Abstract
Background: The provision of comprehensive care and support services to orphans and disadvantaged children that are individualized and tailored through the use of child- and family-centered information is critical but little if any information is available on satisfaction with HIV/AIDS care among orphans and vulnerable children in Gondar. Therefore, this study aimed to assess the satisfaction of HIV/AIDS care and support service delivered to caregivers of Orphans and Vulnerable Children, Gondar City, 2023.
Methods: A facility-based cross-sectional study design with explanatory concurrent mixed methods was applied. A total of 424 Orphans and Vulnerable Children’s caregivers for interviewer-administered questionaries, 5 key informant interviews, and 385 Orphans and Vulnerable Children’s document reviews were conducted. The data were entered into the Kobo toolbox software and exported to STATA version 16 for analysis. A binary logistic regression analysis was performed to identify significant variables. The qualitative data were transcribed, translated, coded, and analyzed using thematic analysis.
Results: In this study, the Orphans and Vulnerable Children’s/ caregivers satisfaction of HIV/AIDS C&S services was 68.20% with (95%CI=63.20%,71.10%). In multivariable logistic regression analysis, separate waiting rooms (AOR=0.05, 95% CI: 0.005, 0.52), materials for Orphans and Vulnerable Children to take home (AOR=1.76, 95%CI: 1.67, 7.59), and provisions of attractive and friendly services to Orphans and Vulnerable Children (AOR=2.24, 95%CI: 1.08, 4.64) were significant variables.
Conclusion: Orphan and vulnerable children caregiver satisfaction to HIV/AIDS C&S service was 68.20% with (95%CI=63.20%,71.10%). Separate waiting rooms, attractive and friendly service, and materials to take home were factors that affected Orphans and Vulnerable Children’s caregiver satisfaction to the HIV/AIDS C&S service. Rigorous efforts to build systems that apply the policy and principles of HIV C&S services are recommended. Therefore, the government, partners, programmers, and implementers should give attention to improving the HIV C&S services.
Keywords
Satisfaction, HIV/AIDS care and support services, Orphans and Vulnerable Children
Introduction
Concern regarding orphans and vulnerable children (OVC) under the age of 18 is growing on a global scale. These kids lost one or both of their parents. Many more children are raising one or more parents who are chronically ill, according to the United Nations Children Fund and the United States Agency for International Development (USAID). Sub-Saharan Africa (SSA) is where the vast majority of these OVC are from [1,2]. Globally, 15.4 million children under the age of 17 are expected to have lost one or both parents to AIDS by 2020. In 2020, it is estimated that 1.7 million children under the age of 14 were living with HIV. Children alone account for 40% of those receiving HIV treatment for viral suppression [3].
More than 12% of all children in Ethiopia are affected due to the death of one or both parents due to HIV/AIDS [4]. HIV/AIDS has changed the way millions of children are raised in Ethiopia, including Gondar, because it is no exception. Many are cared for by widowed or sick parents, while others live with large families [5]. In Ethiopia, about 6% of the total population, is classified as OVC [4]. According to the report of Yecokeb Berehan, there are an estimated 13,234 OVC in Gondar [6].
HIV/AIDS care and support (C&S) services for orphaned and vulnerable children are high among international agencies and donors working to improve the well-being of OVC in the order of the whole world [7]. OVC living with HIV/AIDS treatment gaps exist in many SSA nations to a higher extent with treatment rates ranging from 12-48 percent [8].
To address this problem, Ethiopia has several community-based OVC-related organizations at the grassroots level. The primary goal of this program is to provide comprehensive, individualized, and tailored care to local HIV OVC and their households, ensuring that OVC households achieve financial stability and child well-being outcomes [9].
Early infant diagnostic testing is similarly lacking, with only 52 percent of HIV-exposed infants tested by two months of age in high-burden countries, mostly in SSA [10]. Other methods of HIV testing to identify HIV-infected children include routine pediatric outpatient screening, sibling and congenital screening of patients enrolled in HIV care targeting them, screening in the community, and by providing vaccination after the event Integration with other initiatives and research as part of it have stopped programs to prevent mother-to-child transmission of HIV [11,12].
HIV testing challenges at the facility level, such as those related to access and confidentiality, may be addressed by home-based techniques [13]. Other impediments, such as fear of the stigma associated with HIV-positive diagnosis, will exist, and HIV services delivered at home could pose further challenges [13-15]. While there is little published evidence on the extent to which screening questions are asked with the magnitude of HIV/AIDS care service satisfaction targeted to OVC in their home environments [16].
Satisfaction with the delivery of HIV/AIDS C&S services to OVC programs in ANPPCAN is low despite the fact that HIV/AIDS prevention and control is a priority program of the national or global health community. Additionally, it will be used as an HIV/AIDS investment in Gondar, northwestern Ethiopia.
Methods
Study area and period
The study was conducted in Gondar City at ANPPCAN health facility from May 01/2023 to June 01/2023. Gondar is located 750 kilometers away from Addis Ababa. While according to the Central Statically Agency’s population projection, the population of Gondar City was estimated to increase to 323,875 by 2015 and 360,600 in 2017. Out of this 13,234 were OVC [6]. ANPPCAN-Ethiopia is the only NGO that has been implementing family-focused HIV/AIDS C&S services to OVC in Gondar City.
Study design
A facility-based cross-sectional study design with explanatory concurrent mixed-method was employed. Qualitative and quantitative data were collected concurrently, analyzed separately, and integrated during the interpretation of findings.
Population
Vulnerable children, caregivers and OVC C&S service documents were considered as a source population. Caregivers of OVC and key informants who were available during data collection period were study population as well as selected OVC C&S registered documents from the last one year were study population.
Inclusion criteria
Caregivers of OVC greater than18 year’s old and key informants who were working in their respective SDP for the last 6 months were included in the study.
Sample size
It was determined by using single population proportion formula by taking p=50%, because there is no previously similar study done in the country, margin of error, d=0.05 and 95% confidence interval. So, the final sample size with non-response rate was 424.
For key informant interview
The key informants were ANPPCAN project manager, OVC specialist, community social workers, and community HIV/AIDS linkage coordinators. A total of five key informant interviewers participated in the study.
For retrospective document review
A total of 385 OVC documents were reviewed from June 01/ 2022 to June 01/2023 (one year document review) was included in the evaluation.
Sampling procedure
In Gondar City administration, ANPPCAN is implementing the HIV/AIDS C&S services in six sub-cities each has one SDP (Fasil, Mehal Arada, Jantekel, Zobel, Maraki and Azezo). Finally, three SDP from three sub cites (Fasil, Maraki and Azezo) were randomly selected. Then, the sample size was proportionally allocated according to the size of the population in each SDP to get representative participants in each selected SDP. Finally, caregivers of OVC were selected by systematic random sampling technique, in all working hours of the week during the data collection period in each SDP (Figure 1).
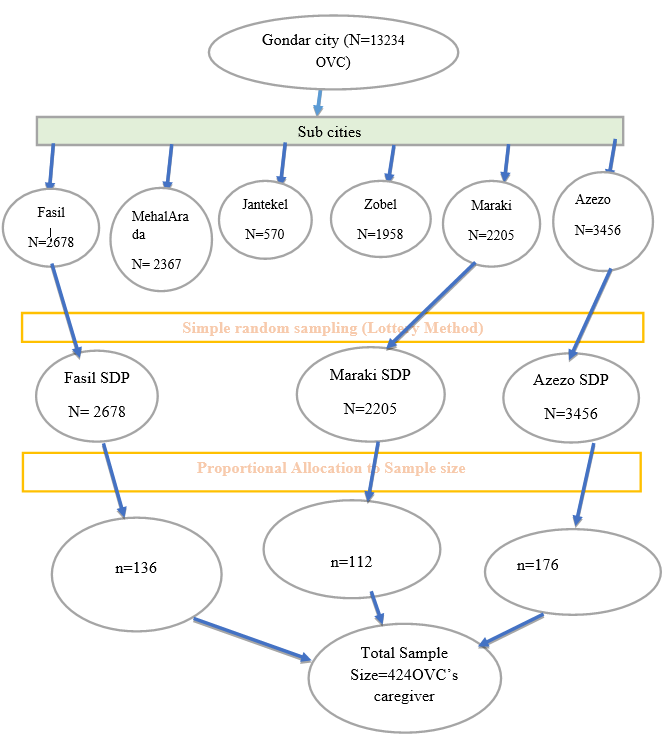
Figure 1. Diagrammatical presentation of sampling procedure of selecting caregivers of OVC for interview to assess to HIV/AIDS C&S services satisfaction in ANPPCAN, Gondar City, 2023.
Measurements
Caregiver of OVC satisfaction: Refers to how OVC and their caregiver’s level of engagement in HIV/AIDS C&S services [17]. It was measured using eight “yes” or “no” response questions. We used the above mean score (5.06) to say high, otherwise low satisfaction to the service.
An orphan child: Is defined as a child under the age of 18 who has lost one or both parents, regardless of the reason for the loss. An orphan can be maternal, paternal, or double [18-20].
A vulnerable child: Is a child under the age of 18 whose existence, care, protection, or development may be compromised due to a certain condition. Vulnerable children can be those with a chronically ill patient (mother or father) who is very sick for 3 or more months [20,21].
Data collection tools and procedures
Data was collected using an interviewer-administrated structured questionnaire. The instrument was developed by reviewing different literatures and modified to the local context. Two (2) data collectors, a BSC nurse and a BSC nurse supervisor were assigned.
Key informant interviews were conducted by principal investigator using semi-structured questionnaires which were held in a private place to maintain privacy with effective probes. Then the interview was tape recorded and scripted using Amharic language. Transcription, translation, and format were carried out on the same day of the interview. The average time taken for the interview was 65 minutes and proper note was taken and final transcripts contained both Amharic and English versions.
Data quality control
To ensure the quality of data, pretested was done in 21(5%) of the sample size in a non-selected sub-city (Mehal Arada) that has similar contexts to the selected sub-cities in Gondar City. A two-day training was given about questionnaires. Prior to analysis, data was cleaned up and cross-checked. The principal investigator and the supervisor closely monitored the process throughout the data collection period and made due corrections. The credibility of the data was determined through triangulation of data between methods of data collection and recruitment of appropriate interviewees was considered, and the participants’ voice was inserted in the result to check its accuracy.
Data management and analysis
The filled questionnaires were exported from open data kit/ODK to STATA version 16 for further analysis. Descriptive and summary statistics were presented in the form of text and tables. Multi-co linearity was checked using variance inflation factor (VIF), which was 1.68. Internal consistency reliability of instrument was checked to show the internal homogeneity of items using Cronbach’s alpha, which was 0.83. We assessed the goodness of fit for the corresponding model using the Pearson goodness-of-fit which was insignificant (p- value=0.16), therefore our model is a good fitted model.
Analysis of transcript data was done by Open code software. After coding of the participants’ similar ideas, codes were formed into themes based on their similarity of ideas and the theme. The data was analyzed by thematic analysis based on its relatedness, and direct quoting was undertaken. During this process, codes were regrouped in the codebook to reflect the ongoing emergence of themes. Finally, the results were supplemented with the respective dimensions.
Ethical clearance
Ethical clearance was obtained from the University of Gondar, the Institute of public health Ethical Review Committee with reference number IPH/2254/2014. Official permission was obtained from ANPPCAN health institution. Oral informed consent was obtained from caregivers of OVC. Moreover, confidentiality was maintained through anonymity and privacy measures to protect respondent’s rights through the research process. Moreover, respondents were informed about their right to withdraw from the study at any time and they could not be harmed by doing so.
Result
Of the total 424 caregivers of OVC, 415 (97.8%) responded to the self-administered exit interview. The mean age of OVC was 12.75 and 255 (61.45%) were males. Regarding their residence, 339 (81.69%) were urban residents and 332 (80%) were Orthodox Christians. Concerning their educational status, 268 (64.58%) of them were attending primary education (grade 1–8) (Table 1).
|
Variables |
|
Frequency |
Percentage |
|
Sex |
Male |
255 |
61.45 |
|
Female |
160 |
38.55 |
|
|
Religion |
Orthodox |
332 |
80 |
|
Muslim |
78 |
18.8 |
|
|
Others |
5 |
1.2 |
|
|
Residence |
Urban |
339 |
81.69 |
|
Rural |
76 |
18.31 |
|
|
Work for money |
Yes |
227 |
54.70 |
|
No |
188 |
45.30 |
|
|
Educational status |
Primary Education |
268 |
64.58 |
|
Secondary Education |
142 |
34.22 |
|
|
Unable to read and write |
2 |
0.48 |
|
|
Able to read and write |
3 |
0.72 |
|
|
Other=protestant and Catholic |
|||
Document review
Of 385 OVC documents, 310 OVC were referred for HIV testing to community HIV/AIDS linkage coordinator from social workers. The sub population code, HIV status of mother and criteria of OVC for HIV testing referral were not fully registered. Among those who were referred for HIV testing, seven out of 310 OVC documents were not attached to their respective referrals slip.
Social and community level workers register each OVC age, current HIV status, HIV status of mother, date of HIV testing but few social and community level workers miss to document sub population code, referral slip attached, and criteria of OVC for HIV testing referral on family HIV risk assessment and HIV status tracking tool. This is antagonist to the key informant findings:
“…We all social and community workers of the institution must document each OVC related characteristics well and neatly. If there exist miss registered variables, we were not considered as a hard worker. To have good name in this institution, we always strived to had good documentation.’’ [25 years Female social worker]
Factors affecting satisfaction for respondents
In simple binary logistic regression analysis; religion, residence, children asked their problem, counseling area kept visual privacy, separate waiting room, adequate waiting room, educational posters that describe clients’ rights, materials for OVC clients to take home, service provision attractive and friendly to OVC, continuous support to OVC C&S services and presence of clear, written guidelines or SOP had a p-value <0.25 were considered as candidate variables for multivariable analysis.
Caregiver of OVC who get HIV/AIDS C&S service in SDP which has no separate waiting room had 95% less likely to be satisfied compared to SDP having a separate waiting room (AOR=0.05, 95% CI: 0.005,0.52).
The odds of caregiver of OVC satisfied to HIV/AIDS C&S service who took readable materials to their home was 1.76 times compared to SDP which have no materials for OVC clients to take home (AOR=1.76, 95%CI: 1.67, 7.59).
The odds of caregiver of OVC satisfaction to HIV/AIDS C&S service getting attractive and friendly service to their OVC were 2.24 times higher compared with those caregivers of OVC that didn’t get attractive and friendly service in HIV/AIDS C&S service (AOR=2.24, 95%CI: 1.08, 4.64) (Table 2).
|
Variables |
Satisfaction |
OR |
||||
|
|
Yes (%) |
No (%) |
COR (95% CI) |
P value |
AOR (95% CI) |
P-Value |
|
Religion |
|
|
|
|
|
|
|
Orthodox |
221 (66.6) |
111 (33.4) |
1 |
|
1 |
|
|
Muslim |
59 (75.6) |
19 (24.4) |
1.55 (0.88,2.74) |
0.12 |
1.62 (0.9,2.91) |
0.11 |
|
Other |
3 (60) |
2 (40) |
0.753 (0.12,4.57) |
0.76 |
0.84 (0.13,5.35) |
0.86 |
|
Residence |
|
|
|
|
|
|
|
Urban |
236 (69.6) |
103 (30.4) |
1 |
|
1 |
|
|
Rural |
47 (61.8) |
29 (38.2) |
0.7 (0.42, 1.18) |
0.19 |
0.76 (0.44,1.33) |
0.34 |
|
Asked OVC problem |
|
|
|
|
|
|
|
Yes |
200 (66.2) |
102 (33.8) |
0.7 (0.43, 1.14) |
0.16 |
0.86 (0.51,1.45) |
0.58 |
|
No |
83 (73.5) |
30 (26.5) |
1 |
|
1 |
|
|
Counseling area visual privacy |
|
|
|
|
|
|
|
Yes |
197 (66.3) |
100 (33.7) |
0.73 (0.45, 1.17) |
0.19 |
0.73 (0.44, 1.2) |
0.22 |
|
No |
86 (72.9) |
32 (27.1) |
1 |
|
1 |
|
|
Waiting room |
|
|
|
|
|
|
|
Yes |
273 (68.8) |
124 (31.2) |
1 |
|
1 |
|
|
No |
10 (55.6) |
8 (44.4) |
0.57 (0.21, 1.47) |
0.23 |
0.05 (0.01,0.52) |
0.012** |
|
Materials to take-home |
|
|
|
|
|
|
|
Yes |
244 (66.5) |
123 (33.5) |
1 |
|
1 |
|
|
No |
39 (81.2) |
9 (18.8) |
2.18 (1.02, 4.65) |
0.04 |
1.76 (1.67,7.59) |
0.014** |
|
Posted clients rights |
|
|
|
|
|
|
|
Yes |
223 (66.8) |
111 (33.2) |
0.66 (0.38, 1.15) |
0.15 |
1.17 (0.69,1.98) |
0.55 |
|
No |
60 (75) |
20 (25) |
1 |
|
1 |
|
|
Adequate waiting room |
|
|
|
|
|
|
|
Yes |
204 (70.3) |
86 (29.7) |
1.38 (0.88, 2.14) |
0.15 |
1.3 (0.82,2.09) |
0.26 |
|
No |
79 (63.2) |
46 (36.8) |
1 |
|
1 |
|
|
Friendly service |
|
|
|
|
|
|
|
Yes |
266 (70) |
114 (30) |
2.47 (1.23, 4.97) |
0.01 |
2.24 (1.08, 4.64) |
0.03** |
|
No |
17 (44.7) |
18 (55.3) |
1 |
|
1 |
|
|
Support services |
|
|
|
|
|
|
|
Yes |
205 (65.5) |
108 (34.5) |
0.58 (0.35, 0.98) |
0.04 |
0.69 (0.4, 1.2) |
0.29 |
|
No |
78 (76.5) |
24 (23.5) |
1 |
|
1 |
|
|
Guidelines existing |
|
|
|
|
|
|
|
Yes |
274 (67.7) |
131 (32.3) |
0.23 (0.03, 1.85) |
0.17 |
0.46 (0.05,4.21) |
0.49 |
|
No |
9 (90) |
1 (10) |
1 |
|
1 |
|
|
CI: Confidence Interval; COR: Crude Odds Ratio; AOR: Adjusted Odds Ratio |
||||||
This was supported by the key informant interview:
“…Even though we had HIV diagnostic testing kit, OVC register, referral slip form, information, education and communication materials, and risk assessment screening tool which are essential materials that used us for C& S services for our OVC program, there exist “on and off” of this material. This was due to budget deficit. Final that makes them not satisfied towards the service.” [38 years Male, Program Manager]
“…. Care and support service providers are expected to conduct C&S services based on national standard OVC C&S guidelines which was printed and donated for us from USAID.” [41 years male OVC specialist]
“…Almost all C&S providers were given essential capacity development training to perform their activity adhere to this national guideline. Only one SDP had essential SOP.” [41 years male OVC specialist]
“…Initially during staff recruitment process, we were considering C&S service providers educational status and their direct work experience on OVC project to be considered that they are capable of managing the project properly after joining this project. When there exists update on algorism, staff got capacity building training.” [38 years male program manager]
“…Participation of the community particularly community coalition committee members, who were selected from the community, local administration and other stakeholders has helped ANPPCAN to identify the target beneficiaries and subsequently deliver appropriate services. The community engagement in implementing the project at local level has created a sense of ownership, trust and belongingness which in turn would ensure sustainability of the C&S services and as the result clients satisfied by its service.” [38 years old, Male, program manager]
Discussion
This research is consistent with existing literature. The existing literature showed HIV/AIDS remains the leading cause of morbidity and mortality worldwide. Moreover, sub-Saharan countries, including Ethiopia, are highly affected by HIV/AIDS pandemic. Ethiopia’s government has been working on a comprehensive HIV care and treatment program, including antiretroviral therapy. However, evaluating client satisfaction with antiretroviral treatment services is not well studied.
Several studies have been conducted to assess client satisfaction and associated factors with antiretroviral treatment services provided at public health facilities in the Ethiopia region. Various research studies showed that overall client satisfaction with antiretroviral treatment services was lower than the national target of 85%. Sex parameters such as male and employment were positively associated with clients’ satisfaction with ART services among socio-demographic characteristics, or both are the determinants for client satisfaction with ART services. The availability of prescribed laboratory services, prescribed drugs, and the cleanliness of toilets in the facility were factors associated with client satisfaction with antiretroviral treatment services. Studies showed that the tangibility aspects of the client’s response on the cleanliness of toilets in the facility are poor, or toilets in those health facilities were dirty or unclean. Procurement and supply for the availability of laboratories and medicine require attention. Sex-sensitive programs should be considered to improve client satisfaction. Further studies are needed, including the clinical characteristics of ART clients.
In the given study, Orphan and vulnerable children caregiver satisfaction with HIV/AIDS C&S service was 68.20%. Various factors such as separate waiting rooms, attractive and friendly service, and materials to take home impacted the Orphans and Vulnerable Children’s caregiver satisfaction with the HIV/AIDS C&S service. No doubt, strong measures are required to build systems that apply the policy and principles of HIV C&S services. which shows the program needs improvement. This was relatively higher than the comparative studies conducted in Gondar City [22], Bahir Dar City [23], and Dessie City [24]. This may be because most SDP had access to medical staff who have received training on national consolidated recommendations for all-inclusive HIV prevention, care, and treatment. This finding was lower than evaluation conducted by United states Department of Defense and Health Resource and Service Administration [25]. The possible explanation for the difference finding might be difference in economic status, difference in study setting and health system between the United States of America and Ethiopia. On the other hand, this finding was higher than evaluation study conducted by prevention research center which showed that 59% [26]. The possible difference could be due to changes in HIV/AIDS services, caregiver experience, or related policies between study periods that may affect satisfaction levels, effectiveness of services in subsequent assessments, satisfaction may increase, and sample characteristics and methods can contribute to change.
But the above finding was not in line with guideline recommendation which says programs should seek to enhance the participation of all beneficiaries and their caregivers [19]. OVC and their families should participate, to the fullest extent of their capacities, through the entire project cycle of planning, implementing, monitoring, and evaluating. Participation increases satisfaction to the service of the child and his or her families and improves the likelihood of making a measurable difference in their lives [27]. The possible explanation for this gap may be due to awareness and care provider may not motivate /encourage OVC’s care giver to participate throughout the project life.
According to document review result, social and community level workers miss to document/attach sub population code, referral slip and criteria of OVC for HIV testing referral on family HIV risk assessment and HIV status tracking tool. A possible reason for this finding might be due to social workers’ lack of concentration and poor documentation skill.
Caregiver who gets HIV/AIDS C&S service to their OVC in SDP which has no separate waiting room are 95% less likely to be satisfied compared to SDP having a separate waiting room (AOR=0.05, 95% CI: 0.005,0.52). We can also interpret this finding as: Caregivers getting HIV/AIDS C&S service for their OVC in SDP which has separate waiting room are 5% more likely to be highly satisfied compared to SDP which has no separate waiting room. This finding was supported by a study conducted in the USA where those OVC who were served by health facilities that had a separate waiting room showed a better care on retention among HIV-infected OVC [28,29]. Besides, this finding is in line with the WHO quality assessment standard [29,30] that stated as the presence of separate waiting room for the C&S services enhances the intervention delivery with a better response. A possible explanation could be, usually waiting rooms for OVC/caregivers are equipped with many educational materials like visual and audio, leaf lets, television, posters and even peer educators there. Hence, OVC/caregivers in the waiting area have better information on the HIV/AIDS C&S services available, how to approach the C&S providers and the like [29,30]. In addition, separate waiting rooms allow OVC/caregiver to be kept from visual and auditory privacy from adult clients and that may increase OVC/caregivers confidence on seeking the HIV/AIDS C&S and hence all the above may contribute to get the OVC/caregivers highly responsive to the deliverable services [28-30].
The odds of caregiver of OVC satisfaction to HIV/AIDS service getting attractive and friendly service to their OVC were 2.24 times higher compared with counterpart (AOR=2.24, 95%CI: 1.08, 4.64). This finding was in line with Family health international 360 [31] and national standard OVC C&S guidelines [19] which states Programs must encourage service users to make services more child-friendly. The possible explanation for this finding could be when the caregiver of OVC getting attractive and friendly service, they may be highly motivated and satisfied by the service delivered for their OVC as well as they may become happy with the care provider. This makes them come to SDP frequently to obtain their need-based services.
The odds of caregiver of OVC satisfaction to HIV/AIDS C&S services who took readable materials to their home was 1.76 times higher compared to caregiver of OVC who did not took readable materials to their home (AOR=1.76, 95%CI: 1.67, 7.59). This was supported by key informants as:
“…We all think that each SDP should had all necessary IEC/BCC readable materials that could enhance HIV/AIDS knowledge for each OVC/caregivers who came to our SDP for certain HIV/AIDS related services. This directly had effect on caregiver of OVC participation to C&S service because they had information about what type of service provided in each SDP after reading these IEC/BCC materials.” [28 years old, male, community linkage coordinator]
The possible explanation might be that when OVC and care givers took readable material from SDP to their home, their attitude and awareness towards the service may become positive and this also enable them to take services without interruption.
Strength and limitations of study
The study was triangulated with a qualitative design, which explores in-depth reasons for the satisfaction of HIV/AIDS C&S services. It assessed different factors for satisfaction of HIV/AIDS C&S services among OVCs’ and was being the 1st in kind in Ethiopia targeting them with validated and comprehensive tool, which provides updated information. However, during document review unworked activities may be typed as worked. This may give an inflated result.
Conclusion
OVC caregiver satisfaction to HIV/AIDS C&S service was 68.20% with (95%CI=63.20%,71.10%). Separate waiting rooms, attractive and friendly service, and materials to take home were factors that affect caregiver of OVC satisfaction to the HIV/AIDS C&S service. Hence, this study generates new evidence by showing the actual program-level performance of HIV/AIDS C&S services for OVC which was used as an input to strengthen the HIV C&S service. Rigorous efforts to build systems that apply the policy and principles of HIV C&S services in the NGO are recommended. Therefore, the government, partners, programmers, and implementers should give attention on improving the HIV C&S services.
Abbreviations
AIDS: Acquired Immunodeficiency Syndrome; ANPPCAN: African Network for Prevention and Protection Children Against Neglect; AOR: Adjusted Odd Ratio; ART: Anti-Retroviral Treatment; CDC: Centers for Disease Control and Prevention; CI: Confidence Interval; COR: Crude Odd Ratio; HIV: Human Immune-deficiency Virus; OVC: Orphan and Vulnerable Children; PEPFAR: President Emergency Plan Fund for AIDS Relief; SDP: Service Delivery Point; VCT: Voluntary Counseling and Testing; WHO: World Health Organization
Consent for Publication
Not applicable.
Availability of Data and Materials
Data is available upon reasonable request from the corresponding author.
Competing Interests
All authors declared that they have no competing interest.
Funding
No funding for this project.
Authors’ Contribution
Conceptualization: LA & ZY, data curation: LA & TA, formal analysis: LA, investigation: LA &ZY, methodology: LA, software: LA, validation: LA, visualization: LA &TA, writing original draft: LA & TA, writing review & editing: LA & ZY. All authors contributed to the article and approved the submitted version accordingly based on the above descriptions.
Acknowledgments
We would like to thank the University of Gondar and Institute of public health, Department of Health system and Policy as well as Gondar administration city women’s affair office for their cooperation and permission to conduct the study. We are also grateful to all respondents, data collectors, and supervisors for providing valuable time and necessary information for this research.
References
2. Gitonga GK. An assessment of factors that influence the management of quality care to orphans and vulnerable children (Doctoral dissertation).
3. UNAIDS DJRF. Report. 2021.
4. Abashula G, Jibat N, Ayele T. The situation of orphans and vulnerable children in selected Woredas and towns in Jimma Zone. International Journal of Sociology and Anthropology. 2014 Sep 1;6(9):246.
5. Thurman TR, Jarabi B, Rice J. Caring for the caregiver: evaluation of support groups for guardians of orphans and vulnerable children in Kenya. AIDS Care. 2012 Jul 1;24(7):811-9.
6. Report UJEE. Yekokeb Berhan Program for Highly Vulnerable Children in Ethiopia. Pact Ethiiopia Addis Ababa; 2017.
7. Crivello G, Chuta N. Rethinking orphanhood and vulnerability in Ethiopia. In: Child Protection in Development. Routledge; 2014. pp. 100-112.
8. Chamie G, Napierala S, Agot K, Thirumurthy H. HIV testing approaches to reach the first UNAIDS 95% target in sub-Saharan Africa. The Lancet HIV. 2021 Apr 1;8(4):e225-36.
9. Bandason T, McHugh G, Dauya E, Mungofa S, Munyati SM, Weiss HA et.al. Validation of a screening tool to identify older children living with HIV in primary care facilities in high HIV prevalence settings. AIDS (London, England). 2016 Mar 3;30(5):779.
10. UNAIDS JUNPoHAJG. Start Free Stay Free AIDS Free-2019 report. 2019.
11. World Health Organization. The voices, values and preference of adolescents on HIV testing and counselling: consultation for the development of the World Health Organization HIV testing and counselling guidelines for adolescents. World Health Organization; 2013.
12. Ahmed S, Kim MH, Sugandhi N, Phelps BR, Sabelli R, Diallo MO, et.al. Beyond early infant diagnosis: case finding strategies for identification of HIV-infected infants and children. AIDS (London, England). 2013 Nov;27(0 2):S235.
13. Gill MM, Jahanpour O, van de Ven R, Barankena A, Urasa P, Antelman G. HIV risk screening and HIV testing among orphans and vulnerable children in community settings in Tanzania: Acceptability and fidelity to lay-cadre administration of the screening tool. Plos one. 2021 Mar 25;16(3):e0248751.
14. Merten S, Ntalasha H, Musheke M. Non-uptake of HIV testing in children at risk in two urban and rural settings in Zambia: a mixed-methods study. PloS One. 2016 Jun 9;11(6):e0155510.
15. Kurth AE, Lally MA, Choko AT, Inwani IW, Fortenberry JD. HIV testing and linkage to services for youth. Journal of the International AIDS Society. 2015 Feb;18:19433.
16. Kalichman SC, Hudd K, DiBerto G. Operational fidelity to an evidence-based HIV prevention intervention for people living with HIV/AIDS. The Journal Of Primary Prevention. 2010 Aug;31:235-45.
17. Carroll C, Patterson M, Wood S, Booth A, Rick J, Balain S. A conceptual framework for implementation fidelity. Implementation Science. 2007 Dec;2:1-9.
18. UNICEF. Africa's Orphaned and Vulnerable Generations: Children Affected by AIDS. UNICEF; 2006.
19. Federal Democratic Republic of Ethiopia MoWsA, Prevention FHA, Office C. Standard service delivery guidelines for orphans and vulnerable children's care and support programs. Ministry of Women, Children, and Youth Affairs Addis Ababa, Ethiopia; 2010.
20. Gondel A. ASSESSING THE MULTI-SECTORAL RESPONSE OF HIV/AIDS-T HE ROLES OF HIV/AIDS COMMITTEE ON PROVISION OF CARE AND SUPPORT WITH SPECIAL EMPHASIS IN CARING HIV/AIDS ORPHAN AND VULNERABLE C HILDREN-CHALLENGES AND PROSPECTS-THE CASE OF FITCHE TOWN (Doctoral dissertation, St. Mary's University).
21. Padian NS, Holmes CB, McCoy SI, Lyerla R, Bouey PD, Goosby EP. Implementation science for the US President's Emergency Plan for AIDS Relief (PEPFAR). JAIDS Journal of Acquired Immune Deficiency Syndromes. 2011 Mar 1;56(3):199-203.
22. Azanaw A, Alemu MB, Yitayal M, Aschalew AY. Evaluation of the pediatric antiretroviral therapy service in Gondar city public health facilities—A case study design with mixed methods. Plos One. 2022 Dec 30;17(12):e0279890.
23. Alemayehu YK, Bushen OY, Muluneh AT. Evaluation of HIV/AIDS clinical care quality: the case of a referral hospital in North West Ethiopia. International Journal for Quality in Health Care. 2009 Oct 1;21(5):356-62.
24. Fentaye FW, Kumar P. Grading the Level of Adherence to the Care and Treatment of Providers and Clients on Antiretroviral Therapy Program in Dessie Referral Hospital. South Wollo, Ethiopia. IOSR Journal of Dental and Medical Sciences (IOSR-JDMS). 2019;18(1):5-8.
25. Hiv TL. PEPFAR looks to the future. The Lancet HIV. 2022 Jun 1;9(6):e367.
26. Domitrovich CE, Greenberg MT. The study of implementation: Current findings from effective programs that prevent mental disorders in school-aged children. Journal of Educational and Psychological Consultation. 2000 Jun 1;11(2):193-221.
27. PEPFAR. Orphans and other vulnerable children programming guidance for United States Government in-country staff and implementing partners. Office of the Global AIDS Coordinator Washington, DC; 2006.
28. Lee L, Yehia BR, Gaur AH, Rutstein R, Gebo K, Keruly JC, et.al. The impact of youth-friendly structures of care on retention among HIV-infected youth. AIDS Patient Care and STDs. 2016 Apr 1;30(4):170-7.
29. Habitu YA, Biks GA, Worku AG, Gelaye KA. Individual and contextual factors affect the implementation fidelity of youth-friendly services, northwest Ethiopia: A multilevel analysis. Plos One. 2022 Feb 10;17(2):e0263733.
30. World Health Organization. Quality assessment guidebook: a guide to assessing health services for adolescent clients.
31. Manual AT. Nutrition and HIV/AIDS. 2008.