Abstract
Background: Thoracic spine thrust (TST) manipulation has been investigated for its mechanical and neurophysiological effect. However, changes in plantar pressure distribution still does not directly relate to TST manipulation in scientific literature.
Objective: To compare differences in plantar pressure distribution post Thoracic spine thrust (TST) manipulation between men and women practitioners of resistance exercise.
Methods: Thirty participants were selected (15 men and 15 women) that complied with the eligibility criteria. All participants were practitioners of resistance exercise and underwent evaluations in the baropodometry platform pre- and post- TST manipulation. All tests were performed in a single session to assess the plantar pressure and surface area of both feet, maximum peak pressure, and mean pressure.
Results: The plantar pressure distribution showed significant difference (p<.001) in plantar surface area (cm2) between men vs. women group pre- and post-TST manipulation. However, women showed significant increase and decrease in right forefoot (p<.01) and hindfoot (p<.03) post-manual therapy, respectively.
Conclusion: These finding confirm that TST manipulation improved the plantar surface area and distribution of the plantar surface area in women. Thus, it appears that TST manipulation acutely assists in the stability of women.
Keywords
Thoracic spine thrust manipulation, Baropometry platform, Balance, Muscle and joint injuries
Introduction
The manual therapy is a therapeutic intervention method involving the skilled application of passive movement to the body from the use of hands with a therapeutic intent [1,2]. Thus, manual therapy techniques are intended to mobilize skin, fascia, neural, vascular, lymphatic, myogenic and arthrogenic tissue [3]. Manual therapy approaches and techniques include massage, joint mobilization/manipulation, myofascial release, nerve manipulation, strain/counterstrain, and acupressure [1-3]. Likewise, this technique aims to optimize tissue extensibility, increase range of motion, mobilize soft tissues and joints, promote relaxation, improve muscle function, modulate pain, reduce soft tissue swelling, inflammation or movement restriction [3,4].
Thrust joint manipulation and mobilization are commonly used to reduce pain, eliminate impairment, and improve function [1,2]. Specifically, thoracic spine thrust (TST) manipulation has been investigated for its mechanical and neurophysiological effect [3-6]. TST manipulation is used for correction of the thoracic vertebrae through different techniques, such as lift off (upper thoracic and lower thoracic spine), thoracic rotation manipulation and the crossed pisiform technique [3,5,7].
TST manipulation requires the application of a thrust with a high-speed and low-amplitude movement at the beginning of exhalation that eliminates tissue resistance, and the vertebra is induced to its articular limit in the opposite direction to restriction [5]. Thus, suggest that TST manipulation has an impact on the integration and processing of somatosensory information from the limbs [5,6]. It appears that this activity cortical somatosensory evoked potentials represent the arrival of the afferent signals at the primary somatosensory cortex and sensorimotor integration, respectively [5,6]. In addition, changes were observed in the motor control changes following spinal manipulation [8]. However, changes in plantar pressure distribution still do not directly relate to TST manipulation in scientific literature. Consequently, the absence of data supports the need for additional studies in this area. Hence, the purpose of this investigation was to compare differences in plantar pressure distribution post-TST manipulation between male and female practitioners of resistance exercise.
Methods
Study design
This is a randomized comparative study. The sample size was determined by including all participants that complied with the eligibility criteria. All participants (male and female) were practitioners of resistance exercise and underwent two tests in the baropodometry platform before and after thoracic spine thrust (TST) manipulation in static conditions without footwear (Figure 1). All tests were performed in a single assessment session to assess plantar surface area of both feet (cm2), plantar pressure distribution between hindfoot and forefoot (%), maximum peak pressure, and mean pressure. All assessments were taken in a temperature-controlled environment (temperature 21°C, 65% relative humidity) by a Hygro-Thermometer with Humidity Alert (Extech Instruments, Massachusetts, EUA). All assessments occurred between 2:00 and 4:00 P.M.
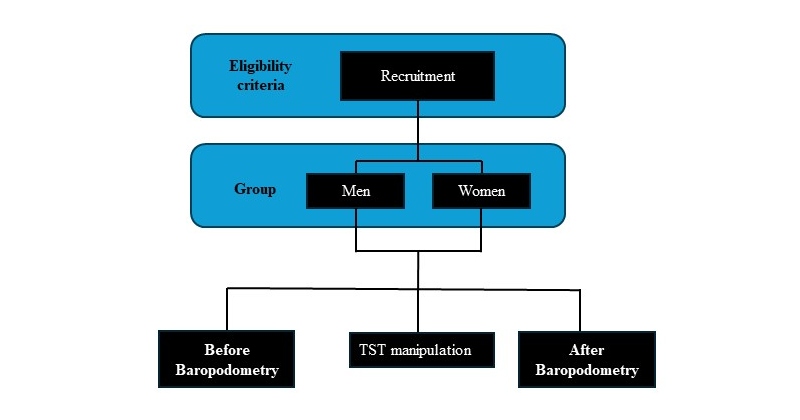
Figure 1: Study design: division of the groups.
Participants
This study included 30 healthy individuals separated into two groups: men (age: 32.6 ± 8.7 years; height: 180.2 ± 5.5 cm; body mass: 83.1 ± 5.8 kg; body fat: 15.2 ± 3.5%; n= 15) and women (age: 35.5 ± 8.1 years; height: 165.3 ± 4.4 cm; body mass: 63.9 ± 9.2 Kg; body fat: 19.5 ± 4.2%, n = 15). The participants’ training frequency was 5.1 ± 0.7 days/week-1 with a mean duration for each session training of 65 min-1 using resistance-training programs. Subjects with at least one year of resistance exercise experience were included to participate in the current study. All participants performed a routine of resistance training programs that engaged the whole body with resistance bands, free-weights, dumbbells and medicine balls. The participants were eligible if they were not smokers for the previous 3 months or more; had no cardiovascular or metabolic diseases, systemic hypertension (140/90 mm Hg or use of antihypertensive medication), recent musculoskeletal injury and surgery (in the last 6 months), or pain in any region of the body; and had not used anabolic steroids, drugs or any medication with the potential to impact physical performance (self-reported). This study was approved by the Ethical Committee for Human Experiments of the Augusto Motta University Center, Rio de Janeiro, Brazil (CAAE: 31692920.5.0000.5235). The present study was conducted at the Rehabilitation Science Center, Augusto Motta University Center, Rio de Janeiro, Brazil. All participants were informed of the experimental procedures and gave written informed consent prior to participation. No clinical problems occurred during the study.
Anthropometric measurements
Body composition was measured following an 8-h overnight fast by bioelectrical impedance analysis using a device with built-in hand and foot electrodes (BIO 720, Avanutri, Rio de Janeiro, Brasil). The participants wore their normal indoor clothing and were instructed to stand barefoot in an upright position with both feet on separate electrodes on the device’s surface and with their arms abducted and both hands gripping two separate electrodes on each handle of the device. All biometric measurements were carried out in an air-conditioned room (21°C). No clinical problems occurred during the study.
Baropodometry assessment
The baropodometry platform consisted of a support with a 655 mm long and 534 mm wide (BaroScan®, Londrina, Brazil). The board contained 4,096 platinum electronic sensors covered by an alveolar rubber captor that gives pressure information from each foot through a USB cable to the computer for appropriate software (BaroSys). The sampling rate was set at 100 Hz for static assessment. Before assessments, all individuals remained in a standing, bipedal position with their arms pending along the body over the platform with their eyes open mirrored to a fixed point on the wall of the examination room. During static conditions, the subjects stood on the platform in an orthostatic position for 5-s (Figure 2). The following parameters were considered in static condition: plantar surface area of both feet (cm2), plantar pressure distribution between hindfoot and forefoot (%), maximum peak pressure, and mean pressure. The forefoot was assumed to be the foot part anterior to the gravity center and the hindfoot as the part posterior to the center of gravity registered on the device.
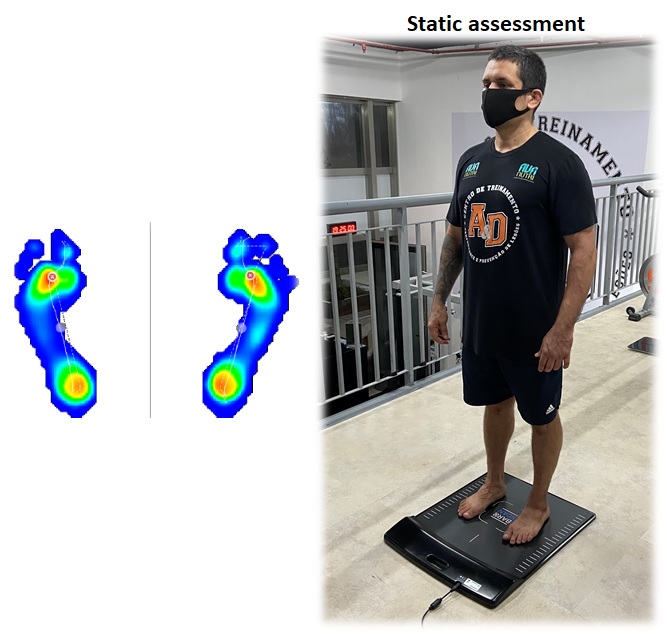
Figure 2: Positioning for performing static assessments on the stability platform.
Thoracic spine thrust manipulation
The thoracic spine thrust (TST) manipulation consisted of a high-velocity, low-amplitude anterior-to-posterior with range force applied through the elbows to the upper thoracic spine on the T3 vertebra spine in cervicothoracic flexion, with the patient positioned supine (Figure 3). The physiotherapist positioned a stabilizing hand immediately caudal to the T3 vertebra, pushing the volunteer’s arms downward to generate flexion of the upper thoracic spine. Then, the volunteer was instructed to inhale deeply and at the end of the expiration, a high-speed, short amplitude thrust was performed in the posterosuperior direction. However, if a cavitation did not occur on the first attempt, the participant was repositioned, and a second thrust was performed. On the other hand, no more than 2 thoracic spine thrusts were performed per participant [5]. The physiotherapist who performed and controlled the interventions had at least 10 years of clinical experience.
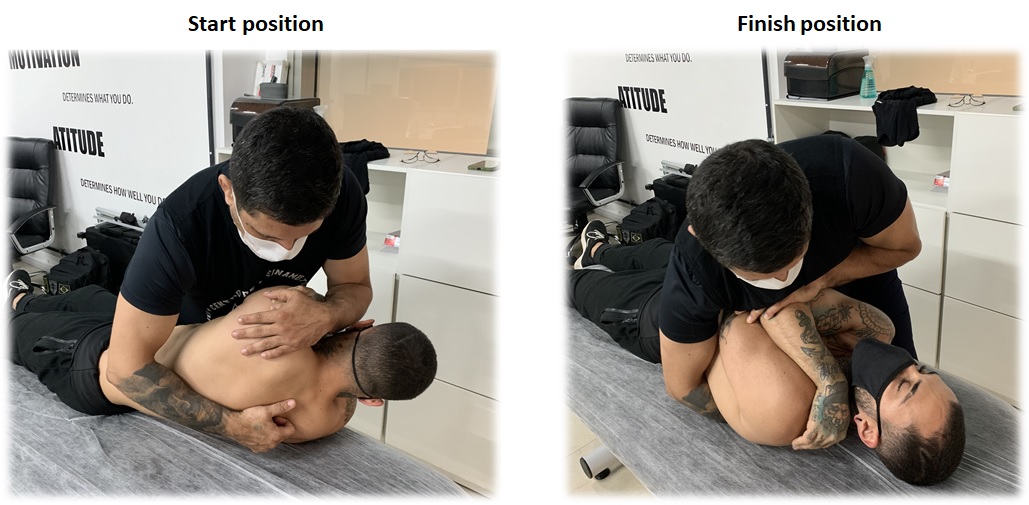
Figure 3: Start and finish position of thoracic spine thrust manipulation of the T3 vertebral segment.
Statistical analysis
All data are presented as mean ± SD. Statistical analysis was initially performed using the Shapiro-Wilk normality test and the homocedasticity test (Bartlett criterion). To test the reproducibility between the tests, the intraclass correlation coefficient (ICC) was used. Two-way analysis of variance (ANOVA) was used to test for main and interaction effects of the group (men and women) and timing of measurement for each outcome variable independently and the post hoc Bonferroni was used to possibility a statistically significant. Student’s t-test was used to assess differences between tests in the baropodometry platform (before vs. after TST-manipulation). The effect size (ES) was assessed using Cohen’s d. Values of d < 0.1, from 0.1 to <0.20, from 0.20 to <0.50, from 0.50 to <0.80, and ≥0.80 were considered as trivial, small, moderate, large and very large, respectively. The significance level was set at 0.05 and the software used for statistics was GraphPad® (Prism 6.0, San Diego, CA, USA).
Results
Table 1 compares the plantar surface area between men and women. The two-way ANOVA yielded main effects for group in left foot (F1.72 = 27.29, p< .0001) and right foot (F1.72 = 46.38, p< .0001) such that Bonferroni post- hoc showed significant differences in plantar surface area (cm2) between men and women group pre- and post-manual therapy (Table 1). On the other hand, the right foot was significantly different (p< .01) in plantar surface area (cm2) between pre- and post-manual therapy in women (Table 1). However, right forefoot (F1.72 = 12.72, p< .0006) and right hindfoot (F1.72 = 12.83, p< .0006) showed main effects for groups demonstrating significant differences between men and women group only pre-manual therapy (Table 2). But women showed significant increase and decrease in right forefoot (p<.01) and hindfoot (p<.03) post-manual therapy, respectively (Table 2). On the other hand, nonsignificant difference was observed in plantar surface area maximum pressure and mean pressure between men and women group pre- and post-manual therapy (Tables 3 and 4).
|
|
|
MEN |
WOMEN |
95% CI |
p< |
ES (a.u.) |
|
PRE |
Right |
99.10 ± 20.21 |
68.36 ± 11.50 |
-30.74 (-44.38 to -17.09) |
0.001 |
1.86 (very large) |
|
Left |
94.29 ± 18.10 |
71.60 ± 12.28 |
-22.69 (-36.31 to -9.06) |
0.001 |
1.47 (very large) |
|
|
POST |
Right |
100.20 ± 18.02 |
73.52 ± 12.80* |
-26.67 (-40.3 to -13.03) |
0.001 |
1.70 (very large) |
|
Left |
95.56 ± 19.59 |
74.28 ± 13.87 |
-21.28 (-34.91 to -7.65) |
0.01 |
1.25 (very large) |
|
|
* p<.01 – pre vs. post right foot women. |
||||||
|
|
|
MEN |
WOMEN |
95% CI |
p< |
ES (a.u.) |
|
Forefoot (PRE) |
Right |
44.22 ± 9.08 |
33.48 ± 11.73 |
-10.74 (-19.22 to -2.25) |
0.01 |
1.02 (very large) |
|
Left |
44.11± 9.53 |
43.23 ± 7.66 |
- 0.88 (-8.55 to 6.78) |
>0.05 |
0.10 (small) |
|
|
Forefoot (POST) |
Right |
46.91 ± 11.48 |
38.94 ± 11.01* |
- 7.96 (-16.45 to 0.52) |
>0.05 |
0.70 (large) |
|
Left |
43.25 ± 10.70 |
45.94 ± 9.50 |
2.68 (-4.98 to 10.36) |
>0.05 |
0.26 (moderate) |
|
|
Hindfoot (PRE) |
Right |
55.48± 9.50 |
66.52 ± 11.73 |
11.03 (2.45 to 19.61) |
0.01 |
1.03 (very large) |
|
Left |
55.89 ± 9.53 |
56.77 ± 7.66 |
0.88 (-6.78 to 8.55) |
>0.05 |
0.10 (small) |
|
|
Hindfoot (POST) |
Right |
53.09 ± 11.48 |
61.06 ± 11.01** |
7.96 (-0.61 to 16.54) |
>0.05 |
0.70 (large) |
|
Left |
56.75 ± 10.70 |
54.06 ± 9.50 |
-2.68 (-10.36 to 4.98) |
>0.05 |
0.25 (moderate) |
|
|
* p<0.01 – pre vs. post right forefoot women. ** p<0.03 – pre vs. post right hindfoot women. |
||||||
|
|
|
MEN |
WOMEN |
95% CI |
p< |
ES (a.u.) |
|
PRE |
Right |
1.24 ± 0.42 |
1.53 ± 0.47 |
0.29 (-0.08 to 0.66) |
>0.05 |
0.65 (large) |
|
Left |
1.31 ± 0.41 |
1.26 ± 0.53 |
- 0.03 (-0.37 to 0.29) |
>0.05 |
0.10 (small) |
|
|
POST |
Right |
1.28 ± 0.49 |
1.49 ± 0.56 |
0.20 (-0.16 to 0.58) |
>0.05 |
0.39 (moderate) |
|
Left |
1.35 ± 0.40 |
1.28 ± 0.35 |
-0.07 (-0.40 to 0.25) |
>0.05 |
0.18 (small) |
|
|
|
MEN |
WOMEN |
95% CI |
p< |
ES (a.u.) |
|
PRE |
Right |
0.34 ± 0.08 |
0.39 ± 0.09 |
0.04 (-0.02 to 0.11) |
>0.05 |
0.58 (large) |
|
Left |
0.38 ± 0.09 |
0.37 ± 0.08 |
-0.00 (-0.06 to 0.06) |
>0.05 |
0.11 (small) |
|
|
POST |
Right |
0.35 ± 0.09 |
0.40 ± 0.10 |
0.04 (-0.02 to 0.11) |
>0.05 |
0.52 (large) |
|
Left |
0.37 ± 0.8 |
0.38 ± 0.08 |
0.01 (-0.05 to 0.07) |
>0.05 |
0.12 (small) |
Discussion
This study aimed at investigating the contribution of the TST manipulation in the plantar pressure distribution between trained men and women. The main results obtained with this study were that (a) men showed greater plantar surface area (cm2) when compared to women pre- and post-TST manipulation, (b) right foot women showed increased plantar surface area (cm2) post-manual therapy, (c) the right foot distribution of the plantar surface area (%) revealed an increase and decrease in forefoot and hindfoot post-manual therapy in women, respectively.
Anatomical or biomechanical variations between men and women can directly intervene in plantar surface area. This statement corroborates our results, which were observed in greater plantar surface area in men. Some studies reported differences in feet and gait-related anatomy and habits between men and women [9,10]. Other studies showed that males had a foot longer, higher plantar fascia, and heel fat pad thickness compared to women [11,12]. In general, men and women feet are different to varying degrees with respect to arch lateral side of the foot, the first toe, heel-to-toe length, ball length, ball width, ball circumference, malleoli height, and arch dimensions [11-13]. These differences should be considered in relation to greater plantar surface area in static conditions in men when compared to women. On the other hand, the plantar surface area of the right foot women increased post-TST manipulation. A hypothetical explanation for this result may be related to decrease in conduction velocity that alters motor unit recruitment patterns and lower twitch torque motor units in lower limbs post-spinal manipulation [6]. This response possibly promotes reduced muscle tension and may contribute to the increase in plantar surface area due to the impact on motor control.
In relation to the percentage distribution of the plantar surface area, the scientific literature has shown that a normal distribution of healthy subjects has been around 60% on the hindfoot and 40% on the forefoot, with a tolerance of – 4% [14,15]. In present study, differences were observed in the fore-/Hind-foot in right foot load distribution parameters between men and women before manual therapy, i.e., sex difference showed an increase of 24% in right forefoot in men, while women showed 16.6% greater plantar load distribution in right hindfoot. Corroborating with ours results, a study showed that men subjects had greater plantar soft tissue thickness on metatarsal heads (medial forefoot and lateral forefoot) in relation to women [16]. These results support the concept that all the heads of the metatarsal bones bear weight during quiet standing [17,18]. On the other hand, we observed greater plantar load distribution in right hindfoot before manual therapy in women. Thus, the greatest magnitude of plantar load distribution in hindfoot may be associated with the functional shortening of the superficial dorsal line, disturbed muscle tension on the plantar surface, or shortening of the hamstring muscles [19,20]. However, the question arises whether the greater soft tissue thickness in forefoot and hindfoot can bear and adapt to the greater peak pressure or pressure-time integral. Remember that excess forefoot loading may be associated with a shortening of the anterior superficial line of the fascia and cause significant metatarsal and plantar aponeurosis pain [20]. On the other hand, excess hindfoot loading can contribute to dysfunction of the subtalar joint and possibly compromising plantar flexion, adduction and inversion in one direction and dorsiflexion, abduction, and eversion in the opposite direction [16].
The distribution of body weight through the foot depends on the shape of the arch and the location of the line of gravity at a given moment. In addition, asymmetric plantar load distribution has also been investigated in the scientific literature [21,22]. Ours study revealed asymmetry in the plantar load distribution during static condition before manual therapy in women, i.e., was observed a difference between the left vs. right of 22.6% in forefoot and a difference of 14.7% between the left vs. right in hindfoot. The presence of asymmetry between the feet can be an indication that there has been a notable negative impact on normal foot function and unequal loading of the two feet, as limb function [21-23]. We may hypothesize that way of loading and setting of the foot is often the result of biomechanical variations from structural changes in the spine that can cause asymmetry of foot loads, weakening of their muscle, ankle stabilization, and gait asymmetry [24]. However post- manual therapy, a reduction in asymmetry (left vs. right foot) was observed, 15.2% in the forefoot and 11.4% in the hindfoot in females. Likewise, we also observe an increase (14.1%) and decrease (8.2%) in right forefoot and hindfoot post-manual therapy in women. It appears that our results are associated with TST manipulation because spinal manipulation improves the release of entrapped synovial folds or plica, promote relaxation of hypertonic muscle by sudden stretching, contribute to disruption of articular or periarticular adhesions and repair the unbuckling of motion segments that have undergone disproportionate displacements [25]. Furthermore, other studies have shown that an improvement in postural control from the reduction in sway speed immediately post-TST manipulation can be attributed to improved sensorimotor integration and increased proprioception from induced changes in the discharge of mechanoreceptors from the paraspinal region, especially group Ia spindle afferents [26,27].
The limitations of the study include the absence of control group and measures of physiological parameters and electromyographic evaluation, which would be interesting; yet this does not limit the answer to the study question. However, we recognize the potential for unmeasured confusion. In addition, longitudinal studies are needed to define a cause-and-effect relationship and differences between techniques of TST manipulation in relation to sex differences.
Conclusion
The results of this investigation confirm that TST manipulation improved the plantar surface area and distribution of the plantar surface area in women. These findings are related to the women right foot that showed increased plantar surface area and significant changes in the distribution of the plantar surface area. These data contribute to the qualitative and quantitative understanding of sex differences in stability condition by using TST manipulation. Therefore, the use of TST manipulation is recommended, in an acute manner, as it has been shown to be efficient in stabilizing women.
Conflict of Interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
2. Henley CE, Ivins D, Mills M, Wen FK, Benjamin BA. Osteopathic manipulative treatment and its relationship to autonomic nervous system activity as demonstrated by heart rate variability: a repeated measures study. Osteopath Med Prim Care. 2008 Jun 5;2:7.
3. Bialosky JE, Bishop MD, Price DD, Robinson ME, George SZ. The mechanisms of manual therapy in the treatment of musculoskeletal pain: a comprehensive model. Man Ther. 2009 Oct;14(5):531-8.
4. Espí-López GV, Rodríguez-Blanco C, Oliva-Pascual-Vaca A, Molina-Martínez F, Falla D. Do manual therapy techniques have a positive effect on quality of life in people with tension-type headache? A randomized controlled trial. Eur J Phys Rehabil Med. 2016 Aug;52(4):447-56.
5. Hartstein AJ, Lievre AJ, Grimes JK, Hale SA. Immediate Effects of Thoracic Spine Thrust Manipulation on Neurodynamic Mobility. J Manipulative Physiol Ther. 2018 May;41(4):332-41.
6. Robinault L, Holobar A, Crémoux S, Rashid U, Niazi IK, Holt K, et al. The Effects of Spinal Manipulation on Motor Unit Behavior. Brain Sci. 2021 Jan 14;11(1):105.
7. Bicalho E, Setti JA, Macagnan J, Cano JL, Manffra EF. Immediate effects of a high-velocity spine manipulation in paraspinal muscles activity of nonspecific chronic low-back pain subjects. Man Ther. 2010 Oct;15(5):469-75.
8. Haavik H, Murphy B. The role of spinal manipulation in addressing disordered sensorimotor integration and altered motor control. J Electromyogr Kinesiol. 2012 Oct;22(5):768-76.
9. Putti AB, Arnold GP, Abboud RJ. Foot pressure differences in men and women. Foot Ankle Surg. 2010 Mar;16(1):21-4.
10. Cho SH, Park JM, Kwon OY. Gender differences in three dimensional gait analysis data from 98 healthy Korean adults. Clin Biomech (Bristol, Avon). 2004 Feb;19(2):145-52.
11. Taş S. Effect of Gender on Mechanical Properties of the Plantar Fascia and Heel Fat Pad. Foot Ankle Spec. 2018 Oct;11(5):403-9.
12. Luo G, Houston VL, Mussman M, Garbarini M, Beattie AC, Thongpop C. Comparison of male and female foot shape. J Am Podiatr Med Assoc. 2009 Sep-Oct;99(5):383-90.
13. Kandil OD, Aboelazm SN, Mabrouk MS. Foot biometrics: gender differences in plantar pressure distribution in standing position. Am J Biomed Eng. 2014;4(1):1-9.
14. Pomarino D, Pomarino A. Plantar Static Pressure Distribution in Healthy Individuals: Percentiles for the Evaluation of Forefoot Loading. Foot Ankle Spec. 2014 Aug 1;7(4):293-7.
15. Sarpong NO, Swindell HW, Trupia EP, Vosseller JT. Republication of "Metatarsal Fractures". Foot Ankle Orthop. 2023 Aug 6;8(3):24730114231193428.
16. Koo S, Chun S, Lee KM, Cho BC, Koo YJ, Kang DW, et al. Sex Differences in Pedobarographic Findings and Relationship between Radiographic and Pedobarographic Measurements in Young Healthy Adults. Clin Orthop Surg. 2018 Jun;10(2):216-24.
17. Koenraadt KL, Stolwijk NM, van den Wildenberg D, Duysens J, Keijsers NL. Effect of a metatarsal pad on the forefoot during gait. J Am Podiatr Med Assoc. 2012 Jan-Feb;102(1):18-24.
18. Lord M. Foot pressure measurement: a review of methodology. J Biomed Eng. 1981 Apr;3(2):91-9.
19. Hoover DL, Carlson KM, Christensen BK, Zebas CJ. Biomechanical analysis of women weightlifters during the snatch. J Strength Cond Res. 2006 Aug;20(3):627-33.
20. Hawrylak A, Gronowska H. Plantar Pressure Distribution in Female Olympic-Style Weightlifters. Int J Environ Res Public Health. 2020 Apr 13;17(8):2669.
21. Sadeghi H, Allard P, Prince F, Labelle H. Symmetry and limb dominance in able-bodied gait: a review. Gait Posture. 2000 Sep;12(1):34-45.
22. Wafai L, Zayegh A, Woulfe J, Aziz SM, Begg R. Identification of Foot Pathologies Based on Plantar Pressure Asymmetry. Sensors (Basel). 2015 Aug 18;15(8):20392-408.
23. Zifchock RA, Davis I, Higginson J, Royer T. The symmetry angle: a novel, robust method of quantifying asymmetry. Gait Posture. 2008 May;27(4):622-7
24. Buldt AK, Allan JJ, Landorf KB, Menz HB. The relationship between foot posture and plantar pressure during walking in adults: A systematic review. Gait Posture. 2018 May;62:56-67.
25. Shekelle PG. Spinal manipulation. Spine (Phila Pa 1976). 1994 Apr 1;19(7):858-61.
26. Devi U, Anumula SK, Suhail A. Effect of Thoracic Manipulation on Pain and Postural Sway in Chronic Mechanical Neck Pain Patients: A Quasi-experimental Study. Journal of Clinical & Diagnostic Research. 2021 Oct 1;15(10):YC01-5.
27. Ditcharles S, Yiou E, Delafontaine A, Hamaoui A. Short-Term Effects of Thoracic Spine Manipulation on the Biomechanical Organisation of Gait Initiation: A Randomized Pilot Study. Front Hum Neurosci. 2017 Jun 30;11:343.