Abstract
As people with HIV (PWH) age with improved antiretroviral therapy (ART), understanding health outcomes in cohabiting couples whether seroconcordant or serodiscordant has become increasingly important for comprehensive HIV care. This study investigated viral load suppression rates, hypertension, and diabetes prevalence among HIV-infected individuals in seroconcordant and serodiscordant cohabiting relationships and identified demographic and clinical factors associated with these outcomes. This hospital-based study analyzed 247 adults (>18 years) with HIV, comprising 176 individuals from seroconcordant couples and 71 HIV-infected individuals from serodiscordant couples. Participants' mean age was 47.59 ± 10.61 years, with a mean ART duration of 13.29 ± 5.43 years. The overall viral suppression rate was 97.6%, while hypertension prevalence was 9.3% and diabetes prevalence was 2.8%. Enhanced adherence counselling (EAC) for prior virologic failure was provided for 6.5% of participants. Concordance status did not significantly affect viral suppression (p = 0.7) or hypertension prevalence (p=0.8). However, seroconcordant couples had significantly longer ART duration (14.02 vs 11.24 years, p<0.001), while serodiscordant couples had longer cohabitation duration (20.83 vs 17.99 years, p=0.033). Despite excellent overall suppression, participants on second-line ART regimens had 93% lower odds of viral suppression compared to first-line recipients [adjusted odds ratio (aOR)=0.07, 95% confidence interval (CI): 0.01–0.76, p=0.028]. Those with a history of EAC had similarly reduced suppression odds of viral suppression (aOR=0.11, 95% CI: 0.01–0.94, p=0.044). Male sex and higher body mass index were independent predictors (aOR=3.13, 95% CI: 1.15–9.09, p=0.025 and aOR=1.12, 95% CI: 1.02–1.23, p=0.014, respectively). These findings underscore that partner HIV status does not influence clinical outcomes but highlight important needs for sustained adherence support in patients with complex treatment histories and targeted cardiovascular risk management in the ageing population of PWH.
Keywords
Seroconcordant, Serodiscordant, HIV, Viral suppression, Adherence, Non-communicable diseases
Introduction
The accessibility of antiretroviral therapy (ART) has fundamentally changed human immunodeficiency virus (HIV) infection from a life-threatening disease to a chronic condition that necessitates lifelong treatment with ART. Active participation in HIV care, particularly consistent adherence to ART, is associated with sustained viral suppression, which enables people with HIV (PWH) to live longer and also effectively prevents the transmission of HIV to uninfected partners [1]. As survival rates have improved, non-communicable diseases (NCD) such as cardiometabolic disorders have emerged as a significant cause of morbidity and mortality among the ageing population of PWH [2,3]. These comorbidities occur at an earlier age compared with the HIV-negative general population and can be attributed in part to the adverse effects of certain ART and the underlying chronic persistent inflammation associated with HIV infection [4–6].
Couples in serodiscordant or seroconcordant relationships are a vital population for HIV prevention and care efforts. Serodiscordant couples (in which one partner is HIV-infected and the other HIV-negative) have historically contributed substantially to new HIV infections [7]. However, mounting evidence that HIV-infected individuals with an undetectable viral load (VL) cannot transmit the virus has increased acceptance of serodiscordant relationships, and their numbers are expected to rise [1,8,9]. This represents a paradigm shift from the traditional approach of identifying such couples through routine couples counselling and testing toward more voluntary disclosure and proactive engagement in care. Importantly, studies have shown that prevention of transmission to one’s partner is a primary motivation for ART uptake among PWH in serodiscordant relationships. Moreover, PWH in serodiscordant partnerships demonstrate significantly improved ART uptake and adherence compared with those in seroconcordant partnerships (where both partners are HIV-infected) [10,11]. This underscores the critical role that relationship dynamics and protective motivation play in treatment engagement and, ultimately, in achieving viral suppression and preventing new infections.
Despite the public health importance of both viral suppression and NCD burden, there are important knowledge gaps regarding HIV-infected individuals in cohabiting relationships. Most published work reports individual-level ART adherence/ viral suppression or NCD prevalence without consideration of relationship context; comparatively, studies characterizing these outcomes among HIV-infected individuals in seroconcordant versus serodiscordant partnerships are lacking. Understanding how relationship type (seroconcordant versus serodiscordant) may influence individual health outcomes is important given the unique motivations and dynamics within each partnership type. In this study, we investigated the VL suppression rates and the prevalence of hypertension and diabetes among HIV infected individuals in seroconcordant and serodiscordant cohabiting relationships. Given the public health importance of preventing onward transmission and the rising burden of chronic disease in the ageing population of PWH, evidence examining outcomes by relationship type is timely and may be policy relevant.
Methods
Study design and setting
This hospital-based, cross-sectional study was conducted at the ART outpatient clinic of the Federal Teaching Hospital (FTH) Gombe, located in Gombe State, Northeast Nigeria. Ethical approval was obtained from the institutional Ethics and Research Committee before commencement of the study (Approval Number: [FTHG/HREC/S.13/382]). Participants were recruited using a consecutive sampling method. Written informed consent was obtained from all participants prior to enrolment. The ART clinic provides routine HIV care and follow-up services. During each clinic visit, weight and blood pressure are routinely measured and recorded. Plasma HIV VL is determined at 6 months and 1 year after ART commencement with annual monitoring thereafter to assess treatment response. Targeted VL testing is performed for patients with suspected clinical or immunological failure, while individuals with unsuppressed VL (>200 copies/mL) are offered enhanced adherence counselling (EAC). Body mass index (BMI) categories were defined using the WHO classification as follows: underweight (<18.5 kg/m²), normal (18.5–24.9 kg/m²), overweight (25–29.9 kg/m²), and obese (≥30 kg/m²). Hypertension was defined as the current use of antihypertensive medication or a systolic blood pressure ≥140 mmHg and/or a diastolic blood pressure ≥90 mmHg. Known diabetic patients on treatment, as well as those screened within the preceding three months, were included. The first-line ART regimen consisted of tenofovir, lamivudine, and dolutegravir, while the second-line regimen comprised a protease inhibitor-based regimen (atazanavir or darunavir boosted with ritonavir).
Study population and recruitment
The study recruited heterosexual, HIV-infected adults aged 18 years and above attending routine follow-up visits at the ART clinic. Potentially eligible seroconcordant participants were first identified during clinic attendance. The study objectives and procedures were explained to interested individuals, and those who provided informed consent were interviewed. They were then asked to contact their partners to request permission for telephone contact. HIV-infected partners were subsequently contacted by phone, and consenting individuals were enrolled. Pregnant or lactating women, individuals with acute illness, or those with known organ dysfunction were excluded from participation.
Data collection
Data were obtained from hospital records and entered into a structured questionnaire. Upon receiving consent, the ART clinic identification numbers of participants and their partners were used to retrieve relevant clinical data from hospital records. A de-identified structured questionnaire was used to collect the following variables:
- Demographic data: Age, marital status, and duration of cohabitation
- HIV-related information: ART initiation date, current ART regimen, and VL measurements over the past 48 months
- Adherence history: Documentation of EAC over the past 48 months
- Clinical parameters: Weight, height, and presence of NCD: hypertension and diabetes
The clinic’s routine procedure for measuring weight, blood pressure, and conducting laboratory investigations ensured that updated clinical parameters were systematically recorded during follow-up visits. These records were reviewed and extracted for analysis.
Statistical analysis
All statistical analyses were performed using R software (version 4.5.2, R Foundation for Statistical Computing, Vienna, Austria). Descriptive statistics were calculated for all variables, with continuous variables presented as means ± standard deviation (SD) and categorical variables as frequencies and percentages. The Shapiro-Wilk test was used to assess the normality of continuous variables. For bivariate comparisons between seroconcordant and serodiscordant groups, independent samples t-tests were used for normally distributed continuous variables, while the Mann-Whitney U test was applied for non-normally distributed variables. Chi-square tests were used to compare categorical variables between groups; Fisher's exact test was employed when expected cell counts were less than five.
Missing data were handled using multiple imputation by chained equations (MICE) with predictive mean matching (PMM). Five imputed datasets were generated with 50 iterations per imputation. Variables with missing data included height, BMI, and other clinical measurements affecting less than 10% of observations. Complete case analysis was performed for sensitivity assessment. Multivariable logistic regression analyses were conducted to identify independent predictors of VL suppression and hypertension. For viral suppression, the model included concordance status (primary exposure), age, sex, ART duration, regimen type (first-line vs second line), and history of EAC as covariates. For hypertension, the model included concordance status, age, sex, BMI, and ART duration. Results were reported as adjusted odds ratios (aOR) with 95% confidence intervals (CI). Model fit was assessed using the Hosmer-Lemeshow goodness-of-fit test. Exploratory subgroup analyses examined viral suppression rates stratified by sex, and Pearson correlation analysis assessed the relationship between ART duration and viral suppression. All statistical tests were two-tailed, and p-values <0.05 were considered statistically significant.
Results
Demographic and clinical characteristics of the participants
A total of 247 participants living with HIV with a mean age of 47.59 ± 10.61 years were included in the analysis. The sample was evenly distributed by sex, with 122 (49.4%) males and 125 (50.6%) females. Participants were on ART for a mean duration of 13.29 ± 5.43 years, with the majority (91.1%, n=225) on first-line regimens and 8.9% (n=22) on second-line regimens. The mean weight was 66.07 ± 13.27 kg and the mean BMI was 24.56 ± 5.08 kg/m². Regarding concordance status, 176 (71.3%) participants were from seroconcordant couples where both partners were HIV-infected, while 71 (28.7%) were HIV-infected individuals from serodiscordant couples. Viral suppression was achieved in the vast majority of participants (97.6%, n=242), with only 5 (2.0%) having unsuppressed VL. The prevalence of hypertension was 9.3% (n=23), while diabetes was rare, affecting 2.83% (7/247) of the sample. EAC for previous virologic failure, had been provided to 6.5% (n=16) of participants. Details of the demographic characteristics are shown in Table 1.
|
Variable |
Mean ± SD |
|
Age (years) |
47.59 ± 10.61 (range: 20, 95) |
|
Sex, number (%) Male Female |
122 (49.39) 125 (50.61) |
|
Duration on ART (years) |
13.29 ± 5.43 (range: 1, 24) |
|
Weight (kg) |
66.07 ± 13.27 (range: 38, 125) |
|
BMI (kg/m2) |
24.56 ± 5.08 (range: 15.97, 45.91) |
|
Serostatus Seroconcordant Serodiscordant |
176 (71.26) 71 (28.74) |
|
Viral load (copies/mL), number (%) Suppressed Unsuppressed |
242 (97.57) 5 (2.02) |
|
EAC, number (%) No Yes |
231 16 |
|
ART regimen, number (%) First line Second line |
225 (91.09) 22 (8.91) |
|
Hypertension, number (%) No Yes |
224 (90.69) 23 (9.31) |
|
Diabetes, number (%) No Yes |
240 (97.17) 7 (2.83) |
|
Key: ART: Antiretroviral Therapy; BMI: Body Mass Index; EAC: Enhanced Adherence Counselling; SD: Standard Deviation |
|
Comparison by serostatus
Baseline characteristics stratified by concordance status are presented in Table 2. The two groups were well-balanced across most demographic and clinical characteristics. There were no significant differences in age (p=0.432), sex distribution (p=1.000), weight (p=0.184), or BMI (p=0.380) between seroconcordant and serodiscordant participants. However, two significant differences emerged. Seroconcordant couples had a significantly longer duration on ART compared with serodiscordant couples (p<0.001), while serodiscordant couples had been married significantly longer than seroconcordant couples (p=0.033). Despite these temporal differences, the two groups had comparable clinical outcomes. VL suppression rates were excellent and similar in both groups (97.7% seroconcordant vs 98.6% serodiscordant, p=1.000), as was hypertension prevalence (9.1% vs 9.9%, p=1.000). The distribution of ART regimens and the proportion of participants with a history of EAC were also comparable between groups.
|
Variables |
Seroconcordant |
Serodiscordant |
p-value |
|
Age (years), mean (SD) |
47.29 (10.7) |
48.46 (10.4) |
0.432 |
|
Sex, number (%) Male Female |
88 (50.0) 88 (50.0) |
35 (49.3) 36 (50.7) |
1.0 |
|
ART duration, (years), mean (SD) |
14.02 (4.98) |
11.24 (6.14) |
<0.001 |
|
Marriage duration, (years), mean (SD) |
17.99 (8.45) |
20.83 (11.4) |
0.033 |
|
Weight (kg), mean (SD) |
65.21 (12.38) |
67.69 (15.21) |
0.184 |
|
BMI (kg/m2), mean (SD) |
24.4 (4.84) |
25.03 (5.71) |
0.38 |
|
ART regimen, number (%) First line Second line |
160 (90.9) 16 (9.1) |
67 (94.4) 4 (5.6) |
1.0 |
|
Viral load, number (%) Suppressed Unsuppressed |
172 (97.7) 4 (2.3) |
70 (98.6) 1 (1.4) |
1.0 |
|
Hypertension, number (%) No Yes |
160 (90.9) 16 (9.1) |
64 (90.1) 7 (9.9) |
1.0 |
|
EAC, number (%) No Yes |
165 (93.8) 11 (6.2) |
66 (93.0) 5 (7.0) |
1.0 |
|
Key: ART: Antiretroviral Therapy; BMI: Body Mass Index; EAC: Enhanced Adherence Counselling; SD: Standard Deviation. |
|||
Regression analysis
In the multivariable analysis, concordance status was not significantly associated with viral suppression after adjusting for age, sex, ART duration, regimen type, and history of EAC. However, two factors were independently associated with viral suppression. Participants on second-line ART regimens had significantly lower odds of viral suppression compared to those on first-line regimens (aOR=0.07, 95% CI: 0.01–0.76, p=0.028). Additionally, participants with a history of EAC had significantly lower odds of current viral suppression compared to those without such a history (aOR=0.11, 95% CI: 0.01–0.94, p=0.044). Age, sex, and ART duration were not significantly associated with viral suppression in the adjusted model. Furthermore, after adjusting for concordance status, age, sex, BMI, and ART duration, concordance status was not significantly associated with hypertension. Two factors emerged as independent predictors of hypertension. Male sex was significantly associated with increased odds of hypertension compared to female sex (aOR=3.13, 95% CI: 1.15–9.09, p=0.025). Similarly, higher BMI was independently associated with increased odds of hypertension, with each one-unit increase in BMI associated with 12% higher odds (aOR=1.12, 95% CI: 1.02–1.23, p=0.014). Age showed a trend toward significance (aOR=1.04, 95% CI: 1.00–1.08, p=0.080), suggesting that older age may be associated with increased hypertension risk, though this did not reach statistical significance. Figure 1 displays hypertension prevalence stratified by age, BMI, and sex, revealing striking patterns. Among males, hypertension prevalence ranged from 0% to 36.4%, with the highest burden observed in overweight males aged 50–59 years (36.4%, n=11). Notably, even young males (<40 years) with overweight BMI demonstrated substantial hypertension prevalence (28.6%, n=7), suggesting early cardiovascular impact of elevated body weight. Males showed hypertension across all BMI categories, including underweight (20.0% in the 50–59 year age group, n=5) and normal BMI (7.1-14.3% depending on age), indicating vulnerability independent of obesity. ART duration was not associated with hypertension risk.
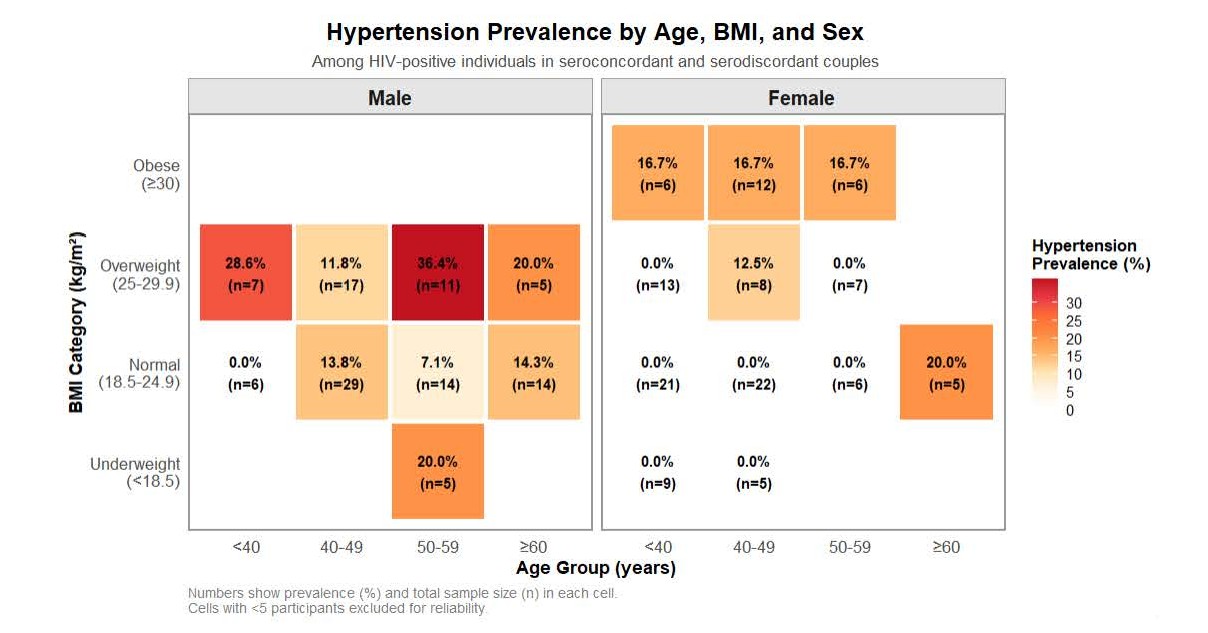
Figure 1. Hypertension prevalence stratified by age, BMI, and sex. Heat map showing prevalence (%) and sample size (n) across age groups and BMI categories. Color intensity: white (0%) to red (>30%). Age: <40, 40–49, 50–59, ≥60 years. BMI (kg/m²): <18.5 (underweight), 18.5–24.9 (normal), 25–29.9 (overweight), ≥30 (obese).
Discussion
This study examined ART adherence, VL suppression rates, hypertension, and diabetes prevalence among HIV-infected individuals in seroconcordant and serodiscordant cohabiting relationships. The principal finding of this study is that treatment history particularly use of second-line ART regimens and prior virologic failure significantly predicted suboptimal viral suppression, while traditional cardiometabolic risk factors drove hypertension prevalence. These findings underscore the complex interplay between HIV treatment trajectories and NCD burden in ageing cohabiting couples living with HIV.
The absence of differences in viral suppression by concordance status is reassuring, with both groups achieving excellent suppression rates (97.6%) under standard care. However, treatment history emerged as an important marker of virologic vulnerability. Participants on second-line ART had 93% lower odds of viral suppression compared to first-line recipients (aOR=0.07, 95% CI: 0.01–0.76, p=0.028). This aligns with previous studies at our center and with another study from Nigeria showing higher failure rates on second-line therapy [12,13]. This association likely reflects the underlying complexity of these patients’ clinical trajectories that may include prior treatment failure, drug resistance, and adherence challenges rather than a causal effect of the regimen itself. Additionally, the protease inhibitor-based second-line regimens used in our cohort demonstrated inferior suppression compared to dolutegravir-based first-line therapy, which may further contribute to the observed disparity [14]. Similarly, participants with history of EAC had significantly lower odds of current suppression (aOR=0.11, 95% CI: 0.01–0.94, p=0.044). Critically, this association should be interpreted as a marker rather than a cause: EAC history identifies patients who have experienced prior virologic failure and continue to face ongoing treatment challenges. Programmatic studies confirm that while many achieve re-suppression after EAC, a substantial minority remain unsuppressed on subsequent testing [15,16]. This pattern does not reflect EAC ineffectiveness, rather, EAC serves its intended purpose of identifying and supporting patients with virologic failure. Instead, it reveals that a single episode of intensive counselling, while beneficial, is insufficient for patients contending with complex, persistent barriers including food insecurity, mental health issues, or drug resistance. These findings suggest that both second-line ART use and EAC history serve as clinical markers identifying patients who require sustained, comprehensive support through differentiated service delivery models incorporating frequent monitoring, continuous psychosocial counselling, peer support, and community-based interventions rather than episodic approaches alone.
Analysis of factors associated with hypertension among the study participants revealed that male sex emerged as the strongest independent predictor, with males having more than three times higher odds compared to females (aOR=3.13, p=0.025). This sex disparity aligns with broader epidemiological patterns and may reflect hormonal differences, poorer health-seeking behavior among men, and biological differences in cardiovascular physiology [17,18]. BMI was also independently associated with hypertension risk, with each one-unit increase conferring a 12% higher odds (aOR=1.12, p=0.014). This represents a modifiable risk factor amenable to lifestyle interventions. Given the mean BMI of 24.56 kg/m² approaching the overweight threshold, there is a clear opportunity for primary prevention through integrated nutritional counselling and physical activity promotion. The overall hypertension prevalence of 9.3% observed in this cohort is comparable to previous reports of 9% in Ghana and 10.2% in Zimbabwe but considerably lower than the 50.1% reported among South African PWH aged >50 years [19–21]. Variations in hypertension prevalence across studies likely reflect differences in sociodemographic characteristics and the age distribution of the study populations. Nevertheless, as the HIV-infected population continues to age and life expectancy improves, the burden of hypertension and other cardiovascular diseases is expected to rise. These findings underscore the importance of gender-specific screening strategies and proactive integration of cardiovascular risk assessment and management into routine HIV care.
Interestingly, seroconcordant couples had significantly longer durations on ART compared to serodiscordant couples (14.02 vs 11.24 years, p<0.001), while serodiscordant couples had been cohabiting longer (20.83 vs 17.99 years, p=0.033). These patterns may reflect different HIV acquisition and disclosure dynamics in the two couple types. Seroconcordant couples may have been diagnosed and initiated on treatment simultaneously or within close timeframes, potentially reflecting shared risk exposures or mutual testing following one partner's diagnosis. The longer marriage duration in serodiscordant couples could suggest HIV acquisition later in the relationship, possibly through extra-relationship exposures. Despite these temporal differences in HIV and relationship histories, the similar clinical outcomes between groups reinforce that service delivery can be standardized regardless of couple concordance status.
This study has several strengths, including the couple-based recruitment strategy, comprehensive assessment of both HIV-specific and cardiovascular outcomes, and the use of multivariable analysis to adjust for confounders. The cross-sectional design precludes causal inference and assessment of temporal relationships. Importantly, the excellent viral suppression rate, while clinically favorable, resulted in only five unsuppressed cases, substantially limiting statistical power for multivariable analyses of viral suppression. This is evident in the wide confidence intervals observed, particularly for concordance status (95% CI: 0.13–48.0), necessitating cautious interpretation of these estimates. A significant limitation is the absence of comprehensive cardiovascular risk assessment beyond hypertension and BMI. We did not evaluate other important cardiovascular risk factors including lipid profiles, smoking status, physical activity levels, or family history of cardiovascular disease, while diabetes showed minimal variation in our sample. This restricted assessment limits our ability to fully characterize cardiometabolic risk in this population and may underestimate the true burden of cardiovascular disease risk. The relatively low hypertension prevalence may reflect both the demographic characteristics of our sample and potential underdiagnosis in this clinic-based population.
In conclusion, this study demonstrates that HIV serostatus does not influence viral suppression or hypertension rates among HIV-infected individuals in cohabiting couples, whether seroconcordant or serodiscordant. However, important individual-level vulnerabilities emerged: patients on second-line regimens and those with prior virologic failure markers need sustained adherence support, while male sex and elevated BMI identify individuals requiring targeted hypertension screening and weight management interventions. These findings highlight the critical need for integrating comprehensive cardiovascular screening into routine HIV care. As the HIV-infected population ages and NCD increasingly contribute to morbidity, proactive integrated care addressing modifiable risk factors, particularly weight management and sustained treatment adherence support, will be essential for optimizing long-term health outcomes.
Conflict of Interest
The authors declare none.
Funding
There was no funding for this study
Acknowledgement
The authors acknowledge the contributions of staffs of ART clinic FTH Gombe in data acquisition during the study.
Author’s Contributions
MWA, FKS, and MMS designed the study. MWA and MMS conducted data acquisition. MWA performed the data analysis. MWA, IAB, ZIN, UMH, and MMM contributed to data interpretation and critical revision of the manuscript. All authors read and approved the final manuscript.
References
2. Shah AS, Stelzle D, Lee KK, Beck EJ, Alam S, Clifford S, et al. Global burden of atherosclerotic cardiovascular disease in people living with HIV: systematic review and meta-analysis. Circ. J. 2018 Sep 11;138(11):1100–12.
3. Zhabokritsky A, Klein M, Loutfy M, Guaraldi G, Andany N, Guillemi S, et al. Non-AIDS-defining comorbidities impact health related quality of life among older adults living with HIV. Front. Med. 2024 Apr 16;11:1380731.
4. Neuhaus J, Jacobs Jr DR, Baker JV, Calmy A, Duprez D, La Rosa A, et al. Markers of inflammation, coagulation, and renal function are elevated in adults with HIV infection. The Journal of infectious diseases. 2010 Jun 15;201(12):1788–95.
5. Amutuhaire W, Mulindwa F, Castelnuovo B, Brusselaers N, Schwarz JM, Edrisa M, et al. Prevalence of cardiometabolic disease risk factors in people with HIV initiating antiretroviral therapy at a High-Volume HIV Clinic in Kampala, Uganda. Open Forum Infect. Dis 2023 Jun;10(6):ofad241.
6. Ye R, Zhang Y, Gu J. The prevalence of comorbidities and differences in noncommunicable diseases and nonrandom associations of comorbidities between HIV-infected and-uninfected individuals in Guangdong Province, China. BMC Public Health. 2025 Feb 24;25(1):761.
7. Colombe S, Beard J, Mtenga B, Lutonja P, Mngara J, de Dood CJ, et al. HIV-seroconversion among HIV-1 serodiscordant married couples in Tanzania: a cohort study. BMC infectious diseases. 2019 Jun 13;19(1):518.
8. Smith DK, Van Handel M, Wolitski RJ, Stryker JE, Hall HI, Prejean J, et al. Vital Signs: Estimated Percentages and Numbers of Adults with Indications for Preexposure Prophylaxis to Prevent HIV Acquisition — United States, 2015. MMWR Morb Mortal Wkly Rep. 2015 Nov 27;64(46):1291–5.
9. Rendina HJ, Cienfuegos-Szalay J, Talan A, Jones SS, Jimenez RH. Growing acceptability of Undetectable= Untransmittable but widespread misunderstanding of transmission risk: findings from a very large sample of sexual minority men in the United States. J Acquir Immune Defic Syndr. 2020 Mar 1;83(3):215–22.
10. Patel RC, Leddy AM, Odoyo J, Anand K, Stanford-Moore G, Wakhungu I, et al. What motivates serodiscordant couples to prevent HIV transmission within their relationships: findings from a PrEP implementation study in Kenya. Cult Health Sex. 2018 Jun 3;20(6):625–39.
11. Kim HY, Hanrahan CF, Dowdy DW, Martinson N, Golub J, Bridges JF. The effect of partner HIV status on motivation to take antiretroviral and isoniazid preventive therapies: a conjoint analysis. AIDS care. 2018 Oct 3;30(10):1298–305.
12. Ali MW, Musa MS. The effect of mobile phone utilization for enhanced adherence counselling intervention among persons with HIV. AIDS care. 2023 Dec 2;35(12):1919–27.
13. Obasa GB, Ijaiya M, Okwor E, Dare B, Emerenini F, Oladigbolu R, et al. Factors associated with viral load re-suppression after enhanced adherence counseling among people living with HIV with an initial high viral load result in selected Nigerian states. PLOS Glob. Public Health. 2024 Nov 22;4(11):e0002876.
14. Aboud M, Kaplan R, Lombaard J, Zhang F, Hidalgo JA, Mamedova E, et al. Dolutegravir versus ritonavir-boosted lopinavir both with dual nucleoside reverse transcriptase inhibitor therapy in adults with HIV-1 infection in whom first-line therapy has failed (DAWNING): an open-label, non-inferiority, phase 3b trial. The Lancet infectious diseases. 2019 Mar 1;19(3):253–64.
15. Ndikabona G, Alege JB, Kirirabwa NS, Kimuli D. Unsuppressed viral load after intensive adherence counselling in rural eastern Uganda; a case of Kamuli district, Uganda. BMC Public Health. 2021 Dec 18;21(1):2294.
16. Bakari HM, Alo O, Mbwana MS, Salim SM, Ally ZM, Musoke R, et al. Enhanced adherence counselling completion rates, viral load suppression in people with HIV in Africa: systematic review and meta-analysis. Discover Public Health. 2025 Jan 13;22(1):12.
17. Masenga SK, Povia JP, Mutengo KH, Hamooya BM, Nzala S, Heimburger DC, et al. Sex differences in hypertension among people living with HIV after initiation of antiretroviral therapy. Front. Cardiovasc. Med. 2022 Nov 17;9:1006789.
18. Tegegne KD, Adela GA, Kassie GA, Mengstie MA, Seid MA, Zemene MA, et al. Prevalence and factors associated with hypertension among peoples living with HIV in East Africa, a systematic review and meta-analysis. BMC Infectious Diseases. 2023 Oct 25;23(1):724.
19. Appiah LT, Sarfo FS, Huffman MD, Nguah SB, Stiles JK. Cardiovascular risk factors among Ghanaian patients with HIV: a cross‐sectional study. Clin. Cardiol. 2019 Dec;42(12):1195–201.
20. Magodoro IM, Esterhuizen TM, Chivese T. A cross-sectional, facility based study of comorbid non-communicable diseases among adults living with HIV infection in Zimbabwe. BMC Res. Notes. 2016 Aug 2;9(1):379.
21. Okyere J, Ayebeng C, Owusu BA, Dickson KS. Prevalence and factors associated with hypertension among older people living with HIV in South Africa. BMC Public Health. 2022 Sep 5;22(1):1684.