants. At the same time, an indication-specific, highly individualized approach is required, which clearly differs from classic rehabilitation concepts. Key elements should include pacing, self-management, empathy, and stimulus reduction. In addition, screening is needed to identify suitable rehabilitants, and rehabilitation and the home environment need to be more closely integrated to ensure the sustainability of the rehabilitation interventions.
Funding
The study “Post-COVID Rehabilitation am Reha-Zentrum Oldenburg – Weiterentwicklung und Bewertung der Wirksamkeit des Post-COVID Rehabilitationskonzepts (Post-COVID Reha)” is funded by the German Pension Insurance Oldenburg-Bremen (DRV) (060.008.01.00-3.050).
Ethics and Data Security
The study has been approved by the responsible Medical Ethics Committee. All participants provided informed consent. All data were pseudonymized before data handling.
Declaration of Competing Interests
AH and NSch are employees of the German Pension Insurance Oldenburg-Bremen (DRV). CU, MF, and JH are employees of the Rehabilitation Center Oldenburg. The other authors declare that they have no competing interests.
Acknowledgements
The authors would like to thank all PCS-affected rehabilitants, as well as the employees of the Rehabilitation Center Oldenburg, for their participation in this project and study. We also extend our sincere thanks to Dorian Louis Noll and Carina Köpcke for their valuable support in this study.
References
2. Pavli A, Theodoridou M, Maltezou HC. Post-COVID Syndrome: Incidence, Clinical Spectrum, and Challenges for Primary Healthcare Professionals. Arch Med Res. August 2021;52(6):575–81.
3. Scharf RE, Anaya JM. Post-COVID Syndrome in Adults-An Overview. Viruses. March 2023;15(3):675.
4. Sk Abd Razak R, Ismail A, Abdul Aziz AF, Suddin LS, Azzeri A, Sha’ari NI. Post-COVID syndrome prevalence: a systematic review and meta-analysis. BMC Public Health. July 2024;24(1):1785.
5. Tenforde MW, Kim SS, Lindsell CJ, Billig Rose E, Shapiro NI, Files DC, et al. Symptom Duration and Risk Factors for Delayed Return to Usual Health Among Outpatients with COVID-19 in a Multistate Health Care Systems Network - United States, March-June 2020. MMWR Morb Mortal Wkly Rep. July 2020;69(30):993–8.
6. National Institute for Health and Care Excellence (NICE). COVID-19 rapid guideline: managing the long-term effects of COVID-19. [Internet]. London: NICE; 2020 [11. February 2026]. Available at: https://www.nice.org.uk/guidance/ng188
7. Ahmad M, Kim K, Indorato D, Petrenko I, Diaz K, Rotatori F, et al. Post-COVID Care Center to Address Rehabilitation Needs in COVID-19 Survivors: A Model of Care. Am J Med Qual. 2022 May-Jun 01;37(3):266–71.
8. Deutsche Rentenversicherung (DRV). Rehabilitation [Internet]. Berlin: Deutsche Rentenversicherung; 2025 [cited 2026 May 19]. Available at: https://www.deutsche-rentenversicherung.de/DRV/DE/Reha/reha_node.html
9. Kladny B. Inpatient and outpatient rehabilitation in Germany. Current state and further development. Unfallchirurg. 2015 Feb;118(2):103–11.
10. Deutsche Rentenversicherung (DRV). Grundlagen, Ziele und Dimensionen [Internet]. Berlin: Deutsche Rentenversicherung; 2025 [15. January 2026]. Available at: https://www.deutsche-rentenversicherung.de/DRV/DE/Experten/Infos-fuer-Reha-Einrichtungen/Grundlagen-und-Anforderungen/Reha-Qualitaetssicherung/grundlagen_ziele_dimensionen.html
11. Mittag O, Raspe H. A Brief Scale for Measuring Subjective Prognosis of Gainful Employment: Findings of a Study of 4279 Statutory Pension Insurees Concerning Reliability (Guttman Scaling) and Validity of the Scale. Rehabilitation (Stuttg). June 2003;42(3):169–74.
12. Herdman M, Gudex C, Lloyd A, Janssen M, Kind P, Parkin D, et al. Development and preliminary testing of the new five-level version of EQ-5D (EQ-5D-5L). Qual Life Res. December 2011;20(10):1727–36.
13. Ludwig K, Graf von der Schulenburg JM, Greiner W. German Value Set for the EQ-5D-5L. Pharmacoeconomics. June 2018;36(6):663–74.
14. EuroQol Group. EuroQol - a new facility for the measurement of health-related quality of life. Health Policy. December 1990;16(3):199–208.
15. Deck R, Mittag O, Hüppe A, Muche-Borowski C, Raspe H. [IMET - Index for the Assessment of Health Impairments]. January 2011. In: Leibniz-Zentrum für Psychologische Information und Dokumentation (ZPID) (Publisher), Elektronisches Testarchiv. Trier: ZPID.
16. Löwe B, Wahl I, Rose M, Spitzer C, Glaesmer H, Wingenfeld K, et al. A 4-item measure of depression and anxiety: validation and standardization of the Patient Health Questionnaire-4 (PHQ-4) in the general population. J Affect Disord. April 2010;122(1–2):86–95.
17. Kroenke K, Spitzer RL, Williams JBW, Löwe B. An ultra-brief screening scale for anxiety and depression: the PHQ-4. Psychosomatics. 2009;50(6):613–21.
18. Penner IK, Raselli C, Stöcklin M, Opwis K, Kappos L, Calabrese P. The Fatigue Scale for Motor and Cognitive Functions (FSMC): validation of a new instrument to assess multiple sclerosis-related fatigue. Mult Scler. December 2009;15(12):1509–17.
19. Cotler J, Holtzman C, Dudun C, Jason LA. A Brief Questionnaire to Assess Post-Exertional Malaise. Diagnostics (Basel). September 2018;8(3):66.
20. Kuczyk C, Nöhre M, Herrmann-Lingen C, Stolz M, Krauth C, Brähler E, et al. Reliability and validity of the German version of the DePaul Symptom Questionnaire Post-Exertional Malaise (DSQ-PEM). Front Psychiatry. September 2025;16.
21. Broadbent E, Petrie KJ, Main J, Weinman J. The Brief Illness Perception Questionnaire. J. Psychosom. Res. June 2006; 60(6):631–7.
22. Deutsche Rentenversicherung (DRV). Rehabilitandenfragebogen für die ganztägige stationäre Rehabilitation mit somatischem Behandlungsschwerpunkt [Internet]. Berlin: Deutsche Rentenversicherung; 2024 [11. February 2026]. Available at: https://www.deutsche-rentenversicherung.de/SharedDocs/Downloads/DE/Experten/infos_reha_einrichtungen/quali_rehabilitandenbefragung/indikationsbereiche/2024-fragebogen-ganztaegig-stat-reha-somatisch.html
23. Kuckartz U, Rädiker S. Qualitative content analysis: methods, practice and software. 2nd ed. Los Angeles, London, New Delhi, Singapore, Washington DC, Melbourne: SAGE; 2023. p. 263.
24. Software VERBI. MAXQDA. 2024.
25. Waltz TJ, Powell BJ, Fernández ME, Abadie B, Damschroder LJ. Choosing implementation strategies to address contextual barriers: diversity in recommendations and future directions. Implement Sci. April 2019;14(1):42.
26. The EQUATOR Network. Enhancing the QUAlity and Transparency Of health Research (EQUATOR Network): Reporting guidelines for main study types [Internet]. 2021. [18. February 2026]. Available at: https://www.equator-network.org/reporting-guidelines/
27. Wade DT. Goal setting in rehabilitation: an overview of what, why and how. Clin Rehabil. April 2009;23(4):291–5.
28. Bode RK, Heinemann AW. Course of functional improvement after stroke, spinal cord injury, and traumatic brain injury. Arch Phys Med Rehabil. January 2002;83(1):100–6.
29. Ahmad M, Kim K, Indorato D, Petrenko I, Diaz K, Rotatori F, et al. Post-COVID Care Center to Address Rehabilitation Needs in COVID-19 Survivors: A Model of Care. Am J Med Qual. 2022;37(3):266–71.
30. Hayden MC, Limbach M, Schuler M, Merkl S, Schwarzl G, Jakab K, et al. Effectiveness of a Three-Week Inpatient Pulmonary Rehabilitation Program for Patients after COVID-19: A Prospective Observational Study. Int J Environ Res Public Health. August 2021; 18(17):9001.
31. Jöbges M, Tempfli M, Kohl C, Herrmann C, Kelm S, Kupferschmitt A, et al. Neuropsychological outcome of indoor rehabilitation in post-COVID-19 condition-results of the PoCoRe study. Front Neurol. 2024;15:1486751.
32. Salzmann S, Herrmann M, Henning M, Schwertner L, Euteneuer F, Goldau L, et al. Side-effect expectations are associated with disability, physical fitness, and somatic symptoms 3 months after post-COVID neurological inpatient rehabilitation. J Psychosom Res. November 2024;186:111902.
33. Leiße A, Yilmaz-Aslan Y, Neugebauer T, Erdogdu IÖ, Bakan AS, Sultanoglu B, Führer AG, Brzoska P. COVID-19-related disease perceptions in the population of Turkey – results of a cross-sectional study. Das Gesundheitswesen. 2022 Aug;84(08/09):V-170.
34. Hammer S, Monaca C, Hoelz A, Tannheimer M, Baumgart SH, Dornieden K, et al. “Ultimately, you are on your own.” A qualitative analysis of barriers to health care from the perspective of patients with long COVID. Journal for Evidence, Continuing Education and Quality in Healthcare. April 2025;193:8–17.
35. Schmachtenberg T, Königs G, Dragaqina A, Roder S, Müller F, Müllenmeister C, et al. “There is no one who helps you with it”: experiences of people with long COVID regarding medical care, therapeutic measures, and barriers in the German healthcare system: results of a qualitative study with four focus groups. BMC Health Serv Res. 26. October 2023;23(1):1160.
36. Müller K, Poppele I, Ottiger M, Weber RC, Stegbauer M, Schlesinger T. Course of neuropsychological health in post-COVID patients differs 6 and 12 months after inpatient rehabilitation. Front Psychiatry. April 2025;16.
37. Stucke J, Neudecker S, Meier I, Meyer-Feil T. Illness experiences, problems and needs of patients with post-COVID syndrome: What can we learn for medical rehabilitation?. Rehabil. April 2025;64(2):92–100.
38. Deck R, Schramm S, Hüppe A. Supported Own Initiative of Rehabilitation Patients (“New Credo”) – A Successful Model?. Rehabil. October 2012;51(5):316–25.