Abstract
Introduction: The most frequent distal radius malunion is secondary to a Colles’ fracture with distal radius shortening, loss of radial inclination and dorsal angulation. This deformity generates alterations in the transmission of forces in the wrist with adaptive carpal instability, osteoarthritis in the radiocarpal, midcarpal and distal radioulnar joints with ulnocarpal impaction syndrome, which requires surgical treatment. There are multiple techniques for distal radius osteotomies. The aim of this study is to present a surgical technique, the L-shaped osteotomy for distal radius malunion .
Methods: Surgical technique: The distal radius deformity is studied and the inverted L-shaped osteotomy is marked on the distal radius. It is carved the long branch of the “L” parallel to the articular surface at a distance of between 5 and 20 mm from the joint, and the short branch is carved vertically, following a groove that is formed after the radius malunion, between the metaphysis and base of the radial styloid, tangential to the healthy cortical bone of the radial diaphysis.
Discussion: This procedure is a modification to the usual technique that allows preserving bone stock in the radial column of the radius metaphysis, reducing the size of the gap, improving the contact points between both fragments of the osteotomy, by a simple distraction of the focus of the osteotomy, but also a sliding of the external cortical of the radius on the metaphysis.
Conclusion: The modification of the technique with an L-shaped osteotomy is a simple and reproducible technique, it is more anatomical and preserves more bone stock than in the conventional technique. It allows correction in all planes, reduces the requirements for structural bone grafting, allowing surgery to be performed under a regional anesthetic block and on an ambulatory procedure.
Keywords
Distal radius fracture, Distal radius osteotomy, Distal radius malunion, Bone graft
Introduction
For many years it was widely believed that the functional outcome of distal radius fractures (RDF) was usually satisfactory, even in the absence of treatment or when treatment had failed to achieve acceptable anatomic reduction [1].
Certainly, most of the patients who have suffered a RDF recover the use of the hand and can carry out most of their activities of daily living without too much difficulty. But this is not the case in young patients who have suffered high-energy trauma and have high functional demands [2]. Most distal radius fractures occur with an impaction fracture pattern and consequently with loss of cancellous bone tissue, especially in post-menopausal women with osteoporosis. This means that, even after an adequate initial reduction, the fracture becomes impacted again in the short term, despite its immobilization with a plaster cast [3]. The outcomes of fractures that resulted in malunion and current quality criteria force us to be increasingly rigorous and consider bad results many of those fractures that just two decades ago we would consider good.
Fractures in this anatomical region have a high morbidity and, on the opposite of what Colles asserted, it could almost be confirmed that in intraarticular, comminuted fractures or with large initial displacement, if the consolidation does not achieve a restitutio ad integrum of the anatomy, it would remain a functional deficit with limited range of motion of the wrist and hand, deformities, residual pain and loss of strength [1]. Malunion is the most common complication and usually occurs after a Colles fracture, either because perfect reduction was not achieved, or because it has suffered early loss of reduction or late collapse. It is common for it to happen in fractures that have not been treated properly, when loose or poorly shaped plasters were used, or after wrongly indicated osteosynthesis (K-wires in very unstable fractures) or poorly executed [4].
Malunion in extra-articular radius fractures can suffer various deformities, such as radius shortening that determines a positive ulnar variance and its consequent ulnocarpal impaction syndrome, dorsal or palmar radial angulation and loss of radial inclination [4]. These deformities alter normal load transmission causing functional limitation, adaptive carpal instability and secondary osteoarthritis that can functionally affect three joints: radiocarpal, midcarpal and distal radioulnar joint (Figure 1) [5]. Neuropathies and secondary tendon ruptures can also occur.

Figure 1. Malunion with shortening of the radius, loss of radial inclination and dorsal angulation with osteoarthritis of the radiocarpal, midcarpal, and distal radioulnar joints with ulnocarpal impaction syndrome.
The diagnosis of malunion was based on the evaluation and comparison of the normal radiological parameters described for palmar angulation, radial inclination, ulnar variance, and height of the distal radial metaphysis. Thus, altered radiological parameters with radial height loss greater than 10 mm, palmar or dorsal angulation greater than 20°, radial inclination less than or equal to 10°, ulnar variance greater than or equal to 2 mm, and joint step-off or gap greater than 2 mm, indicate the necessity of surgical correction in any of its various modalities [6]. Considering that the most frequent malunion is secondary to a Colles fracture and that the origin of the injury is the impaction of the distal radius metaphyseal trabecular bone tissue, this article describes a different osteotomy modality for extra-articular malunions and its advantages: the distal radius L-shaped osteotomy. Its formal indication is for the distal radius extra-articular malunion, in order to correct the radial shortening, the loss of radial inclination, and the dorsal or palmar angulation. The aim of this paper is to describe a surgical technique: L-shaped osteotomy for distal radius malunion.
Surgical Technique
The patient is placed in dorsal decubitus on the operating table with the upper limb abducted on a radiolucent support under axillary anesthetic block. The approach is performed following the guidelines of the modified Henry´s wrist approach [7].
The flexor carpi radialis tendon is separated to the ulnar side along with the rest of the flexor tendons, thus reaching the deep plane occupied by the pronator quadratus. It is incised in an "L" shape, leaving a sufficient margin on its radial side to carry out the reconstruction at the end of the surgery. The pronator quadratus is released for accurate visualization of the distal radius.
The distal radius deformity is studied and the inverted L-shaped osteotomy is marked on the distal radius. It is carved the long branch of the “L” parallel to the articular surface at a distance of between 5 and 20 mm from the joint, and the short branch is carved vertically, following a groove that is formed after the radius malunion, between the metaphysis and base of the radial styloid, tangential to the healthy cortical bone of the radial diaphysis.
Once the osteotomy site has been marked, it is carried out with a microsaw or osteotome, completing an additive L-shaped osteotomy (Figure 2). Once the distal radius fragment is released, the reduction is performed by traction and ligamentotaxis, guided by fluoroscopy, returning the parameters to the distal radius in terms of height, adequate palmar and ulnar inclination, observing the transformation of the L-shaped osteotomy turning into a triangle by sliding the base of the radial styloid over the metaphysis. The triangular gap resulting would be delimited by an external side constituted by the radial styloid, an upper side formed by the radial epiphysis and a base corresponding to the radial metaphysis. Its vertices would be: the union of the two segments of the "L", the contact point of the medial cortical of the radial epiphysis with the metaphysis and the contact point between the proximal end of the styloid and the metaphysis on its external edge.
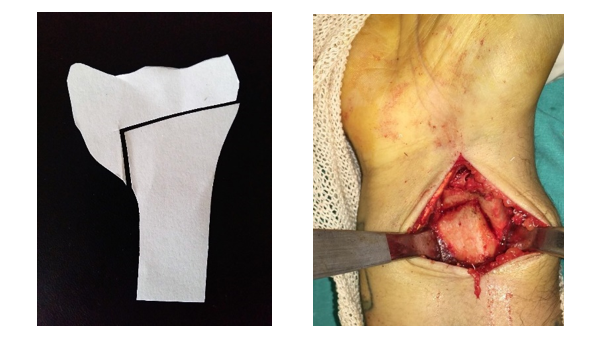
Figure 2. Delimitation of the osteotomy.
Thus, an island-shaped hole surrounded by bone is formed (Figure 3). Then, it is temporarily stabilized with Kirschner pins.
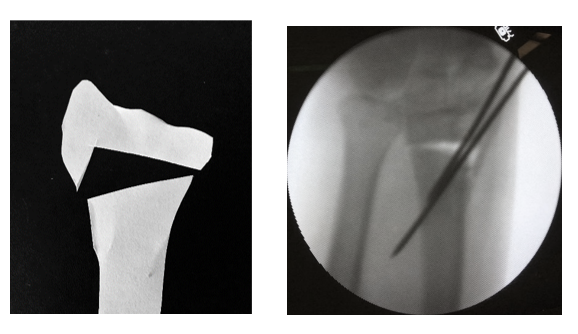
Figure 3. Reduction and shaping of a triangular gap.
With this technique, bone grafting would be unnecessary, which is one of the advantages of the L-shaped osteotomy, minimizing the gap size. The gap is completely surrounded by vascularized bone with two points of contact, preserving the bone stock. If the gap generated is very large and has a trapezoidal shape, it is recommended to use bone graft or bone substitute, according to the Orbay technique [8], pronating the proximal fragment. In this way, the bone graft or substitute remains like an island, completely surrounded by structural bone well vascularized and it requires less quantity. Reduction was verified by fluoroscopy and stabilization was carried out with a volar blocking plate for distal radius. Then we proceed to the wound closure, with repair of the pronator quadratus. A short arm plaster cast is placed, with free metacarpophalangeal joints.
Postoperative management
Immediately after surgery, the patient is immobilized with a short arm cast for 2 weeks, with mobilization finger exercises, with upper limb elevated and anti-edematous treatment. In exception for comorbidities, the procedure is performed on an outpatient basis under axillary anesthetic block with good management of postoperative pain. Prophylactic antibiotic therapy, analgesia and the beginning of physiotherapy are indicated. Two weeks later, a short thermoplastic splint with free metacarpophalangeal joints is placed and rehab begins.
Discussion
Distal radius malunion can generate biomechanical alterations in radiocarpal, midcarpal, and distal radioulnar joints, with adaptive carpal instability and ulna carpal impaction syndrome. Its best treatment is prevention, performing the appropriate treatment at the right time. Facing the diagnosis of distal radius malunion with radial shortening, loss of radial inclination or dorsal or volar angulation, the correct treatment is its surgical correction.
Until now, some distal radius osteotomy techniques and various treatments of the distal ulna have been described.
Among the most accepted techniques, osteotomy by dorsal approach has been described following the guidelines of Diego Fernández with placement of a tricortical iliac crest bone graft and stabilization with pins or dorsal plates. Although, comparative studies show better anatomical corrections than osteotomies by anterior approach, the dorsal plate has shown greater number of complications, such as extensor tenosynovitis and tendon ruptures in short and medium term, with a high incidence of reoperation to remove osteosynthesis material [9,10].
With the advent of the most modern locking volar plates, the most widely used surgical technique has been the additive stabilized osteotomy with the locking volar distal radius plate, with more and more adherents to this technique without bone grafting.
According to Malone et al. [ 11], the rigidity of locking distal radius volar plates provides us with sufficient stability to avoid the use of tricortical bone graft.
Donor site morbidity is well documented, specially the iliac crest, with complications such as graft harvesting site residual pain, hematoma or seroma, wound infection and regional sensory nerve injury. In addition, surgery time is prolonged, requiring general anesthesia, increasing the hospital length stay to at least 24 hours.
Another advantage of using volar distal radius plates is their simpler approach, with direct vision and that the osteosynthesis plate is deeply lodged, covered by the quadratus pronator, with fewer complications on the tendons compared to the placement of dorsal plates.
The L-shaped osteotomy is a modification to the usual technique that allows to preserve bone stock in the metaphysis radial column, reducing the size of the gap, improving the contact points between both fragments of the osteotomy, as it is performed with a simple distraction of the osteotomy site, but also, a sliding of the external radial cortical on the metaphysis. In this way, the gap generated is triangular and surrounded by bone, both distally and proximally, as well as laterally and medially.
Several studies question the need to use bone graft, as described in publications of Wieland, Malone, Prommersberger, Tarallo, and Mahmoud, where the cancellous bone great healing capacity in the radius metaphysis highlighted the importance of the triangular or trapezoidal shape gap generated after reduction of the osteotomy [5,11-14]. The gap shape assures the presence of at least one contact point after the distal radius osteotomy. The trapezoidal gap shape has a higher rate of delayed fracture healing and pseudoarthrosis, meanwhile in all published series, the triangular gap has shown optimal healing [15]. After the L-shaped osteotomy, a medial and a lateral contact point would be formed, with bone stock preservation, a technique performed by volar approach, in a simple and reproducible manner, without the comorbidities that implies obtaining an iliac crest bone graft, being able to perform the procedure on an outpatient basis with a regional anesthetic block.
Conclusion
Faced with an extra-articular distal radius malunion diagnosis, understanding this condition with radius shortening, radial inclination loss and dorsal or volar angulation, controlled osteotomy fixed with locking volar distal radius plate has shown very good results and fewer complications compared to dorsal stabilized osteotomy. Bone graft use is not mandatory, but if a trapezoidal gap is generated after the osteotomy, it would be advisable to add some graft. The technique modification with an L-shaped osteotomy is a simple, reproducible and more anatomical procedure, with more bone stock preservation than in the conventional technique. It lets us correct malunion in all planes, it reduces the structural bone graft requirements, allowing surgery to be performed under a regional anesthetic block and on an ambulatory basis procedure.
References
2. Irisarri C. Controversias en el tratamiento de las fracturas de la extremidad distal del radio. Pat Apto Locomotor. Madrid: Fundación Mapfre. 2007;5(Supl II): 34-40.
3. Charnley J. The closed treatment of common fractures. Baltimore: Williams & Wilkins. 1961.
4. D ´Elia M, Amico RA, Maio J, Capomassi M. Consolidaciones viciosas del radio distal. Rev Asoc Arg Ortop y Traumatología. 2001; 67(1)27- 32.
5. Tarallo L, Mugnai R, Adani R, Catani F. Malunited extra-articular distal radius fractures: corrective osteotomies using volar plate. J. Orthop Traumatol. 2014;15(4):285-290.
6. Evans BT, Jupiter JB. Best Approaches in Distal Radius Fractures Malunions. Current Reviews in Musculoskeletal Medicine. 2019;12:198-203.
7. Henry AK. Extensible Exposure. 2nd Ed. Baltimore: Williams and Wilkins. 1957;67.
8. Orbay J. Volar plate fixation of distal radius fractures. Hand Clin. 2005;21:347-354.
9. Fernández DL. Distal radius fractures. Reconstructive procedures for malunion and traumatic arthritis. Orthop Clin North Am. 1993;24: 341-63.
10. Oka K, Kataoka T, Tanaka H, Okada K, Yoshikawa H, MuraseT. A comparison of corrective osteotomies using dorsal and volar fixation for malunited distal radius fractures. International Orthopaedics. 2018;42(12):2873-2879.
11. Malone Kj, Magnell TD, Freeman DC, Boyer MI, Placzek JD. Surgical correction of dorsally angulated distal radius malunions with fixed angle volar plating: a case series. J Hand Surg Am. 2006;31(3):366-372.
12. Prommersberger KJ, Lanz UB. Corrective osteotomy of the distal radius through volar approach. Tech Hand Up Extrem Surg. 2004;8(2):70-77.
13. Mahmoud M, El Shafie S, Kamal M. Correction of dorsally-malunited extra articular distal radial fractures using volar locked plates without bone grafting. J Bone Joint Surg Br. 2012;94(8):1090-6.
14. Wieland AW, Dekkers GH, Brink PR. Open wedge osteotomy for malunited extra articular distal radius fractures with plate osteosynthesis without bone grafting. Eur J Trauma. 2005;31(2):148-53.
15. Scheer JH & Adolfsson LE. Non-union in 3 of 15 osteotomies of the distal radius without bone graft. Acta Orthopaedica. 2015;86(3):316-320.