Clinical Image
Esophageal cancer, a highly aggressive malignancy, frequently presents with advanced-stage dysphagia, significantly impacting patient quality of life [1]. While surgical resection offers the best chance for cure in early stages, many patients are diagnosed with unresectable or metastatic disease, necessitating palliative interventions to alleviate symptoms. In such instances, endoscopic palliation, particularly with the deployment of self-expanding metal stents, plays a crucial role in restoring luminal patency and improving oral intake [2]. This case details the successful application of an esophageal self–expanding metal stent for palliation of unresectable esophageal cancer, highlighting its efficacy and safety profile in a real-world clinical scenario. This intervention is often considered first–line therapy for such management given its efficacy in rapidly restoring esophageal patency and improving patient's nutritional intake [3]. We present a case of 52-year-old male with biopsy proven case of squamous cell carcinoma of esophagus with history dysphagia and recurrent cough especially after food intake. The patient was evaluated thoroughly and esophagogastroduodenoscopy was done which was suggestive of ulcerated growth with narrowing from 20 cm to 27 cm from incisors, and a small circular defect was seen at around 24 cm suggestive of tracheo–esophageal fistula (Figure 1).
Due to unrespectable disease, the patient was planned for esophageal self-expanding metal stent placement (SEMS). Partially covered Esophageal SEMS of size 12 cm was placed starting from 19 to 31 cm, to sufficiently cover the trachea-esophageal fistula as well as the growth containing segment of esophagus (Figures 2 and 3). Post SEMS placement, the patient had relief in symptoms like dysphagia and recurrent cough.
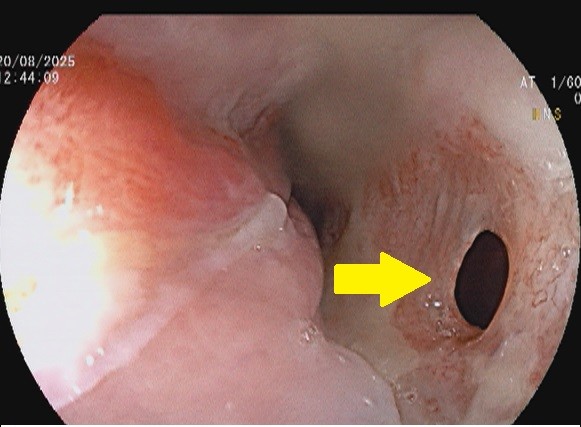
Figure 1. Endoscopic image showing ulcerated growth causing narrowing of esophageal lumen along with a small circular defect suggestive of tracheo-esophageal fistula (yellow solid arrow).

Figure 2. Endoscopic image post esophageal self expanding metal stent (E-SEMS) placement.
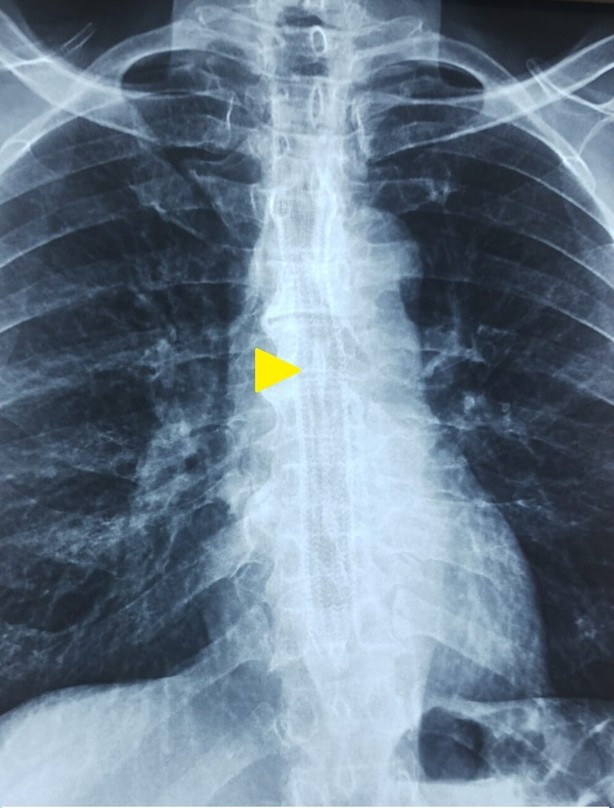
Figure 3. X-ray image showing esophageal self expanding metal stent (E-SEMS) in situ (yellow arrow head).
Declarations
Ethical approval
Not applicable.
Consent to participate
Patient provided informed consent to participate.
Human ethics
Not applicable.
Consent for publication
Patient provided informed consent to publish the included information.
Availability of supporting data
Not applicable.
Competing interests
None.
Funding
None.
Authors’ contributions
All author contributed equally in the preparation of manuscript.
Acknowledgements
None.
References
2. Javaid S, Frasier K, Baur V. Comparafive analysis of enteral and parenteral nutrifion impact on outcomes in esophageal cancer pafients: a paradigm for nutrifional opfimizafion in oncology. J Oncology. 2024;4(1):1124.
3. Jung CFM, Müller-Dornieden A, Gaedcke J, Kunsch S, Gromski MA, Biggemann L, et al. Impact of Endoscopic Vacuum Therapy with Low Negative Pressure for Esophageal Perforations and Postoperative Anastomotic Esophageal Leaks. Digestion. 2021;102(3):469–479.