Abstract
Introduction: For patients with high-risk acute myeloid leukemia (AML), defined by certain cytogenetic (CG) and molecular genetic features, hematopoietic stem cell transplantation (HSCT) remains the only curative therapy. The logistics of proceeding to transplant might necessitate consolidation chemotherapy involving high dose cytarabine (HiDAC).
Methods: We performed a retrospective cohort analysis and evaluated outcomes of high-risk AML patients treated at the Georgia Cancer Center at Augusta University, who were diagnosed and either did or did not receive HiDAC consolidation therapy between November 2003 and December 2020. For those not transplanted, we reviewed the clinical course following HiDAC consolidation therapy and identified the adverse effects, if any, that would preclude HSCT.
Results: A total of 92 high-risk AML patients were evaluated; 81.5% received induction therapy (mean age 50.8), while 18.5% did not (mean age 75.4, P<0.0001). Patients who received HiDAC had a 50% HSCT rate; infection-related complications were a major barrier. Patients who did not receive HiDAC following induction had a 45.9% HSCT rate; disease progression and performance status were the major barriers. Mean age differed significantly between non-HiDAC patients who did vs. did not receive HSCT (44.3 vs. 65.7, P=0.0002). Infections included Klebsiella, VRE, and fungal sinusitis. Median time to HSCT was 326.5 days with HiDAC vs. 127 days without.
Conclusion: Our findings suggest starting the HSCT evaluation process during the induction admission. HSCT is the sole curative option for high-risk AML patients and HiDAC consolidation may prevent a subset of these patients from receiving HSCT due to increased toxicity, immunosuppression, and infections.
Keywords
Acute myeloid leukemia, High-dose cytarabine, Intermediate-dose cytarabine, Hematopoietic stem cell transplantation, Myeloid leukemia, Leukemia
Introduction
Acute myeloid leukemia refers to a heterogeneous group of clinically aggressive hematologic neoplasms defined by arrested myeloid maturation, resulting in the accumulation of myeloid blasts in bone marrow, blood, and other tissues [1]. Cytogenetic and molecular characteristics further stratify AML into favorable, intermediate, and high-risk classifications. The high-risk category as defined by the European Leukemia Net (ELN) in 2017 includes any of the following cytogenetic changes: DEK-NUP214, KMT2A-rearrangement, BCR-ABL1, GATA2, MECOM, deletion 5q, abnormal 17p, complex or monosomal karyotype, wild type NPM1 and FLT3-ITD with high allelic ratio (>0.5), or mutated: RUNX1, ASXL1, or TP53 [1].
In fit and eligible patients, the goal of treatment is to induce complete remission (CR) or partial remission (PR) by means of high intensity induction therapy usually involving seven days of continuous cytarabine infusion along with anthracycline treatment on days one through three (7+3). To assess the response to induction and determine the remission status, bone marrow aspirate and biopsy are done 7–10 days after completion of induction therapy and again after the recovery of platelets and neutrophil counts. Next, consolidation therapy is used to further reduce the risk of disease recurrence by eradicating any residual leukemic cells that remained after induction. The goal of consolidation therapy is to prevent disease progression and improve overall survival. Consolidation therapy will involve either high intensity chemotherapy based around continuous infusions of high dose cytarabine (HiDAC) or hematopoietic stem cell transplantation (HSCT). Following consolidation, AML patients who were ineligible for HSCT, had FLT3-mutations, or had positive minimal residual disease (MRD) may receive non-myelosuppressive maintenance therapy over months to year. Standard induction therapy utilizing the 7+3 regiment results in 5-year overall survival (OS) rates of 30–45%. In patients with high-risk status, HSCT remains the only curative therapy currently available. Reported overall survival rates range from 30–70% when accounting for type of transplant, source of stem cells, the conditioning regiment used, and the stage of the disease. Despite the relative success of HSCT in high-risk AML patients, the literature reports relapse rates ranging from 30–50% [2].
The logistics involved with transplant, including patient HLA typing, donor selection, pre-transplant conditioning, and stem cell collection might necessitate consolidation chemotherapy. Over the past several decades, there have been several studies that compare the outcomes in AML patients treated with HiDAC versus intermediate dose cytarabine (IDAC). Regarding overall survival (OS), relapse-free survival (RFS), disease-free survival (DFS), and all-cause mortality, IDAC appears to be equivalent to HiDAC in patients with high-risk AML. IDAC also has a more favorable toxicity profile than HiDAC [3–7]. Other studies have demonstrated that patients treated with IDAC will have a higher likelihood of successfully receiving HSCT than those who are treated with HiDAC consolidation therapy [8]. We looked at the outcomes for high-risk AML patients evaluated and treated at our transplant institution, the Georgia Cancer Center at Augusta University, from 2003 to 2020. For those not transplanted, we considered whether the use of consolidation therapy with HiDAC was a contributing factor to lack of HSCT in this population.
Materials and Methods
We performed a retrospective cohort analysis and evaluated patient characteristics and outcomes of high-risk AML patients treated at our transplant institution, the Georgia Cancer Center at Augusta University, who were diagnosed and either did or did not receive HiDAC consolidation therapy between November 2003 and December 2020. High-risk AML was defined using the 2017 ELN guidelines and included patients whose AML was positive for one (or more) of the following genetic mutations: DEK-NUP214, KMT2A-rearrangement, BCR-ABL1, GATA2, MECOM, deletion 5q, abnormal 17p, monosomal karyotype (defined by the presence of 1 single non-X or Y monosomy in association with at least 1 additional monosomy or structural chromosome abnormality (excluding core-binding factor AML), complex cytogenetics defined as having greater than or equal to 3 CG changes), wild type NPM1 and FLT3-ITD with high allelic ratio (>0.5), or mutated: RUNX1, ASXL1, or TP53. For those not transplanted, we reviewed the clinical course following HiDAC consolidation therapy and identified the adverse effects, if any, that would preclude HSCT. We calculated descriptive statistics on age, gender, and race of the cohort, and differences in rates of infection between those who received HiDAC and those who did not. We stratified the cohort into subgroups based on induction status, HiDAC status, IDAC status, HSCT status, and reasons for not undergoing HSCT including death/infection versus other causes.
Descriptive statistics were calculated for continuous variables (mean, median, and range) and categorical variables (frequency and percentage). Comparisons between continuous variables were performed using the Student’s t-test or analysis of variance (ANOVA) when data met assumptions of normality and equal variance. Equality of variances was assessed using Bartlett’s test, and data were tested for normality using the Shapiro–Wilk test. When assumptions of normality or homogeneity of variance were not met, or when subgroup sizes were small, non-parametric methods such as the Mann–Whitney/Wilcoxon two-sample test (Kruskal–Wallis test for two groups) were used. Comparisons between categorical variables were performed using the chi-square test or Fisher’s exact test where appropriate. A p value <0.05 was considered statistically significant. Statistical analyses were conducted using Epi Info Software version 7.2.5.0 (Centers for Disease Control and Prevention, Atlanta, GA, USA).
Results
Patient demographics overall
Patient characteristics are described as seen in Table 1. A total of 92 patients diagnosed with high-risk AML were evaluated at our center from November 2003 to December 2020. The entire cohort had a median age of 60, mean age of 55.3, with a range from 14–85. The racial breakdown of the cohort is as follows: White patients made up 69.6% (n=64), black patients made up 27.2% (n=25), Hispanic patients made up 1.1% (n=1), and other racial identities made up 2.1% (n=2). Males comprised 46.7% (n=43) and females comprised 53.3% (n=49).
|
Age (Range, Median, Mean,) |
Race |
Sex |
|
Entire Cohort (n=92) Range: 14–85 Median: 60 Mean: 55.3 |
White: 64 (69.6%) Black: 25 (27.2%) Hispanic: 1 (1.1%) Other: 2 (2.1%) |
Male: 43 (46.7%) Female: 49 (53.3%) |
|
Patients who received Induction: n=75 (81.5%) Range: 14–77 Median: 55 Mean: 50.8 |
White: 52 (69.3%) Black: 20 (26.7%) Hispanic: 1 (1.3%) Other: 2 (2.7%) |
Male: 31 (41.3%) Female: 44 (58.7%) |
|
Patients who did not receive Induction: n=17 (18.5%) Range: 64–85 Median: 77 Mean: 75.4 |
White: 12 (70.5%) Black: 5 (29.5%) Hispanic: 0 (0%) Other: 0 (0%) |
Male: 12 (70.5%) Female: 5 (29.5%) |
|
No HiDAC Consolidation: n=54 (58.7%) Range: 14–85 Median: 64.5 Mean: 58.9 |
White: 38 (70.3%) Black: 14 (25.9%) Hispanic: 0 (0%) Other: 2 (3.8%) |
Male: 29 (53.7%) Female: 25 (46.3%) |
|
No HiDAC Consolidation, with HSCT: n=17 (18.5%) Range: 14–71 Median: 42 Mean: 44.3 |
White: 14 (82.4%) Black: 3 (17.6%) Hispanic: 0 (0%) Other: 0 (0%) |
Male: 7 (41.2%) Female: 10 (58.8%) |
|
No HiDAC Consolidation or HSCT: n=37 (40.2%) Range: 26–85 Median: 68 Mean: 65.7 |
White: 24 (64.9%) Black: 11 (29.7%) Hispanic: 0 (0%) Other: 2 (5.4%) |
Male: 22 (59.5%) Female: 15 (40.5%) |
|
HiDAC Consolidation: n=38 (41.3%) Range: 19–70 Median: 53 Mean: 50.1 |
White: 26 (68.4%) Black: 11 (28.9%) Hispanic: 1 (2.7%) Other: 0 (0%) |
Male: 14 (36.8%) Female: 24 (63.2%) |
|
HiDAC with HSCT: n=19 (20.7%) Range: 19–65 Median: 53 Mean: 47.0 |
White: 14 (73.7%) Black: 5 (26.3%) Hispanic: 0 (0%) Other: 0 (0%) |
Male: 6 (31.6%) Female: 13 (68.4%) |
|
HiDAC without HSCT due to Infection or Death: n=10 (10.9%) Range: 29–70 Median: 57 Mean: 54.6 |
White: 6 (60.0%) Black: 3 (30.0%) Hispanic: 1 (10.0%) Other: 0 (0%) |
Male: 2 (20.0%) Female: 8 (80.0%) |
|
HiDAC without HSCT due to Other Causes: n=9 (9.8%) Range: 24–63 Median: 56 Mean: 51.8 |
White: 6 (66.7%) Black: 3 (33.3%) Hispanic: 0 (0%) Other: 0 (0%) |
Male: 6 (66.7%) Female: 3 (33.3%) |
|
IDAC Total: n=5 (5.4%) Range: 27–69 Median: 62 Mean: 50.2 |
White: 5 Black: 0 Hispanic: 0 (0%) Other: 0 (0%) |
Male: 2 (40.0%) Female: 3 (60.0%) |
|
IDAC with HSCT: n=3 (3.3%) Range: 27–63 Median: 30 Mean: 40 |
White: 3 (100%) Black: 0 (0%) Hispanic: 0 (0%) Other: 0 (0%) |
Male: 1 (33.3%) Female: 2 (66.7%) |
|
IDAC without HSCT: n=2 (2.2%) Range: 62–69 Median: 65.5 Mean: 65.5 |
White: 2 (100%) Black: 0 (0%) Hispanic: 0 (0%) Other: 0 (0%) |
Male: 1 (50.0%) Female: 1 (50.0%) |
|
Patient characteristics table including age, race, and sex of the High-Risk AML patients treated at the Georgia Cancer Center at Augusta University between November 2003 and December 2020. Patients were stratified based on whether they received induction therapy, HiDAC consolidation therapy, or HSCT. Patients who received HiDAC but did not undergo HSCT were further stratified based on the reasons why HSCT was not performed including infection/death and other causes. Characteristics of patients who received IDAC therapy are also listed. |
||
Characteristics of patients who received induction therapy versus those who did not
Of the 92 patients in the total cohort, 81.5% (n=75) underwent induction therapy and 18.5% (n=17) did not due to prohibitive comorbidities, Eastern Cooperative Oncology Group (ECOG) performance status, being lost to follow-up, or patient preference. For patients who did receive induction therapy, the median age was 55, mean age 50.8, with a range of 14–77. The racial breakdown included 69.3% whites (n=52), 26.7% black (n=20), 1.3% Hispanic (n=1), and 2.7% other (n=2). Males comprised 41.3% of this group (n=31) and females comprised 58.7% (n=44).
For patients who did not receive induction therapy, the median age was 77, mean age 75.4, with a range of 64–85. The racial breakdown included 70.5% whites (n=12), 29.5% black (n=5), and 0% Hispanic or other. Males comprised 70.5% (n=12) of the group in females comprised 29.5% (n=5).
As noted in Table 2, when comparing the mean age for patients who received induction therapy, 50.8, to those who did not, 75.4, there is a statistically significant difference, P<0.0000. There is also a significant difference in the percentage of patients who did not get induction that are male, 70.5%, compared to the percentage of patients who did get induction that are male, 42.1%, P=0.0012.
|
|
Induction Therapy (n=75) |
No Induction Therapy (n=17) |
|
|
Age (Mean) |
50.8 |
75.4 |
P<0.0000 |
|
Race White Black Hispanic Other |
52 20 1 2 |
12 5 0 0 |
P=0.5450 |
|
Sex Male Female |
31 44 |
12 5 |
P=0.0012 (Fischer Exact) |
|
Comparison of mean age, race demographics, and sex in those who received induction therapy versus those who did not. Hispanic and “Other” races were not included in the analysis due to low sample size. P-value comparing sex breakdown is a Fischer exact value. |
|||
Characteristics of patients who did not receive HiDAC consolidation therapy and reasons for no HSCT
HiDAC consolidation therapy was not administered to 58.7% of patients (n=54). Of these 54 patients, 31.5% (n=17) were able to successfully undergo HSCT. The other 68.5% (n=37) of patients were unable to undergo HSCT. Reasons for these patients not successfully receiving HSCT included prohibitive comorbidities or ECOG performance status (n=17, 45.9%), failed induction or disease progression (n=12, 32.4%), infection or death (n=5, 13.5%), patients declining transplant (n=2, 5.4%), and being lost to follow-up (n=1, 2.7%). Table 10 describes the types of infections noted in patients who did not receive HiDAC.
Comparing patients who did not receive HiDAC consolidation therapy based on their HSCT status
The median age of patients who did not receive HiDAC consolidation therapy but were able to undergo HSCT was 42 compared to a median age of 68 in patients who did not receive HiDAC consolidation therapy and were not able to undergo HSCT. As described in Table 3, when comparing the mean age for patients who did not receive HiDAC consolidation therapy or HSCT, 65.7, to that of patients who did not receive HiDAC consolidation therapy but did undergo HSCT, 44.3, there is a statistically significant difference, P=0.0002. The racial distribution (P=0.4082) and sex differences (P=0.1997) between these 2 groups were not statistically significant.
|
|
No HiDAC, No HSCT (n=37) |
No HiDAC, with HSCT (n=17) |
|
|
Age (Mean) |
65.7 |
44.3 |
P=0.0002 |
|
Race White Black Hispanic Other |
24 11 0 2 |
14 3 0 0 |
P=0.4082 |
|
Sex Male Female |
22 15 |
7 10 |
P=0.1997 |
|
Comparison of mean age, race demographics, and sex in those who did not receive HiDAC therapy or HSCT versus those who did not receive HiDAC but did get HSCT. Hispanic and “Other” races were not included in the analysis due to low sample size. |
|||
Characteristics of patients who did receive HiDAC consolidation therapy
Patients who did receive HiDAC consolidation therapy comprised 41.3% of the total patient cohort (n=38). The median age in this group was 53, the mean age was 50.1, and the range was between 19 and 70. Racial breakdown of this group is as follows: White patients made up 68.4% (n=26), black patients made up 28.9% (n=11), and Hispanic patients made up 2.7% (n=1). Males comprised 36.8% (n=14) of this group and females comprised 63.2% (n=24). Of the patients who received HiDAC consolidation therapy, 50% (n=19) went on to HSCT and 50% (n=19) did not proceed to HSCT. For patients who did not receive HSCT, 73.6% (n=14), underwent HLA-typing, indicating consideration for transplantation.
As seen in Table 4, there was no statistically significant difference in mean age (P=0.0603), racial distribution (P=0.4054), or sex (P=0.1414) when comparing those patients who received HiDAC to those who did not.
|
HiDAC (n=38) |
No HiDAC (n=54) |
||
|
Age (Median) |
53 |
64.5 |
P=0.0603 |
|
Race White Black Hispanic Other |
26 11 1 0 |
38 14 0 2 |
P=0.4054 |
|
Sex Male Female |
14 24 |
14 24 |
P=0.1414 |
|
Comparison of median age, race demographics, and sex in those who received HiDAC therapy versus those who did not. Hispanic and “Other” races were not included in the analysis due to low sample size. |
|||
|
HiDAC |
No HiDAC |
||
|
Time in Days Range Median Mean |
97–1339 362.5 442.3 |
46–511 127 165.7 |
P=0.4020 |
|
Comparison of time from diagnosis to HSCT in days in patients treated with HiDAC consolidation therapy versus those who were not. Mann-Whitney/Wilcoxon Two-Sample Test (Kruskai-Wallis test for two groups) has a non-significant P-value of 0.4020. |
|||
Patients who underwent HiDAC consolidation therapy and HSCT had a median age of 53, mean age of 47.0, and a range of 19–65. The racial breakdown of this group contains 73.7% white patients (n=14) and 26.3% black patients (n=5). Males comprised 31.6% of this group (n=6) while females comprise 68.4% (n=13).
Characteristics of patients who received HiDAC consolidation and reasons for not undergoing HSCT
Of the 19 patients who received HiDAC consolidation therapy but were unable to undergo HSCT, 52.6% (n=10) did not proceed to transplant due to infectious complications or death and the remaining 47.3% (n=9) had noninfectious reasons for non-transplant (Table 6).
|
Reasons for Not Receiving HSCT after HiDAC |
Number of Patients |
|
Infections |
7 |
|
Death Prior to Transplant |
3 |
|
Prohibitive Comorbidities |
3 |
|
Unknown |
2 |
|
Neutropenic Fever Without Identifiable Source |
2 |
|
Drug Abuse |
1 |
|
Logistics |
1 |
|
Total |
19 |
For patients who did receive HiDAC consolidation therapy but were unable to proceed to HSCT due to infection or death, the median age was 57, mean age 54.6, with a range 29–70. The racial breakdown of this group is as follows: White patients made up to 60% (n=6), black patients made up 30% (n=3), and Hispanic patients made up 10% (n=1). Males comprised 20% (n=2) of this group and females comprised 80% (n=8).
For patients who did receive HiDAC consolidation therapy but were unable to proceed to HSCT due to noninfectious causes, the median age was 56, mean age 51.8, with a range of 24–63. White patients made up 66.7% (n=6) of this group while black patients made up 33.3% (n=3). Males comprised 66.7% (n=6) of this group while females comprised 33.3% (n=3).
Table 7 describes the types of infections noted following HiDAC consolidation. Other reasons that prevented HSCT included neutropenic fever with an unknown cause, prohibitive comorbidities, substance abuse, disease progression, and lack of follow-up, and unknown causes.
|
Types of Infections |
Number of Patients |
|
Bacteremia Klebsiella Vancomycin Resistant E. Faecalis E. Coli Proteus Group B Strep Coagulase Negative Strep |
2 2 1 1 1 1 |
|
Pneumonia Klebsiella |
1 |
|
Urinary Tract Infections Extended Spectrum Beta-Lactamase Proteus Klebsiella |
1 1 1 |
|
Fungal Sinusitis |
1 |
|
Clostridium Difficile Colitis |
3 |
|
Outcome of Patients Receiving IDAC Consolidation Therapy |
Number of Patients |
|
Able to Receive HSCT |
3 |
|
Unable to Receive HSCT |
2 |
Comparing rates of infection in patients following induction therapy
Among patients who did not proceed to HSCT, infectious complications were observed in 10 of 19 (52.6%) who received HiDAC consolidation compared to 5 of 20 (25.0%) who did not (Fisher’s exact p=0.11). This corresponded to a risk ratio of 2.11 and an odds ratio of 3.33 (95% CI, 0.86–13.0). Although not statistically significant, these findings suggest a trend toward a higher incidence of infection among patients treated with HiDAC.
|
Reasons |
Number of Patients |
|
Prohibitive Comorbidities/ECOG Performance Status |
17 |
|
Failed Induction/Disease Progression |
12 |
|
Infection/Death |
5 |
|
Patient Declined |
2 |
|
Lost to Follow-Up |
1 |
|
Total |
37 |
|
Types of Infection |
Number of Patients |
|
Septic Shock VRE Enterococcus Faecium Unspecified |
1 2 |
|
Pneumonia Burkholdeia Unspecified |
1 1 |
Characteristics of patients who received IDAC consolidation therapy
Of the 5.4% (n=5) of patients who received IDAC consolidation therapy, 60% (n=3) were able to undergo HSCT while 40% (n=2) were not. The median age of patients able to undergo HSCT after IDAC consolidation therapy was 30 with a mean of 40 compared to a median of 65.5 and a mean of 65.5 and those who received IDAC consolidation therapy but were unable to undergo HSCT.
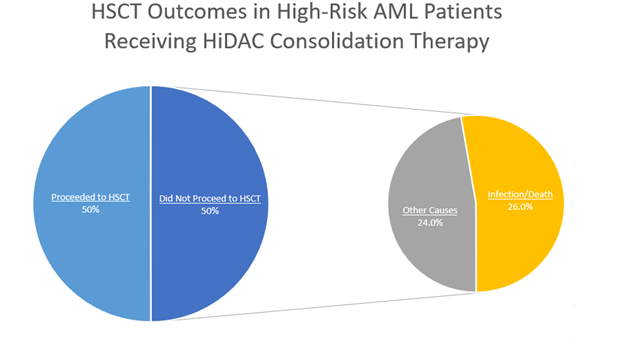
Figure 1. Graphical representation of the HSCT outcomes in 38 high-risk AML patients who received HiDAC consolidation therapy. 50% (n=19) proceeded to HSCT and 50% (n=19) did not proceed to HSCT. Of those who did not proceed to HSCT, 26% (n=10) did not do so due to infection or death and 24% (n=9) did not do so due to other causes including neutropenic fever, substance abuse, disease progression, being lost to follow up, prohibitive comorbidities, difficult logistics, or unknown causes.
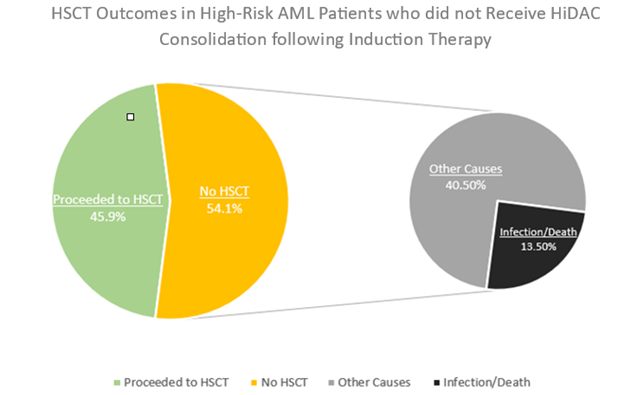
Figure 2. Graphical representation of HSCT outcomes in 37 high-risk AML patients who did not receive HiDAC consolidation therapy when removing those who did not receive induction therapy. 45.9% (n=17) proceeded to HSCT and 54.1% (n=20) did not. Of those who did not proceed to HSCT, 13.5% (n=5) did not do so due to infection or death while 40.5% (n=15) did not do so due to other causes including disease progression and patient preference.
Comparing time from diagnosis to HSCT in patients who did versus did not receive HiDAC consolidation therapy
As described in Table 5, in the 19 patients who received HiDAC consolidation therapy, the time from diagnosis to HSCT in days was as follows: Range 97–1,339, median 326.5, mean 442.3. For the 17 patients who did not receive HiDAC consolidation therapy, the time from diagnosis to HSCT and days was as follows: Range 46–511, median 127, mean 165.7. When comparing the mean time from diagnosis to HSCT in days for these 2 groups using analysis of variance (ANOVA), there initially appears to be a statistically significant difference, P value 0.00416. However, Barlett’s Test for Inequality of Population Variances yields a P value of 0.00002. Any P value less than 0.05 suggests that the variances are not homogenous between these two groups and that ANOVA is not appropriate. Mann-Whitney/Wilcoxon Two-Sample Test (Kruskai-Wallis test for two groups) has a non-significant P-value of 0.4020.
Discussion
Why we use HiDAC
The current paradigm of HiDAC use for post-remission/consolidation therapy in patients with AML is based on the landmark CALGB 8525 study from the late 1990’s which established HiDAC as the standard of care for AML post-remission therapy [9]. As evidenced by that study, for patients aged 60 or younger there was a significant difference in the rate of continued complete remission (CR) after a 5-year progression free survival (PFS) for those patients receiving HiDAC (3,000 mg/m2), Intermediate dose cytarabine (IDAC) (400 mg/m2), and Low-dose cytarabine (LDAC) (100 mg/m2) respectively (p=0.0007). It is important to note however, that for patients over the age of 60, the probability of continuous CR after 4 years was 14% or less in each of the three cytarabine groups.
HiDAC and the timing of HSCT evaluation
In the decades since this landmark trial, several studies have demonstrated that IDAC consolidation or HSCT without consolidation chemotherapy has noninferior PFS and OS compared to consolidation with HiDAC. HiDAC consolidation also has higher toxicity and rates of adverse events compared to IDAC which can prevent certain patients from proceeding to HSCT. Our data suggests that the HSCT evaluation process should start during the induction admission for patients with high-risk AML as defined by the 2017 ELN guidelines. Starting the HSCT evaluation process early helps reduce unnecessary delays between induction and consolidation with HSCT. Reducing these delays will allow providers to feel more comfortable forgoing consolidation chemotherapy to bridge the time between induction and HSCT.
HiDAC versus IDAC: Risk versus benefit
Several studies investigating the differences between the risk profile of HiDAC and IDAC have confirmed the intuitive notion that increasing doses of a cytotoxic agent will have increasing levels of adverse effects. A 2015 retrospective cohort study from Shepshelovich and colleagues revealed that the pharmacodynamics of cytarabine induced leukopenia demonstrated a monophasic decline pattern in WBC and ANC with HiDAC exhibiting a steeper rate of decline compared to IDAC [10]. Given the inferior toxicity profile, the justification for using HiDAC over IDAC comes from the idea that the benefits gained in DFS, PFS, and OS outweigh the toxicity incurred. These benefits, however, do not appear to be present in patients with high-risk cytogenetics. A 2017 meta-analysis by Wu and colleagues compared the benefit and safety of HiDAC (2-3 g/m2 twice daily), IDAC (1–2 g/m2 twice daily), and LDAC (<1 g/m2 twice daily) within 10 randomized phase III trials with 4,008 AML patients from 1994 to 2016 and found that although HiDAC did show a benefit compared to IDAC in disease free survival (HR 0.43, 95% CI 0.33–0.57, P<.00001), these benefits were biased by those with favorable cytogenetics [10]. A 1996 study by Stasi and colleagues showed that HiDAC as part of post remission therapy resulted in a substantial improvement in the cure rate in patients less than 60 years old. However, the primary benefit was derived from those with low- or intermediate-risk karyotypes and the potential benefits of an intensification of chemotherapy in elderly AML patients were by far outweighed by unacceptable toxicity [11]. When comparing clinical outcomes in AML patients receiving either HiDAC or IDAC for consolidation therapy, a consistent pattern is noted. Firstly, there does not appear to be any difference in RFS, DFS, OS, or all-cause mortality when using HiDAC. Secondly, HiDAC has higher levels of toxicity, adverse effects, and infection risk. A 2022 paper from the Thai AML registry noted that consolidation therapy in patients with intermediate to high-risk disease, who achieve their first CR should be treated with IDAC as compared to HiDAC as the former has fewer side effects [4]. Another 2022 study from Ravikumar and colleagues found that IDAC had lesser toxicity when compared to HiDAC, but that determining if efficacy was comparable would need studies with longer follow up periods and prospective studies [5]. In a 2021 study of 62 intermediate or high-risk AML patients by Tangchitpianvit et al., the authors compared HiDAC and IDAC as consolidation therapies. The one-year relapse-free survival (RFS) was 63.3% in the IDAC group and 46.9% in the HiDAC group (P=0.137), while the one-year overall survival (OS) was 93.3% and 84.4%, respectively (P=0.691). Neither difference reached statistical significance [6]. A meta-analysis performed by Magina et al. compared the efficacy of post-remission HiDAC to IDAC/LDAC. This included 9 studies ranging over a period of nearly 25 years. The findings of which were similar to the previous studies mentioned. There was no significant difference between HiDAC regimens and IDAC/LDAC in regard to RFS (HR 0.90, 95% CI 0.8-1.01) or OS (HR 0.98, 95% CI 0.87-1.09) [7]. This evidence suggests that if consolidation therapy needs to be administered in this patient population, IDAC should be used instead of HiDAC as the goal in treating patients with high-risk AML is to give them a chance to cure with HSCT. HiDAC appears to decrease the chance of achieving HSCT due to the adverse effects secondary to immunosuppression and infection. The latter was demonstrated by Hanoun and colleagues in their 2022 paper involving 642 patients who received HiDAC and 178 patients who received IDAC consolidation and found that more patients treated with IDAC received allogenic hematopoietic cell transplantation in first remission compared to those treated with HiDAC (37.6 vs. 19.8%, p<0.001) [8]. Given that there were significant differences in important patient characteristics including cytogenetic risk group, propensity score weighting was used and found that there was no significant benefit of HiDAC compared to IDAC in consolidation for patients under 65, independent of ELN risk group. A randomized controlled trial conducted by Hunault and colleagues published in June of 2025 comparing IDAC with HiDAC as postinduction therapy in patients 18 to 60 years of age with newly diagnosed AML found IDAC to be noninferior in regard to 5 year OS. The OS was estimated at 59.3% in the IDAC group and 57.5% in the HiDAC group (adjusted hazard ratio, 0.96; 95% CI, 0.80 to 1.15; noninferiority test, P=0.0042). The severity of chemotherapy-induced myelosuppression and incidence of related adverse events were lower following IDAC consolidation [14].
HiDAC versus HSCT alone
There is evidence to suggest that HSCT is preferrable to consolidative chemotherapy in this patient population due to the chance for cure and the improvements in DFS, RFS, and OS. A 1995 study by Zittoun and colleagues found that four-year DFS indicated a substantial advantage of both allo and auto-BMT (55% and 48% respectively) over chemotherapy alone (30%) [12]. Kaplan-Meier estimates from a 2016 study by Cornelissen and colleagues on patients with intermediate risk AML demonstrated that HSCT recipients had significantly better OS than patients receiving chemotherapeutic post remission therapy (P=0.001) [13]. The question of the benefit or need for consolidation chemotherapy before proceeding to transplant after achieving first complete remission (CR1) has been a subject of debate. A 2018 meta-analysis by Zhu and colleagues involving 6 studies including 1,659 patients revealed that no significant benefit was found for post-remission consolidation chemotherapy in patients who received allo-HSCT when it came to OS and relapse occurrence. The authors here suggest that patients should proceed to allo-HSCT as soon as CR1 is attained [15].
Is HiDAC consolidation preventing some high-risk AML patients from receiving HSCT?
Our data suggested that of the 38 high-risk AML patients who received HiDAC consolidation therapy, 19 of them were unable to proceed with HSCT indicating that HiDAC treatment was associated with a transplantation rate of 50%. Ten of those 19 patients did not proceed to HSCT due to infection or death. These are likely associated with the severe immunosuppression and toxicity from HiDAC. Five out of the 19 of those who were not transplanted did not have HLA-typing done at the time of first admission, preventing the possibility of early transplant following induction therapy.
Of the 54 high-risk AML patients who did not receive HiDAC consolidation therapy, 37 were unable to proceed with HiDAC treatment. On the surface, this appears to suggest that not pursuing HiDAC consolidation therapy was associated with a transplantation rate of 31.5%. However, when we removed those individuals who were either too sick to receive induction therapy or opted against induction therapy for other reasons, the transplantation rate increased to 45.9%. Importantly, the patients in this cohort who were unable to proceed to HSCT largely did so for reasons other than infection or death i.e. disease progression, failed induction, being lost to follow-up, or patient preference. The patients who did not receive HiDAC consolidation therapy but were able to proceed to HSCT were significantly younger, mean age 44.3, than those who did not receive HiDAC consolidation therapy or HSCT, mean age 65.7. When comparing this trend to those who did receive HiDAC consolidation therapy, a different relationship is noted. There was no significant difference in the mean age of those patients who received HiDAC and HSCT to those who received HiDAC and did not undergo HSCT due to infection/death or other causes. This suggests the underlying factors preventing patients who receive HiDAC from undergoing HSCT are not related to patient’s other comorbidities, EGOG performance status, or age and more likely related to the toxicity, increased immunosuppression, and infection risk of HiDAC. In our cohort, HiDAC consolidation was associated with a numerically higher rate of infectious complications compared to patients who did not receive HiDAC following induction (52.6% vs. 25.0%, p=0.11). The observed twofold increase in infection risk suggests a clinically meaningful trend and the reason statistical significance was not reached is likely due to the smaller sample size used for statistical calculations.
When comparing the time from diagnosis to HSCT in patients who received HiDAC consolidation therapy to those who did not, there was a non-significant increase in the number of days before HSCT in those who received HiDAC.
The data from our study and the literature on this topic over the past 30 years suggest starting the HSCT evaluation process during the induction admission. HSCT is the sole curative option for high-risk AML patients and HiDAC consolidation may prevent a subset of these patients from receiving HSCT due to increased toxicity, immunosuppression, and infections. Moreover, recent findings suggest IDAC consolidation is noninferior to HiDAC with increased patient tolerability. In cases where patients were able to undergo HSCT after getting HiDAC, they had to wait longer on average than those who did not receive HiDAC. Of the 5 patients in our cohort that received IDAC consolidation therapy, 3 were able to receive HSCT and 2 were unable to due to reasons other than infection/death. If consolidation therapy is deemed necessary in this patient population, IDAC should be considered over HiDAC due to its equivalent benefit and lower rates of side effects, toxicity, and infections which prevent HSCT.
Limitations
It is important to note that these results represent a retrospective analysis of high-risk AML patients at our transplant center and should be interpreted in the context of this study. This study has several limitations that should be considered when interpreting its findings. First, the study’s single-center, retrospective design may limit generalizability due to reflecting the protocols and patient characteristics unique to one institution. Second, the sample size of patients who received IDAC instead of HiDAC at our institution is exceedingly small and therefore limits any statistically significant analysis. Third, there has been an updated definition of adverse-risk AML from the ELN in 2022 which expanded the category to include AML with myelodysplasia-related gene mutations, regardless of cytogenetic findings, and removed the FLT3-ITD allelic ratio from risk stratification. This means that there were likely patients from our center who were not included in this study due to being classified as intermediate risk but who would now meet criteria for high-risk disease.
Conclusions
The data from our study and the literature on this topic over the past 30 years suggest starting the HSCT evaluation process during the induction admission. HSCT is the sole curative option for high-risk AML patients and HiDAC consolidation may prevent a subset of these patients from receiving HSCT due to increased toxicity, immunosuppression, and infections. Moreover, recent findings suggest IDAC consolidation is noninferior to HiDAC with increased patient tolerability. These results represent a retrospective analysis of high-risk AML patients at the Georgia Cancer Center at Augusta University, and prospective research should continue to be done to further elucidate these findings.
Abbreviations
AML: Acute Myeloid Leukemia; HiDAC: High-Dose Cytarabine; IDAC: Intermediate-Dose Cytarabine; HSCT: Hematopoietic Stem Cell Transplantation; MRD: Minimal Residual Disease; OS: Overall Survival; RFS: Relapse-Free Survival; CG: Cytogenetics; ECOG: Eastern Cooperative Oncology Group; E. coli: Escherichia coli; VRE: Vancomycin Resistant Enterococcus Faecalis; ANOVA: Analysis of Variance; CR: Complete Remission; PFS: Progression-Free Survival; LDAC: Low-Dose Cytarabine; ELN: European Leukemia Net
Author Contributions
Conceptualization M.S., V.K., and J.C.; Data curation: M.S., A.S., Y.R., I.P.; Formal Analysis: M.S., M.M.; Original Draft Preparation: M.S.; Review and Editing: A.S., Y.R., I.P., J.C., A.J., A.K., C.H., V.K.; Supervision: V.K.
Funding
This research received no external funding.
Data Availability Statement
The author declares that data supporting the findings of this study are available within the article
Conflicts of Interest
JC discloses relationships with Novartis, Pfizer, Sun Pharma, Syndax, Nerviano, Lilly as a consultant. He reports receiving research funding from Novartis, Sun Pharma, Ascentage, and AbbVie. He is also a current holder of stock options and has membership on the Board of Directors at Biopath Holdings. All other authors have no financial disclosure to report.
Informed Consent Statement
Informed consent for publication was waived given the retrospective nature of the study per the Institutional Review Board at Augusta University.
Institutional Board Review Statement
This retrospective study was conducted in accordance with the Declaration of Helsinki and approved by the Ethics Committee and Institutional Review Board of Augusta University. The study was granted an exemption under Category 4, as it involved secondary analysis of de-identified data with no direct interaction with human subjects.
References
2. Döhner H, Estey E, Grimwade D, Amadori S, Appelbaum FR, Büchner T, et al. Diagnosis and management of AML in adults: 2017 ELN recommendations from an international expert panel. Blood. 2017 Jan 26;129(4):424–47.
3. Shepshelovich D, Edel Y, Goldvaser H, Dujovny T, Wolach O, Raanani P. Pharmacodynamics of cytarabine induced leucopenia: a retrospective cohort study. Br J Clin Pharmacol. 2015 Apr;79(4):685–91.
4. Chanswangphuwana C, Polprasert C, Owattanapanich W, Kungwankiattichai S, Rattarittamrong E, Rattanathammethee T, et al. Comparison of Three Doses of Cytarabine Consolidation for Intermediate- and Adverse-risk Acute Myeloid Leukemia: Real World Evidence From Thai Acute Myeloid Leukemia Registry. Clin Lymphoma Myeloma Leuk. 2022 Oct;22(10):e915–e21.
5. Ravikumar D, Saju H, Choudary A, Bhattacharjee A, Dubashi B, Ganesan P, et al. Outcomes of HIDAC 18 g Versus IDAC 9 g in Consolidation Therapy of Acute Myeloid Leukemia: A Retrospective Study. Indian J Hematol Blood Transfus. 2022 Jan;38(1):31–41.
6. Tangchitpianvit K, Rattarittamrong E, Chai-Adisaksopha C, Piriyakhuntorn P, Rattanathammethee T, Hantrakool S, et al. Efficacy and safety of consolidation therapy with intermediate and high dose cytarabine in acute myeloid leukemia patients. 1998. Hematology. 2021 Dec;26(1):355–64.
7. Magina KN, Pregartner G, Zebisch A, Wölfler A, Neumeister P, Greinix HT, et al. Cytarabine dose in the consolidation treatment of AML: a systematic review and meta-analysis. Blood. 2017 Aug 17;130(7):946–8.
8. Hanoun M, Ruhnke L, Kramer M, Hanoun C, Schäfer-Eckart K, Steffen B, et al. Intensified cytarabine dose during consolidation in adult AML patients under 65 years is not associated with survival benefit: real-world data from the German SAL-AML registry. Journal of Cancer Research and Clinical Oncology. 2023 Jul;149(8):4611–21.
9. Mayer RJ, Davis RB, Schiffer CA, Berg DT, Powell BL, Shulman P, et al. Intensified Post-Remission Chemotherapy for Adults with Acute Myeloid Leukemia: An Update of CALGB 8525. In: Büchner T, Schellong G, Ritter J, Creutzig U, Hiddemann W, Wörmann B, Editors. Acute Leukemias VI: Prognostic Factors and Treatment Strategies. Berlin, Heidelberg: Springer; 1997. pp. 787–93.
10. Wu D, Duan C, Chen L, Chen S. Efficacy and safety of different doses of cytarabine in consolidation therapy for adult acute myeloid leukemia patients: a network meta-analysis. Sci Rep. 2017 Aug 25;7(1):9509.
11. Stasi R, Venditti A, Del Poeta G, Aronica G, Abruzzese E, Pisani F, et al. High-dose chemotherapy in adult acute myeloid leukemia: rationale and results. Leuk Res. 1996 Jul;20(7):535–49.
12. Zittoun RA, Mandelli F, Willemze R, de Witte T, Labar B, Resegotti L, et al. Autologous or allogeneic bone marrow transplantation compared with intensive chemotherapy in acute myelogenous leukemia. European Organization for Research and Treatment of Cancer (EORTC) and the Gruppo Italiano Malattie Ematologiche Maligne dell'Adulto (GIMEMA) Leukemia Cooperative Groups. N Engl J Med. 1995 Jan 26;332(4):217–23.
13. Cornelissen JJ, Blaise D. Hematopoietic stem cell transplantation for patients with AML in first complete remission. Blood. 2016 Jan 7;127(1):62-70.
14. Hunault M, Pautas C, Bertoli S, Dumas PY, Raffoux E, Hospital MA, et al. Intermediate-Dose Cytarabine as Postinduction AML Therapy. NEJM Evid. 2025 Jul;4(7):EVIDoa2400326.
15. Zhu Y, Gao Q, Du J, Hu J, Liu X, Zhang F. Effects of post-remission chemotherapy before allo-HSCT for acute myeloid leukemia during first complete remission: a meta-analysis. Ann Hematol. 2018 Sep;97(9):1519–26.