Abstract
Background: Exercise Training is beneficial in heart failure patients, while training opportunities are limited. Pedelecs represent a novel training possibility for these patients, while safety and efficacy of pedelec training in heart failure is unknown. Therefore, we conducted a pilot study to address these issues. The study “HI-Herz.BIKE Saar” (August 2017 - September 2019) examined the health benefits and training effects of e-bikes (pedelecs) in patients from ambulatory heart groups with moderate chronic heart failure (CHI).
Methods: Ten subjects with a strictly defined NYHA stage II-III heart failure and a LVEF of =50% were selected. The presented clinical study is explicitly marked as a pilot study, as a new, so far not tested technique was used for exercise control. When selecting the heart failure patients defined in this way, a higher number of subjects could not be reached at only one study center. Participants cycled once weekly for 60-150 min and 20-50 km with a follow-up of 2 years as detailed in the Methods section. The new HeartGo® system used here for the first time allows heart rate- controlled training on a special pedelec via a smartphone app. The groups were accompanied during the training rides by a doctor and a paramedic. The training units were increased in duration, distance, and target frequency every six months. Frequency behavior, pedaling and motor load on the pedelec as well as clinical data such as ejection fraction, a biomarker (NT-pro BNP), risk factors, arterial blood pressure, and ergometric tests were measured.
Results: Pedelec training in heart failure subjects resulted in significant increases of the index of well-being (p<0.05) and of leftventricular ejection fraction by 29% (p<0.05). This was paralleled by a significant decrease in the heart failure parameter NT-pro BNP by 27% (p<0.05), and a significant increase in performance (ergometric power +44%, p<0.05). Moreover, systolic blood pressure decreased significantly by 11% (p<0.05). In contrast, Body Mass Index and cholesterol levels showed no significant changes. No cardiac complications occurred.
Conclusions: These results suggest that pedaling is not only safe for stable heart NYHA II-III failure patients with an EF =50%, but can induce significant improvements in cardiac performance indices. The subjects were enthusiastic and satisfied with this form of training. The results of this pilot study with its methodological weaknesses should be verified in a larger follow-up study.
Keywords
Heart rate-controlled training, HeartGo® system, Chronic heart failure, Pedelec
Introduction
Secondary prevention of cardiovascular disease such as heart failure includes regular physical activity with endurance and strength training, which is used for this purpose with high prevalence [1,2]. Early rehabilitation should begin in hospital (phase I), be continued in a rehabilitation clinic or as an outpatient close to home (phase II), and then (phase III) preferably in outpatient heart groups (AHG).
A moderate training of 5x30 min or 150 min/week as an effective training goal is aimed at, but often not achieved in heart groups. Endurance sports like walking, running or swimming are recommended. Cycling in heart groups is done less frequently because the performance in the groups is different. Numerous studies have shown that cycling improves endurance, coordination, flexibility, and strength; at the same time, the body weight is not carried, so that this sport is also used very well in the case of overweight and is advantageous for heart patients [2,3]. There is no structured offer for cycling as a rehabilitation sport, especially for patients with heart failure. Here, the recommendations were reserved, since patients with heart failure are usually older participants and because of possible cardiac incidents or accidents, it is assumed that cycling training is dangerous.
Here, electrically assisted cycling is a good option, especially since the pedelec is becoming increasingly popular with seniors. Initial studies show that in overweight people, an improvement in spiroergometric readings is possible using e-bikes [3].
The disadvantage is that older riders usually choose a high pedaling power support because it is “easier” to ride. This reduces the actually desired training effect; there is “gentle riding”.
With a heart rate-controlled system, this relieving behavior is avoided. This results in individual stress and comparable loads. This makes controlled endurance training on the pedelec, similar to stationary ergometry, possible as an option in addition to regular training. Studies on this method are not available.
Also, a scientific evaluation is then easier to realize, especially since the benefits and risks of regular training of the rehabilitation phase III in outpatient heart groups have not been sufficiently scientifically investigated. Haberecht et al. [4] report on insufficient lifestyle changes and about too little physical activity in heart groups, which is, however, considered sufficient by others [5]. It should be noted that participation in a heart group once a week and often less than 45 minutes is insufficient for an efficient training program.
Reports on the use and value of such pedelec assistance systems have not yet been published, apart from some publications on the general use of pedelecs by athletes and seniors with diabetes mellitus [6].
We hypothesized that pedelec training is safe for patients with stable, mild to moderate heart failure, and that it may result in beneficial cardiovascular effects. To test our hypothesis, ten subjects with a strictly defined NYHA stage II-III and a LVEF of ≤ 50% were selected. The presented clinical study is explicitly marked as a pilot study, as a new, so far not tested technique was used for exercise control. When selecting the heart failure patients defined in this way, a higher number of subjects could not be reached at only one study center.
Materials and Methods
In this clinical pilot study, the novel system HeartGo®, which was tested for practicability by preliminary investigations, was used. This frequency-based system automatically controls the training process. Training and clinical parameters were measured. Training was carried out in summer on level paths along the Saar river (“outdoor” training), in winter inside a sports hall (“indoor” training). From August 22nd, 2017 until September 10th, 2019, we carried out 93 training sessions (31 “indoor”, 62 “outdoor”). The participation frequency of the ten study subjects was always >90%. The mean age was 61.5 years (range 43-82), 2 participants were female and 8 were male, the average BMI was 27 (range 21-37). The default training or target frequency averaged 96 beats/min (range 83-116).
Objectives and significance of the study
Research question: Is a heart rate-based training system using pedelecs in heart group participants with heart failure suitable to demonstrate effects on safety of the training process, acceptance of the system, clinical and prognostic parameters?
In a prospective clinical pilot study with 10 patients from Saarland heart groups diagnosed with heart failure NYHA II to III, the novel system HeartGo®, which was tested for practicability by preliminary examinations [7], was used. Not only parameters of the training process were measured, but also clinical parameters, which were intended to provide information about the course of health and thus about the prognosis of the disease.
Study design
10 volunteers with chronic heart failure were recruited with the following requirements:
1. Study duration 2 years,
2. 6 months of belonging to a heart group,
3. Stable clinical condition,
4. Stable medication (see Table 4),
5. NYHA II - III,
6. LVEF ≤50% (HfrEF),
7. 0.5 watts/kg power,
8. Training 1/week 60 - 150 min,
9. Training heart rate 60-70% of maximum heart rate,
10. Summer and winter mode,
11. Distances 2x10 to 2x25 (20 - 50) km.
The test persons were provided with the bikes in fully functional condition.
The presented study is a pilot study, as the strictly defined selection locally hardly allowed for higher numbers of test persons and was carried out with new, previously untested technology. The study was to be followed by further, preferably multi-center studies for verification purposes.
Training parameters
Training parameters were training duration, training distance, frequency behavior, BORG queries, relation pedaling power to motor power, training blood pressure (by means of commercially available, calibrated wrist device, OMRON).
The Borg scale [8] was used as an orientation scale between 6 and 20 for the sensation of effort.
The training phases during the period of use were divided into two winter phases (indoor training) and two summer phases (outdoor training).
During the four phases (winter 2017/2018, summer 2018, winter 2018/2019, summer 2019) the power and target heart frequencies were adjusted. It started with 60% of the maximum heart rate (HFmax), from half time of the study on 70%, or the calculated training frequency according to Tanaka et al. [9] was set. At a roughly constant speed of 20 km/h, the distances were increased and thus the training duration increased.
The four phases were structured as follows:
The chest belt sensors continuously recorded heart rate (HF) and ECG signal “real time” (standard). For this purpose, the test person was given a target heart rate, which usually corresponded to a previously determined training heart rate [9].
The app offers the possibility of selecting four driving modes:
1. Free ride (free selection of assistance via control element)
2. Tour (support automatically determined by the system by terrain rise or fall: GPS altitude)
3. Outdoor training (summer mode)
4. Stationary ergometer training (winter mode)
Modes 3 and 4 were used for the study. The winter training took place in a hall with jacked-up wheels.
The modes have the control algorithms of the RF-assist coupling. The reference parameter for the control was the pre-set target frequency, which has to be maintained by a combination of pedaling and motor power.
The setting of the target frequency was based on the respective maximum heart rate (HFmax) of the test person, which is either determined ergometrically or calculated according to the formula method of Tanaka [9]. It was usually between 60 (at the beginning) and 70% of the HFmax (middle and end).
However, the target frequency had to be adjusted due to individual tolerance (e.g. beta-blocker medication) in order to avoid overloading the pedal power. This resulted in an adjustment of about 10% below the calculated target frequency (IF).
The control process causes the heart rate to fluctuate around the target rate depending on the load and the pedal assistance to increase as the HR increases. Correspondingly, the pedal power increases out of phase when the HF drops below the IF. This is the typical example of an intact control system.
Clinical parameters
At the beginning (start), halfway through the study (middle), and at the end of the study (end), three separate clinical examinations were performed, which included the following parameters:
1. ECG, blood pressure, bicycle ergometry,
2. Echocardiography,
3. Holter ECG for 24 h,
4. Laboratory data: Blood count, electrolytes, kidney values, CRP, HbA1c, NT-Pro-BNP, cholesterol, LDL- and HDL-cholesterol, triglycerides.
| Phase | Speed [km/h] | Distance [km] | Duration [min] |
|---|---|---|---|
| I | 20 | 20 (2x10) | 60 |
| II | 20 | 30 (2x15) | 90 |
| III | 20 | 40 (2x20) | 120 |
| IV | ≥ 20 | 50 (2x25) | ~150 |
The pedelec was adapted by HeartGo® with deep entry, 250 Watt rear wheel drive, and a battery (450 Wh). The motor allows the activation of up to 10 levels of assistance and two levels of recuperation (power recovery).
Electronic equipment
Pedal power and assistance monitor (Swiss Go Drive®) were connected to an Android app developed by HeartGo® on a standard smartphone. The units are linked to the subject’s bicycle and heart rate via Bluetooth technology. The test person wears a chest strap sensor.
Data management
The following data were processed:
1. Real-time ECG via sensor,
2. Pedaling power (watts), engine power (watts), speed (km/h),
3. Terrain profile, support levels (10).
The data was available to the test person on the smartphone display during the test. After completion of the training, they were transferred to the secure portal of the manufacturer and were then available for evaluation and information to the trainer and to the individual test persons.
Acceptance questionnaire
We used a questionnaire system (Well-being or Wellness index) which was introduced and tested by Kolip [10]. It is divided into three positive (answers are correct) and three negative indicators (answers are not correct) and was asked at the end of the study about the state of health before and after the end of the study (Suppl. Table 1)
Ethics committee
The study was accepted by the Ethics Committee of the Medical Association of the Saarland on April 18, 2018: “With reference to §2 of the statute of the Ethics Commission at the Medical Association of the Saarland, there are no objections to the implementation of the intended research project”.
Statistical analysis
To statistically validate the results, we used the Student’s t-test for paired samples and applied a probability of error of 5%. Statistical significance was accepted at a p-value of <0.05. The value groups were compared at the beginning, in some cases halfway through the term, i.e. after one year, and at the end of the term. The study design is therefore prospective and comparative without control group. It is therefore neither randomized nor blinded.
Results
The results (blood tests, echocardiography, and functional changes) are presented in detail in Tables 1-5.
| Clinical and functional examination | ||||
| Study time point | Start | Middle | End | P-Value |
| Bodyweight (kg) | 84.6 | 84 | >0.05 | |
| Body Mass Index (BMI; kg/m2) | 27.27 | 27.49 | >0.05 | |
| Ergometric power (Watt) | 91.67 | 132.5 | <0.05 | |
| Left-ventricular EF (%) |
44.1 | 53 | 56.6 | <0.05 |
| Systolic blood pressure (mmHg) | 128.5 | 120.1 | 115 | <0.05 |
| Index of Well-being | 1.64 | 6.82 | ||
| 6-Minute Walking Distance (m) | 553.8 | 565.6 | 595.6 | >0.05 |
| Laboratory parameters | ||||
| NT-pro BNP (pg/ ml) |
553.38 | 510 | 408.6 | <0.05 |
| Total cholesterol (mg/dl) | 173.4 | 170.1 | 164.6 | >0.05 |
| LDL-Cholesterol (mg/dl) | 100.4 | 97.6 | 92.7 | >0.05 |
| HDL-Cholesterol (mg/dl) | 54.5 | 48.9 | 51.1 | >0.05 |
| Triglycerides (mg/ dl) | 84.6 | 101.5 | 100.7 | >0.05 |
Table 1: Results of the clinical, functional, and laboratory examinations at the beginning (start), halfway through the study (middle), and at the end of the study (end).
| Training results (Cumulated data) | |||||
| Distance (km) | 1734.30 (1750–3359) | ||||
| Duration (h) | 151 (8-23) | ||||
| Speed (km/h) | 19.8 (18.62-21.47) | ||||
| Heart rate (min-1) | 94.4 (83-126) | ||||
| Pedal power (Watt) | 59.5 (49-87) | ||||
| Engine output (Watt) | 68.1 (52.1-89.2) | ||||
| Training data | |||||
| Study phase | Phase I | Phase II | Phase III | Phase IV | P-Value |
| Training pulse (% HFmax) | 60 | 60 | 70 | 70 | |
| Distance (km) | 20 | 30 | 40 | 50 | |
| Duration (min) | 60 | 90 | 120 | 150 | |
| BORG | 11.5 | 10.5 | 11 | 11 | |
| BORG average | 11.25 | 11.25 | 11.25 | 11.25 | |
| BORG HOME average | 11.18 | 11.18 | 11.18 | 11.18 | |
| Pedal power (Watt) | 61.1 | 68.5 | >0.05 | ||
| Engine output (Watt) | 77 | 81 | >0.05 | ||
| Average heart rate (min-1) | 83.6 | 80.2 | >0.05 | ||
| Training blood pressure | |||||
| Study time point | Start | Middle | End | ||
| Systolic BP (mmHg) | 123 | 109 | 110 | <0.05 | |
| Diastolic BP (mmHg) | 73 | 69 | 69 | <0.05 | |
Table 2: Training results: Pedelec data, perceived exertion, heart rate, and blood pressure. Measurements were taken at the beginning (start), halfway through the study (middle), and at the end of the study (end).
| Significances | ||||
| Study time point | Start | Middle | End | p |
| Ergometric power (Watt) | 91.67 | 132.5 | <0.05 | |
| Left-ventricular EF (%) | 44.1 | 53 | 56.6 | <0.05 |
| Systolic blood pressure (mmHg) | 128.5 | 120.1 | 115 | <0.05 |
| Training Blood pressure syst. | 123 | 109 | 110 | <0.05 |
| Training Blood pressure diastol. | 73 | 69 | 69 | <0.05 |
| NT-pro BNP (pg/ml) | 553.38 | 510 | 408.6 | <0.05 |
| Bodyweight (kg) | 84.6 | 84 | >0.05 | |
| Body Mass Index (BMI; kg/m2) | 27.27 | 27.49 | >0.05 | |
| 6-Minute Walking Distance (m) | 553.8 | 565.6 | 595.6 | >0.05 |
| Total cholesterol (mg/dl) | 173.4 | 170.1 | 164.6 | >0.05 |
| LDL-Cholesterol (mg/dl) | 100.4 | 97.6 | 92.7 | >0.05 |
| HDL-Cholesterol (mg/dl) | 54.5 | 48.9 | 51.1 | >0.05 |
| Triglycerides (mg/dl) | 84.6 | 101.5 | 100.7 | >0.05 |
| Pedal power (Watt) | 61.1 | 68.5 | >0.05 | |
| Motor power (Watt) | 77 | 81 | >0.05 | |
| AVG heart rate (min-1) | 83.6 | 80.2 | >0.05 | |
Table 3: Statistical analysis of results before and after training: Significant differences and insignificant trends.
| Drug treatment during study | Number |
|---|---|
| Beta Blockers | 10 |
| Statins | 8 |
| Diuretics | 6 |
| ACE-Inhibitors | 6 |
| AT1-Blockers | 2 |
| Sacubitril/Valsartan | 1 |
| Aldosterone Antagonists | 5 |
| Antiplatelet Therapy | 4 |
| Anticoagulants (NOACs) | 2 |
| Calcium Blockers | 1 |
Table 4:Medical therapy of study participants.
| Diagnoses of underlying diseases in participants | Number |
|---|---|
| Dilated Cardiomyopathy | 5 |
| Ischemic Cardiomyopathy | 5 |
| Arterial Hypertension | 3 |
| Cchronic obstructive lung disease | 2 |
Table 5: Medical diagnoses of study participants.
Clinical results
A questionnaire (Supplementary Table 1) on subjective well-being carried out before the start and after the end of the study showed (Figure 1A) that the index of wellbeing improved significantly during the study. The ratings of perceived exertion (Figure 1B) on the BORG scale were between 9 and 13 with an average rating of 11 (“quite easy”) corresponding to a rather moderate perceived exertion. At the beginning, in the middle, and at the end of the trial a 6-minute walking test was performed. This showed a nonsignificant trend towards improvement (increase of 7.3%).
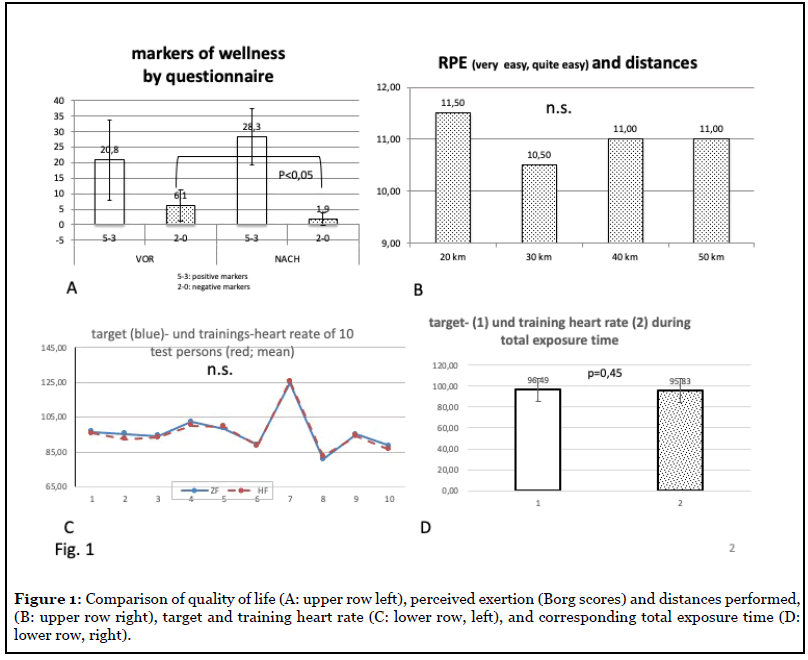
The ratio of target to training heart rate of all study subjects is shown in Figure 1C. There were no significant differences between the set heart rate (target rate) and the achieved frequency level of the test persons. Figure 1D also shows the nondifferent target and heart rates as overall average values.
Pedelec training induced a significant increase in performance, which is evidenced by a significant 45%-increase in ergometric power from 91.67 to 132.5 Watt (p<0.05; Figure 2A). Importantly, the echocardiographically measured left-ventricular ejection fraction LV-EF increased significantly from 44.1 to 56.6% corresponding to an increase of 29% over the twoyear follow-up period (p<0.05; Figure 2B). Moreover, outpatient systolic blood pressure at the beginning and at the end of the study decreased significantly from 128.5 to 115 mm Hg corresponding to a decrease of 11% (p<0.05; Figure 2C).
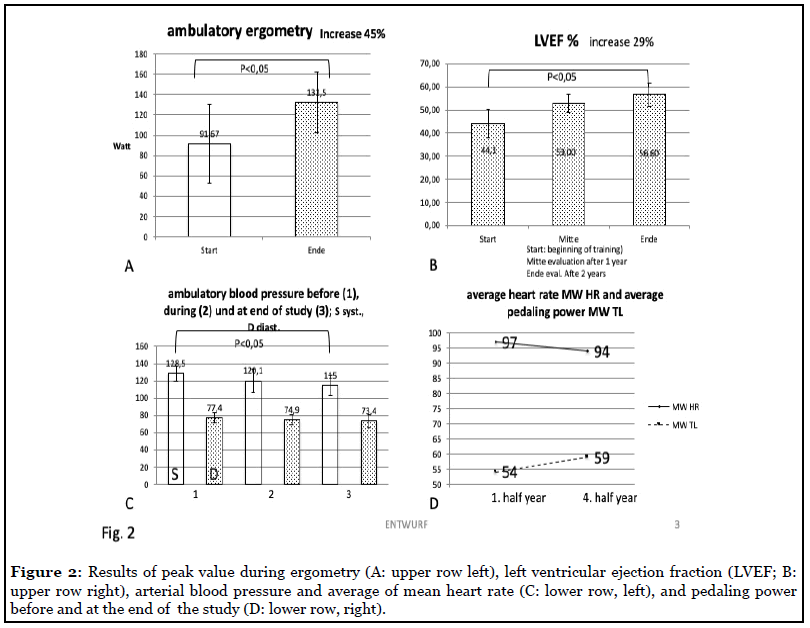
The pedaling power was 64, the motor power was 79 watts, which is 23% higher than the pedaling power. The latter increased in the 4th half year by about 8.5% compared to the first half year. The resting heart rates showed a nonsignificant decrease of about 4.8% compared to the 1st and 4th half year. Figure 2D shows this behavior.
Importantly, pedelec training led to a significant decrease in systolic blood pressure corresponding to 11.6% over the two-year follow-up period (p<0.05; Tables 2 and 3). The resting blood pressure values measured at the beginning of each training session could confirm this as they also decreased by 10%.
Laboratory parameters
At the beginning of the trial all study subjects were characterized by augmented values of the heart failure parameter NT-pro BNP. Importantly, pedelec training resulted in a significant 27.2%-decrease of NT-pro BNP levels over the two-year follow-up period (p<0.05; Tables 1 and 3).
Less noticeable were the values of the lipid status, i.e. total cholesterol, LDL- and HDL-cholesterol, and triglycerides. These only showed trends, but no significant changes. Of note, all test persons were on statin therapy at the time of the study.
Complications and side effects during training
During the study duration of two years there were no incidents due to worsening of heart failure and there were no cardiac complications. All study subjects could safely participate until the end of the trial.
However, two non-cardiac incidents occurred during the study: two patients fell from the bicycle resulting in a fracture of the humerus. No consequential damage occurred and both could resume training following treatment.
Discussion
The results of the present clinical pilot study show that heart rate-controlled training with a pedelec is safe from a cardiac point of view and leads to significant health benefits in stable patients with chronic heart failure in NYHA stages II and III. To our knowledge this is the first report demonstrating this significant effect, which may have important implications for the secondary prevention of heart failure patients.
Cycling in general is one of the most suitable endurance sports for heart patients, since the body weight does not have to be carried. However, it is used too rarely, especially by patients with heart failure. This particular group of elderly people with heart failure, which we have examined in our clinical trial, needs an individually dosed and moderate training load according to medical guidelines. Electrically assisted cycling with a pedelec therefore represents a sensible and attractive alternative for these patients. However, it is still unknown whether and under which conditions a group of patients defined in this way will benefit from pedelec riding. It is also unclear whether this technology is safe enough to recommend the electric bicycle as a training device for cardiac patients in general, and for those with heart failure in particular.
It should be noted that patients with heart failure, who were previously deprived of physical activity, are now recommended endurance sports with a high level of evidence and recommendation (IA), and that these sports provide high benefits. Studies such as the HF-Action study [11], Keteyian et al. 2018 [12], and the CROS study [13] conclude that the health benefit (mortality reduction) is considerable and ranges between 20 and 40%. For some of the parameters measured in this study (e.g. ejection fraction EF) this has also been proven in comparable studies. Erbs et al. [14] report that the EF in a verum group of about 16 patients improved by 10.2% compared to a control group.
Studies on the special question of heart failure patients with the described experimental design are not yet available. There are only preliminary reports [15] that the pedelec may offer advantages compared to the “normal” bicycle and at least does not cause any loss of training.
The use of heart rate as a target and control variable is an adequate and recognized variable in endurance sports, one advantage being that the training effect can be deduced by it [16]. This shows itself in a higher load tolerance, an increasing peak VO2, and a decreasing heart rate at constant load. Adequate frequency control is therefore a desired prerequisite for such a training.
The present system HeartGo® with an Android app on a commercially available smartphone meets this requirement in an optimal way. In the described training mode, the system allows the use of the heart rate as control variable. This works very well, even if the stability, especially that of the sensors, was in need of improvement initially. This can be clearly seen in the Figures 1C and 1 D, which show that optimum frequency control is achieved over the entire training period.
The system was tested in a pilot project (MentorBike 4) [17] on patients in the stationary rehabilitation phase II of a rehabilitation clinic and was judged to be practicable with high acceptance. However, the duration of the test was limited to three months, so it was appropriate to test and evaluate the app over a longer period of time.
The present study was designed as a clinical 2-year pilot study with prospective design. Due to the low number of test persons, the results are only of limited significance. Nevertheless, studies with a low number of subjects lead to meaningful results, for example in the case of questions on physical activity in heart failure [18].
Parameters for objective recording of training data on the pedelec are not available at this time. In general, the training efficiency of heart groups has not been sufficiently investigated, although this physical training has been a central component of holistic rehabilitation sport for more than 40 years with a high level of acceptance. Buchwalski et al. [5] showed a considerable increase in performance by about 50%, but no effect on the “classic” risk factors. However, final statements about the validity of heart groups are missing [19, 20].
The safety of physical training in heart failure patients is classified as high, depending on the severity of the condition. Moreover, it has been shown that the benefit clearly exceeds the risk [21]. This could be confirmed in the study presented. In relation to the total number of 93 training units, the incident rate was 2.15%. In contrast, there is an average benefit of 28.6%, based on all significant changes (ergometry, ejection fraction, blood pressure, biomarkers). However, for high-risk patients such as the group of test persons medical and paramedical supervision is necessary at the very least at the introduction of a pedelec concept. The test persons should be thoroughly trained at the beginning of the training.
If we take as a measure of acceptance the sensation of exertion of the load up to 150 min or 50 km final load the sensation of load according to the BORG scale, this value remains constant at 11 until the end of the study. The ratio of distance (driving distance) to BORG value [22] then increases 2.5 times as an indication of a significant improvement in performance.
The clinical data such as increase in left ventricular ejection fraction LVEF, ergometric power, 6-minute walking test (6MWD], the decrease in the biomarker NTpro BNP or systolic blood pressure indicate a measurable improvement, even if a progression or therapy-related bias due to uncontrolled domestic activity or medically indicated changes in therapy cannot be excluded [19,23].
Further training effects of decreases in cardiovascular risk factors were discernible in the trend. The decrease in heart rate and the increased pedaling load correspond to a moderate training effect [18], which also did not change substantially during the performance increase.
Some of the measured parameters, such as ejection fraction and the NT-pro-BNP values, may point to an improvement in prognosis. However, hard endpoints require a longer observation period, as Taylor et al. [18] demonstrated. Further studies with a larger number of test persons and longer follow-up periods are therefore necessary to clarify the promising role of pedelec training for heart failure patients our results indicate.
Conclusion
The described method of heart rate-controlled cycling on a pedelec in patients with heart disease is effective and acceptance was high.
After careful instruction and practice, this form of training can also be recommended to patients for leisure time activities and training.
Key Message
1. Training of patients with moderate heart failure on the e-bike (pedelec) is possible, safe, and improves the clinical condition of the existing underlying disease.
2. A sustainable training effect for this group could be proven in the presented two-year pilot study.
3. The indicators of well-being and performance tolerance increased significantly, and the blood pressure values decreased accordingly during the study period.
4. The objective performance parameters such as ergometry load and the 6-minute walking test improved.
5. The initially decreased left ventricular ejection fraction increased significantly.
6. The positive results of this pilot study with 10 subjects require verification by a multi-center follow-up study.
Conflicts of Interest
The authors declare that they have no conflict of interest to disclose.
Funding Statement
We received support from the Health Ministry of the Saarland as well as from the Public Health Service.
Acknowledgements
We thank the city of Saarlouis for providing a facility (Stadtgartenhalle) for pedelec training during winter.
Author Contributions Statement
All authors have contributed to the study in the indicated order with Professor Hennersdorf being the senior author. The manuscript was written by Doctors Friedrich, Löllgen, and Hennersdorf. All authors have read the manuscript and approve its submission to Archives of Orthopaedics.
References
2. Steinacker JM, Liu Y, Stilgenbauer F, Nething K. Körperliches Training bei Patienten mit Herzinsuffizienz. Deutsche Zeitschrift für Sportmedizin. 2004;55(5):124- 30.
3. Höchsmann C, Meister S, Gehrig D, Gordon E, Li Y, Nussbaumer M, et.al. Effect of e-bike versus bike commuting on cardiorespiratory fitness in overweight adults: a 4-week randomized pilot study. Clinical Journal of Sport Medicine. 2018 May 1;28(3):255-65.
4. Haberecht O, Bärsch-Michelmann A. Herzgruppen in Deutschland: Stand und Perspektiven. Herzmedizin. 2013;4:33-8.
5. Buchwalsky G, Buchwalsky R, Held K. Langzeitwirkungen der Nachsorge in einer ambulanten Herzgruppe Eine Fall-/Kontrollstudie. Zeitschrift für Kardiologie. 2002 Feb 1;91(2):139-46.
6. Cooper AR, Tibbitts B, England C, Procter D, Searle A, Sebire SJ, et.al. Potential of electric bicycles to improve the health of people with Type 2 diabetes: a feasibility study. Diabetic Medicine. 2018 Sep;35(9):1279-82.
7. Emrich A, Leonhardt F, Werth D, Loos P. Proactive assistance for device-integrated training adjustment in outdoor rehabilitation training. Extended Abstract, Technically Assisted Rehabilitation 2015.
8. Borg GA. Psychophysical bases of perceived exertion. Medicine & Science in Sports & Exercise. 1982; 14(5): 377- 81.
9. Tanaka H, Monahan KD, Seals DR. Age-predicted maximal heart rate revisited. Journal of the American College of Cardiology. 2001 Jan 1;37(1):153-6.
10. Kolip P, Schmidt B. Der Fragebogen zur Erfassung körperlichen Wohlbefindens (FEW 16): Konstruktion und erste Validierung. Zeitschrift für Gesundheitspsychologie. 1999;7(2):77-87.
11. O’Connor CM, Whellan DJ, Lee KL, Keteyian SJ, Cooper LS, Ellis SJ, et.al. Efficacy and safety of exercise training in patients with chronic heart failure: HF-ACTION randomized controlled trial. Journal of the American Medical Association. 2009 Apr 8;301(14):1439-50.
12. Keteyian SJ, Kerrigan DJ, Lewis B, Ehrman JK, Brawner CA. Exercise training workloads in cardiac rehabilitation are associated with clinical outcomes in patients with heart failure. American Heart Journal. 2018 Oct 1; 204:76-82.
13. Rauch B, Davos CH, Doherty P, Saure D, Metzendorf MI, Salzwedel A, et.al. The prognostic effect of cardiac rehabilitation in the era of acute revascularisation and statin therapy: A systematic review and meta-analysis of randomized and non-randomized studies–The Cardiac Rehabilitation Outcome Study (CROS). European Journal of Preventive Cardiology. 2016 Dec;23(18):1914-39.
14. Erbs S, Höllriegel R, Linke A, Beck EB, Adams V, Gielen S, et.al. Exercise training in patients with advanced chronic heart failure (NYHA IIIb) promotes restoration of peripheral vasomotor function, induction of endogenous regeneration, and improvement of left ventricular function. Circulation: Heart Failure. 2010 Jul;3(4):486-94.
15. Peterman JE, Morris KL, Kram R, Byrnes WC. Pedelecs as a physically active transportation mode. European Journal of Applied Physiology. 2016 Aug 1;116(8):1565-73.
16. Vanhees L, De Sutter J, GeladaS N, Doyle F, Prescott E, Cornelissen V et.al. Importance of characteristics and modalities of physical activity and exercise in defining the benefits to cardiovascular health within the general population: recommendations from the EACPR (Part I). European Journal of Preventive Cardiology. 2012 Aug;19(4):670-86.
17. Emrich A, Leonhardt F, Werth D, Loos P. Proactive assistance for device-integrated training adjustment in outdoor rehabilitation training. Deutsches Forschungszentrum für Künstliche Intelligenz Saarbrücken: Congress Mitteilung. 2016.
18. Taylor RS, Long L, Mordi IR, Madsen MT, Davies EJ, Dalal H, et.al. Exercise-based rehabilitation for heart failure: Cochrane systematic review, meta-analysis, and trial sequential analysis. Journal of the American College of Cardiology: Heart Failure. 2019 Aug 1;7(8):691-705.
19. Graf C. Ambulante Herzgruppen in Deutchland- Ruckblick und Ausblick. Deutsche Zeitschrift für Sportmedizin. 2004;55:339-46.
20. Benzer W, Rauch B, Schmid JP, Zwisler AD, Dendale P, Davos CH, et.al. Exercise-based cardiac rehabilitation in twelve European countries results of the European cardiac rehabilitation registry. International Journal of Cardiology. 2017 Feb 1;228:58-67.
21. Steinacker JM, Liu Y, Stilgenbauer F, Nething K. Körperliches Training bei Patienten mit Herzinsuffizienz. Deutsche Zeitschrift für Sportmedizin. 2004;55(5):124- 30.
22. Williams N. The Borg rating of perceived exertion (RPE) scale. Occupational Medicine. 2017 Jul 1;67(5):404- 5.
23. Guyatt GH, Sullivan MJ, Thompson PJ, Fallen EL, Pugsley SO, Taylor DW, et.al. The 6-minute walk: a new measure of exercise capacity in patients with chronic heart failure. Canadian Medical Association Journal. 1985 Apr 15;132(8):919.