Abstract
Pulmonary complications after electrical injury are uncommon and are most often interpreted as parenchymal forms of lung damage, including non-cardiogenic pulmonary edema, diffuse alveolar hemorrhage, or focal thermal injury. However, recent case-based observations suggest that this may not be the only pattern. In some patients, severe hypoxemia and pulmonary hypertension appear to be greater than expected from the extent of radiographic abnormalities. In a recently published case of high-voltage electrocution, profound refractory hypoxemia (PaO2/FiO2 68), markedly elevated pulmonary artery pressures (68/39 mmHg), preserved right ventricular function, and only mild posterior ground-glass opacities on CT pulmonary angiography raised the possibility of a vascular-dominant form of acute lung injury. In that setting, physiological severity was difficult to explain by alveolar flooding alone.
This commentary proposes a clinical and pathophysiological framework for understanding this pulmonary vascular phenotype after electrical trauma. Electrical current may contribute to lung injury through several converging mechanisms, including electroporation-related membrane disruption, thermal microvascular damage, endothelial barrier dysfunction, maladaptive pulmonary vasoconstriction, impaired hypoxic vasoregulation, and microthrombotic perfusion defects that may remain below the resolution of routine CT imaging. Recognizing this pattern could be clinically relevant. It may help clinicians avoid anchoring on incidental distal subsegmental pulmonary embolism, encourage early echocardiographic and hemodynamic assessment, support carefully monitored trials of inhaled pulmonary vasodilators as physiologic probes, and prompt timely referral for extracorporeal support when hypoxemia remains refractory despite optimized conventional care. Future studies should clarify how often this phenotype occurs, identify biomarkers of endothelial and microvascular injury, and determine which patients may benefit from vascular-targeted supportive strategies.
Keywords
Electrocution, Electrical injury, Acute lung injury, Pulmonary hypertension, Endothelial dysfunction, Ventilation–perfusion mismatch, Microthrombosis, Refractory hypoxemia, VV-ECMO
Introduction
Electrical injuries, particularly high-voltage exposures, are relatively infrequent but can lead to severe multisystem morbidity and death. Although cardiovascular and musculoskeletal complications tend to receive most attention, pulmonary involvement is increasingly recognized and may be underdiagnosed. Reported pulmonary manifestations include non-cardiogenic pulmonary edema, diffuse alveolar hemorrhage, focal parenchymal “burn” injury, and refractory hypoxemia with limited imaging abnormalities [1–7]. Despite these observations, a unifying explanation for the spectrum of pulmonary injury remains uncertain, and most clinical interpretations continue to rely primarily on an alveolar or parenchymal model.
Our recently published case illustrated a different possibility: severe refractory hypoxemia with marked pulmonary hypertension and preserved right ventricular function, despite only mild posterior ground-glass changes on CT [1]. A similar mismatch between gas-exchange impairment and the extent of parenchymal abnormalities has been described in other reports of pulmonary electrical injury, supporting the possibility of an underlying vascular or endothelial mechanism [2–4]. Building on these observations, this commentary proposes a clinical and mechanistic framework for recognizing a pulmonary vascular phenotype of acute lung injury after electrical trauma, integrating available case-based evidence with established concepts of electroporation, pulmonary vasoregulation, endothelial injury, and microvascular thrombosis.
Mechanistic Framework: Why Electrical Injury Can Be Vascular-Dominant
Electroporation and endothelial barrier dysfunction
Electroporation, also known as electropermeabilization, describes an increase in cell membrane permeability after exposure to high-voltage, short-duration electric fields [8]. At lower intensities, this process may be reversible, however, when the exposure is intense, prolonged, or unevenly distributed across tissues, it can become injurious. This mechanism is particularly relevant for the pulmonary microvasculature, because experimental and translational studies have shown that electroporation can disrupt the endothelial cytoskeleton, alter monolayer integrity, and increase vascular permeability [9,10]. In vivo observations also suggest that electroporation may produce acute vascular constriction followed by increased permeability through disruption of endothelial cell-to-cell junctions [10]. Taken together, these effects provide a plausible biological basis for an endotheliopathy-first pattern of pulmonary injury after electrocution.
Acute pulmonary vasoconstriction and loss of adaptive hypoxic vasoregulation
Hypoxic pulmonary vasoconstriction (HPV) is a central adaptive mechanism in pulmonary physiology. By diverting blood flow away from poorly ventilated lung units, HPV helps preserve ventilation–perfusion matching. When this response is disrupted, shunt physiology may be amplified and hypoxemia may worsen, even if the alveolar architecture is relatively preserved [11–13]. After electrical injury, endothelial damage could contribute to maladaptive vasoconstriction in well-ventilated regions, loss of targeted HPV responses, or both. The resulting effect would be a more global pattern of V/Q maldistribution and functional shunt. This mechanism is consistent with reports in which severe hypoxemia occurs despite limited consolidative changes on imaging [1–4].
Microthrombosis and perfusion defects
Endothelial injury also creates a procoagulant microenvironment. In Acute Respiratory Distress Syndrome (ARDS), endotheliopathy is increasingly recognized as a central pathobiological pathway, and microvascular thrombosis can contribute to dead-space ventilation and V/Q mismatch [14,15]. In addition, ARDS is now understood as a heterogeneous syndrome that includes biologically and clinically distinct subphenotypes with different inflammatory and vascular profiles [16]. This supports the possibility that vascular-dominant forms of lung injury may occur across different etiologies. In electrical trauma, a similar mechanism is biologically plausible: microthrombotic perfusion defects below the spatial resolution of routine CT imaging could worsen oxygenation and increase pulmonary vascular pressures without producing a visible large-vessel thrombus burden. This hypothesis is consistent with the hemodynamic profile observed in our case, where marked pulmonary hypertension, high/normal cardiac index, and only mildly elevated calculated pulmonary vascular resistance suggested a predominantly distributive or vasoregulatory disturbance with microvascular involvement, rather than a single obstructive lesion [1].
Figure 1 illustrates a proposed vascular-dominant pathway of acute lung injury after electrical trauma. Electrical current may trigger cell membrane electroporation and endothelial injury, with subsequent impairment of barrier function, maladaptive pulmonary vasoconstriction, microthrombotic perfusion defects, ventilation–perfusion mismatch, and severe refractory hypoxemia. The model is based on experimental and translational evidence on electroporation and endothelial permeability [8–10], pulmonary hypoxic vasoregulation [11–13], and endothelial/microvascular dysfunction in ARDS [14–16].
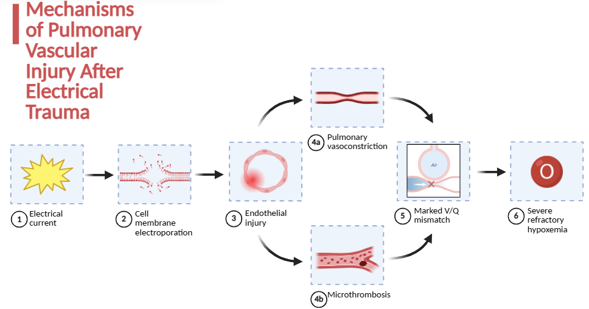
Figure 1. Mechanisms of pulmonary vascular injury after electrical trauma. Created with BioRender.com.
The Pulmonary Vascular Phenotype: Clinical and Hemodynamic Signature
A vascular-dominant pattern after electrical trauma may be suspected when several clinical and hemodynamic clues converge. This cluster should be understood as a proposed bedside framework, not as a validated diagnostic classification. It is derived from the index case, related reports of pulmonary electrical injury, and broader concepts of vascular and endothelial dysfunction in ARDS [1–7,14–16].
Severe hypoxemia disproportionate to imaging
CT may show only mild ground-glass opacities or limited dependent changes, while gas exchange deteriorates to the range of severe ARDS, with PaO2/FiO2 ≤100 [1,5–7,14].
Early or disproportionate pulmonary hypertension
Marked elevation of pulmonary artery pressures may occur with preserved or only mildly impaired right ventricular function. This pattern suggests acute pulmonary vasoregulatory failure rather than progressive parenchymal flooding alone [1].
Minimal evidence of cardiogenic pulmonary edema
Echocardiography may show preserved left ventricular systolic function. When available, invasive hemodynamic assessment can help interpret filling pressures, including wedge pressure, although these values should be considered cautiously in critical illness and under conditions of high intrathoracic pressure [1].
Coexisting triggers that may complicate attribution
Post-cardiac arrest syndrome may contribute to acute lung injury and systemic inflammation, making causality difficult to establish in individual cases [17,18]. In this setting, electrical injury may act as the primary driver, an amplifier, or one component of a multifactorial lung injury process.
Table 1 summarizes a practical bedside comparison between typical alveolar-dominant ARDS and the proposed vascular-dominant phenotype after electrical trauma. This comparison is intended as a conceptual framework rather than a validated diagnostic classification. The synthesis is based on case-based reports of pulmonary injury after electrical trauma [1–7], established principles of pulmonary vasoregulation [11–13], endothelial and microvascular mechanisms in ARDS [14–16], current supportive-care literature for ARDS [23–27], and guidance on extracorporeal support [29,33]. The table is intended as an interpretive clinical framework, not as a validated diagnostic classification.
|
Feature |
Alveolar-dominant ARDS (typical) |
Vascular-dominant electrical phenotype (proposed) |
|
Imaging |
Diffuse bilateral opacities/consolidations |
Mild/limited ground-glass, imaging underestimates severity |
|
Compliance |
Often reduced |
May be relatively preserved early |
|
Primary physiologic problem |
Alveolar flooding, low V/Q |
V/Q maldistribution from vasoregulation failure, functional shunt |
|
Pulmonary pressures |
Variable, RV strain possible |
Pulmonary hypertension may be prominent early |
|
Response to PEEP |
Often improves oxygenation |
Variable, may be limited if perfusion mismatch dominates |
|
Key diagnostic tools |
CT/CXR + ARDS criteria |
Add early echo ± pulmonary artery catheterization |
|
Adjunctive therapies |
Prone positioning, consider ECMO |
Consider inhaled vasodilator trial as physiologic probe, early ECMO triage |
Diagnostic Pitfalls: The Subsegmental PE Problem
CT pulmonary angiography may identify very distal subsegmental pulmonary embolism (SSPE) in critically ill patients. When found in isolation, SSPE often has limited hemodynamic relevance, and current guidelines and expert reviews recommend interpreting it in clinical context, including symptoms, DVT status, recurrence risk, and bleeding risk. In carefully selected low-risk patients, structured surveillance may also be a reasonable alternative to immediate anticoagulation [19–22].
In the proposed electrical vascular phenotype, the main diagnostic pitfall is anchoring: attributing profound hypoxemia to an incidental distal SSPE despite preserved right ventricular function and limited parenchymal abnormalities. Our case illustrates why a physiology-first interpretation is important. When severe hypoxemia and pulmonary hypertension coexist with a modest imaging burden, clinicians should consider diffuse pulmonary microvascular dysfunction rather than assuming that a single distal clot explains the full clinical picture [1].
Therapeutic Implications: Treating Physiology When Imaging Lags
Conventional ARDS measures remain foundational
Regardless of the suspected phenotype, conventional ARDS management remains the starting point. Lung-protective ventilation, using approximately 6 mL/kg of predicted body weight and avoiding injurious airway pressures, remains a core standard of care [23]. In patients with severe hypoxemia, prone positioning should also be considered early, contemporary ARDS guidelines support this strategy, and the PROSEVA trial showed a mortality benefit with early, prolonged prone sessions in severe ARDS [24,25].
Inhaled pulmonary vasodilators as a diagnostic–therapeutic probe
Inhaled pulmonary vasodilators can transiently improve oxygenation in ARDS by redirecting pulmonary blood flow toward better ventilated lung regions, thereby improving ventilation–perfusion matching. However, this physiologic response has not consistently translated into improved survival or other patient-centered outcomes, and inhaled nitric oxide has been associated with potential adverse effects. For that reason, these agents should be viewed as rescue or bridging interventions in selected patients, rather than as disease-modifying therapy. In the vascular-dominant pattern after electrical injury, where pulmonary vasoconstriction and V/Q maldistribution may play a central role, a time-limited trial of inhaled nitric oxide or inhaled prostacyclin could be considered as a bedside physiologic probe. Any response should be assessed objectively, using changes in PaO2/FiO2, pulmonary pressures when available, and dead-space surrogates. This framing keeps the proposal clinically useful while avoiding an unsupported claim of therapeutic efficacy [26–28].
Early ECMO triage when refractory hypoxemia persists
When severe hypoxemia persists despite optimized conventional management, early referral to a center with extracorporeal capability should be considered. In practice, this scenario is often framed around persistent PaO2/FiO2 ≤80–100 despite high FiO2 and appropriate adjunctive measures. The (Extracorporeal Life Support Organization) ELSO guideline on (Venovenous Extracorporeal Membrane Oxygenation) VV-ECMO for adult respiratory failure, together with expert recommendations on ECMO program organization, provides practical guidance for referral, patient selection, initiation, and management [29,33]. In the proposed phenotype, timing is particularly important: imaging abnormalities may remain modest while gas exchange and pulmonary vascular physiology continue to deteriorate. Delayed escalation may increase the risk of multiorgan failure and narrow the window for safe transfer.
Future Directions
Three research priorities follow from the proposed vascular phenotype concept:
Epidemiology and phenotype definition
Because pulmonary involvement after high-voltage electrical injury is rare and clinically heterogeneous, prospective registries may be the most realistic first step beyond isolated case reports. These registries should capture serial gas-exchange data, ventilatory mechanics, echocardiographic findings, candidate endothelial and microthrombotic biomarkers, and clinical outcomes. A structured approach of this kind would help estimate the incidence of this phenotype, describe its clinical course over time, and determine whether reproducible clinical and biological criteria can be established [7,14–16,30–32].
Biomarkers of endothelial injury and microthrombosis
The ARDS literature supports the relevance of endothelial injury markers as both prognostic and mechanistic signals [14,15]. In electrical trauma–associated lung injury, targeted biomarker panels could help identify patients in whom vascular and microvascular mechanisms are more likely to dominate the clinical picture.
Treatment-responsive subgroups
Given the rarity of pulmonary vascular injury after electrical trauma, conventional randomized trials are unlikely to be feasible in the near future. A more practical strategy would be to develop structured observational studies that look for clinically meaningful patterns of treatment response. Future studies could evaluate whether early hemodynamic assessment, objective improvement after inhaled pulmonary vasodilators, or timely referral for VV-ECMO is associated with better oxygenation trajectories, shorter duration of mechanical ventilation, or improved survival. Rather than assuming benefit, this approach would help define whether a reproducible subgroup of patients responds to vascular-targeted supportive care [16,26,33].
Figure 2 presents a clinical framework for recognizing a proposed vascular-dominant phenotype of acute lung injury after electrical trauma. It highlights severe hypoxemia out of proportion to imaging findings, early assessment of pulmonary pressures and ventricular function, contextual interpretation of distal subsegmental pulmonary embolism, time-limited use of inhaled pulmonary vasodilators as physiologic probes, and early referral for extracorporeal support when hypoxemia remains refractory despite optimized conventional management. The framework is informed by case-based reports of pulmonary injury after electrical trauma [1–7], post-cardiac arrest and pulmonary embolism literature [17–22], ARDS supportive-care recommendations [23–27], and extracorporeal support guidance [29,33].
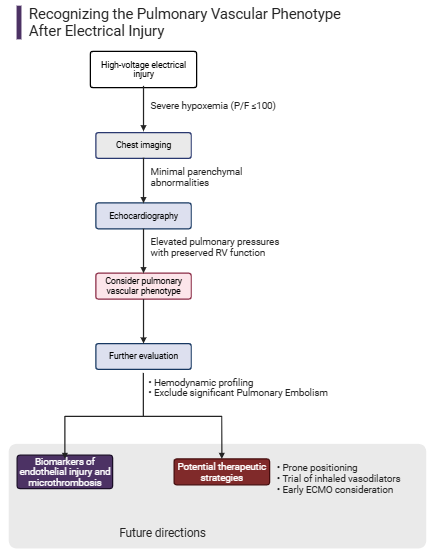
Figure 2. Recognizing the pulmonary vascular phenotype after electrical injury. Created with BioRender.com.
Conclusion
Electrical trauma may, in selected cases, be associated with a pulmonary vascular pattern of acute lung injury. In this proposed phenotype, electroporation-related endothelial injury, maladaptive pulmonary vasoconstriction, and microvascular thrombosis could contribute to severe V/Q maldistribution and pulmonary hypertension, even when parenchymal abnormalities on imaging are limited. Recognizing this possibility is clinically relevant because it encourages clinicians to look beyond a purely alveolar model of injury, avoid premature anchoring on incidental distal SSPE, and consider early echocardiographic and hemodynamic assessment when the severity of hypoxemia is not explained by imaging alone. From a therapeutic standpoint, this framework does not replace conventional ARDS management, but it may help guide escalation when hypoxemia remains refractory. In carefully selected patients, time-limited trials of inhaled pulmonary vasodilators may serve as physiologic probes, and early referral for extracorporeal support should be considered when conventional strategies fail. The current evidence remains limited and largely case-based. Nevertheless, the recurring mismatch between physiology and imaging, together with biologically plausible vascular mechanisms, supports broader clinical awareness and more systematic study of this potential phenotype.
References
2. Koumbourlis AC. Electrical injuries. Crit Care Med. 2002 Nov;30(11 Suppl):S424–30.
3. Waldmann V, Narayanan K, Combes N, Jost D, Jouven X, Marijon E. Electrical cardiac injuries: current concepts and management. Eur Heart J. 2018 Apr 21;39(16):1459–65.
4. Fish RM. Electric injury, part III: cardiac monitoring indications, the pregnant patient, and lightning. J Emerg Med. 2000 Feb; 18(2):181–7.
5. Masanès MJ, Gourbière E, Prudent J, Lioret N, Febvre M, Prévot S, et al. A high voltage electrical burn of lung parenchyma. Burns. 2000 Nov; 26(7):659–63.
6. Singh DK, Pandey G, Rizvi SHM, Singh PK. Isolated pulmonary hemorrhage after electric shock: a rare phenomenon. Monaldi Arch Chest Dis. 2023 Jul 28; 94(1).
7. Vu-Hoai N, Dang-Vu T, Lam-Quoc D, Duong-Minh N, Tran-Ngoc TH, Tran-Ngoc N, et al. Isolated pulmonary injury following electric shock: a case report and literature review. Ann Med Surg (Lond). 2024 Dec 19;87(3):1670–7.
8. Weaver JC. Electroporation: a general phenomenon for manipulating cells and tissues. J Cell Biochem. 1993 Apr;51(4):426–35.
9. Rubinsky B. Irreversible electroporation in medicine. Technol Cancer Res Treat. 2007 Aug;6(4):255-60.
10. Yarmush ML, Golberg A, Serša G, Kotnik T, Miklavčič D. Electroporation-based technologies for medicine: principles, applications, and challenges. Annu Rev Biomed Eng. 2014 Jul 11; 16:295–320.
11. Sylvester JT, Shimoda LA, Aaronson PI, Ward JP. Hypoxic pulmonary vasoconstriction. Physiol Rev. 2012 Jan; 92(1):367–520.
12. Dunham-Snary KJ, Wu D, Sykes EA, Thakrar A, Parlow LRG, Mewburn JD, et al. Hypoxic Pulmonary Vasoconstriction: From Molecular Mechanisms to Medicine. Chest. 2017 Jan;151(1):181–92.
13. Swenson ER. Hypoxic pulmonary vasoconstriction. High Alt Med Biol. 2013 Jun;14(2):101–10.
14. Matthay MA, Zemans RL, Zimmerman GA, Arabi YM, Beitler JR, Mercat A et al. Acute respiratory distress syndrome. Nat Rev Dis Primers. 2019 Mar 14;5(1):18.
15. Ackermann M, Verleden SE, Kuehnel M, Haverich A, Welte T, Laenger F, et al. Pulmonary Vascular Endothelialitis, Thrombosis, and Angiogenesis in Covid-19. N Engl J Med. 2020 Jul 9;383(2):120–8.
16. Sinha P, Calfee CS, Cherian S, Brealey D, Cutler S, King C, et al. Prevalence of phenotypes of acute respiratory distress syndrome in critically ill patients with COVID-19: a prospective observational study. Lancet Respir Med. 2020 Dec; 8(12):1209–18.
17. Nolan JP, Sandroni C, Böttiger BW, Cariou A, Cronberg T, Friberg H, et al. European Resuscitation Council and European Society of Intensive Care Medicine Guidelines 2021: Post-resuscitation care. Resuscitation. 2021 Apr;161:220–69.
18. Sandroni C, D'Arrigo S, Cacciola S, Hoedemaekers CWE, Kamps MJA, Oddo M, et al. Prediction of poor neurological outcome in comatose survivors of cardiac arrest: a systematic review. Intensive Care Med. 2020 Oct;46(10):1803–51.
19. Le Gal G, Righini M, Roy PM, et al. Prediction of pulmonary embolism in the emergency department. Ann Intern Med. 2006 ,144(3):165–71.
20. Leung AN, Bull TM, Jaeschke R, et al. American Thoracic Society clinical practice guideline: Evaluation of suspected pulmonary embolism. Am J Respir Crit Care Med. 2011 ,184(10):1200–8.
21. Kearon C, Akl EA, Ornelas J, Blaivas A, Jimenez D, Bounameaux H, et al. Antithrombotic Therapy for VTE Disease: CHEST Guideline and Expert Panel Report. Chest. 2016 Feb;149(2):315–52.
22. Yoo HH, Queluz TH, El Dib R. Anticoagulant treatment for subsegmental pulmonary embolism. Cochrane Database Syst Rev. 2016 Jan 12;(1):CD010222.
23. Fan E, Del Sorbo L, Goligher EC, Hodgson CL, Munshi L, Walkey AJ, et al. American Thoracic Society, European Society of Intensive Care Medicine, and Society of Critical Care Medicine. An Official American Thoracic Society/European Society of Intensive Care Medicine/Society of Critical Care Medicine Clinical Practice Guideline: Mechanical Ventilation in Adult Patients with Acute Respiratory Distress Syndrome. Am J Respir Crit Care Med. 2017 May 1;195(9):1253–63.
24. Guérin C, Reignier J, Richard JC, Beuret P, Gacouin A, Boulain T, et al. PROSEVA Study Group. Prone positioning in severe acute respiratory distress syndrome. N Engl J Med. 2013 Jun 6;368(23):2159–68.
25. Papazian L, Aubron C, Brochard L, Chiche JD, Combes A, Dreyfuss D,et al. Formal guidelines: management of acute respiratory distress syndrome. Ann Intensive Care. 2019 Jun 13;9(1):69.
26. Gebistorf F, Karam O, Wetterslev J, Afshari A. Inhaled nitric oxide for acute respiratory distress syndrome (ARDS) in children and adults. Cochrane Database Syst Rev. 2016 Jun 27; 2016(6):CD002787.
27. Torbic H, Saini A, Harnegie MP, Sadana D, Duggal A. Inhaled Prostacyclins for Acute Respiratory Distress Syndrome: A Systematic Review and Meta-Analysis. Crit Care Explor. 2023 Jun 8;5(6):e0931.
28. Ferguson ND. Inhaled nitric oxide for acute respiratory distress syndrome. BMJ. 2007 Apr 14;334(7597):757–8.
29. Combes A, Brodie D, Bartlett R, Brochard L, Brower R, Conrad S, et al. International ECMO Network (ECMONet). Position paper for the organization of extracorporeal membrane oxygenation programs for acute respiratory failure in adult patients. Am J Respir Crit Care Med. 2014 Sep 1;190(5):488–96.
30. Goyal D, Jagne N, Dhiman A, Patil V, Rattan A. High voltage electrical injuries: outcomes & 1-year follow-up from a level 1 trauma centre. Int J Burns Trauma. 2021 Apr 15;11(2):115–22.
31. Reilly JP, Calfee CS, Christie JD. Acute Respiratory Distress Syndrome Phenotypes. Semin Respir Crit Care Med. 2019 Feb;40(1):19–30.
32. Vassiliou AG, Kotanidou A, Dimopoulou I, Orfanos SE. Endothelial Damage in Acute Respiratory Distress Syndrome. Int J Mol Sci. 2020 Nov 20;21(22):8793.
33. Tonna JE, Abrams D, Brodie D, Greenwood JC, Rubio Mateo-Sidron JA, Usman A, et al. Management of Adult Patients Supported with Venovenous Extracorporeal Membrane Oxygenation (VV ECMO): Guideline from the Extracorporeal Life Support Organization (ELSO). ASAIO J. 2021 Jun 1;67(6):601–10.