Commentary
The FLAMSA concept was designed as a conditioning regimen for acute leukemia separating leukemia therapy from reduced intensity conditioning. Leukemia treatment consists of a short and intensive chemotherapy followed after a 3-day rest by conditioning with intensive immune suppression and reduced intensity of myeloablative (stem cell toxic) treatment preferably total body irradiation (TBI). Furthermore, it included T cell depletion “in vivo” with antithymocyte globulin (ATG) for prophylaxis of graft-versus-host disease followed by restitution of immunity by the transfusion of donor lymphocytes [1-3]. The first experiences in patients with high-risk acute myeloid leukemia were encouraging; survival of relapsed and primary refractory patients was improved as compared to previous studies. Duration and intensity of prior chemotherapy was critical; patients with primary refractory disease and no more than 2 cycles of therapy had an excellent chance of continued remission [4,5].
The concept of FLAMSA sequential conditioning was convincing to many groups; reports of single centers and multicenter studies were published [6-19] (Table 1). Several studies used busulfan [20], treosulfan [21-24], or melphalan [16] instead of total body irradiation (TBI), retrospective comparisons found results equivalent of FLAMSA-TBI to myeloablative conditioning [25]. However, there are several reports on retrospective studies [26], only one prospective randomized study of FLAMSA compared to other forms of conditioning (FIGARO trial) described no improvement of relapse rate and survival with FLAMSA [27]. In contrast to the original study most patients in the FIGARO trial were in remission; these patients had less benefit from additional chemotherapy. In the original FLAMSA study chemotherapy with cytarabine (ARA-C), fludarabine and amsacrine was necessary to reducing blasts immediately prior to conditioning with total body irradiation, antithymocyte globulin and cyclophosphamide.
| Study | No of pats. | Conditioning | Non-relapse Mortality* | Rel inc.* | Survival (time)* | Reference |
| Original | 75 | FLAMSA + 4Gy TBI, ATG, CY | 33%(1yr) | n.a. | 42% | [1] [4] |
| German multicenter | 121 20 |
FLAMSA-TBI FLAMSA-BUS | 18% na |
28% na |
44% (4yr) na |
[10] |
| British multicenter random. trial | 176 | FLAMSA -BUS control |
20% (1yr) 16% (1yr) |
26.7% 29.5% |
56% 57% |
[27] |
| French Study refractory or relapsed AML | 58 41 |
FLAMSA/clofarabin myeloablative | 17% 15% |
57% 50% |
33% 39% |
[70] |
| HR MDS upfront Duesseldorf | 30 | Mel 24pts Mel+TT 6 pts. | 20% (4yrs) 66% (4Yrs) |
30% | 70% | [51] |
| AML elderly median age 46 | 72 58 |
FLAMSA-TBI FLAMSA-Treo | 13% 28% |
70% 35% |
47% 43% |
[23] |
| AML high risk rel/ref poor cytogenetkics |
60 | FLAMSA-TBI | 28% | n.a. | 42% | [6] |
| AML r/R | 31 12 |
FLAMSA-TBI FLAMSA-Bu | 20-26% | n.a. | 39% | [18] |
| refr AML | 34 10 |
FLAMSA-TBI FLAMSA-BUS | 18%& | 69 | 15% | [11] |
| AML active dis haplo | 21 12 |
FLAMSA-TBI/Bus Clof-TBI |
15% | 35% | 48% | [19] |
| EBMT study rel/refr | 213 40 13 |
FLAMSA -TBI 4Gy FLASMA-BU-CY FLAMSA-BU or Mel | 25,9% | 48,5% | 30,4% | [13] |
| EBMT high risk AML in remission | 159 106 |
FLAMSA-TBI FLAMSA-BUS | 19.4% 31.1% |
21.2% 25.7% |
62% 46.7% |
[7] |
| EBMT CR1/CR2** | 203 145 281 |
FLAMSA-TBI FLAMSA-BUS Treo/Flu |
15,2% 25,2% 13,2% |
20,4% 27,6% 39% |
69% 53,4% 59,9% |
[21] |
| EBMT CR1/CR2 | 1197 258 141 |
FLU-BUS FLAMSA-TBI FLAMSA -Bus | 16.1% 16,4% 26,7% |
30,3% 21,9% 23,1% |
60% 69% 49,4% |
[20] |
| EBMT study refr/rel | 113 112 631 |
FLU-Treo TBF (Thiot BU Flu) FLAMSA |
5% 13% 6% |
46% 54% 53% |
37% 24% 34% |
[24] |
| EBMT refr/rel |
258 314 318 128 |
BUS-CY CY-TBI FLAMSA-TBI FLAMSA-Chemoa |
16% 19% 18% 7% |
56% 51% 55% 53% |
33% 34% 36% 50% |
[14] |
*If not otherwise indicated 2 years
**Significant differences in year of transplant, patient age, remission status, FLT3-ITD, CMV seropositivity, in vivo T cell depletion, stem cell source (bonemarrow vs. pbsc)
a chemo included busulfan 6,4 mg/kg, or melphalan or CY or treosulfan TBI dose 4 Gy without info on fractionation and dose rate, oral busulfan and ex vivo T depletion were excluded; ATG treatment not specified, DLI not given
Table 1:
A second finding of the FIGARO trial was that the rate of patients with minimal (measurable) residual disease (MRD) was not reduced despite additional FLAMSA chemotherapy. MRD is characterized as disease surviving standard chemotherapy. In acute myeloid leukemia (AML) residual disease most likely differs qualitatively form the bulk of blasts. Leukemia cells constituting MRD are resistant to most chemotherapy because they are enriched of dormant or slowly proliferating cells, presumably leukemia stem cells. These cells cannot be eliminated by a short intensive chemotherapy, they can only be killed independently of their cell cycle by radiation or stem cell toxic (myeloablative) drugs as busulfan, treosulfan, melphalan, thiotepa and similar. In the FIGARO trial busulfan in reduced doses was given in both arms. The original FLAMSA regimen contained total body irradiation (TBI) with 4 Gy. On an average, 4 Gy radiation inactivates 99 percent of progenitor cells. Ideally TBI was applied as a single dose at very low dose rates (<10cGy/min). This way the inactivation of hematopoietic progenitor cells was improved in relation to non-hematopoietic toxicities [28]. Normal stem cells compete with leukemia stem cells for the niche in the bone marrow [29], the niche being adjusted to the leukemia stem cell. These leukemia stem cells are protected against chemotherapy in the niche. Therefore, it is important to achieve full donor chimerism as soon as possible. Three months after transplantation full donor chimerism was achieved in only 50 percent of patients in the FIGARO trial [27] as compared to virtually all patients in the original FLAMSA trial [1]. The intensity of conditioning may not be important for patients transplanted in remission; it is important for patients transplanted with active disease [30]. TBI has the advantage of exact dosing and the inclusion of metabolically restricted sites, it has the disadvantage of the requirement of a large field radiation facility. Therefore, multicenter studies with radiation are difficult to perform. The combination of cyclophosphamide (CY) and anti-thymocyte globulin (ATG) may also contribute to the induction of complete chimerism at 3 months. This combination has been successful to abrogate sensitization by prior transfusions in dogs [31] and in conditioning patients with severe aplastic anemia [32].
Thirdly, the higher incidence of acute GVHD may be caused by insufficient T cell depletion. The use of mobilized blood stem cells instead of marrow comprises a higher content of T cells. T cell antibodies should persist in the patient in significant concentrations to inactivate donor T cells. Dependent on the preparation of ATG 60 mg/kg are enough to inactivate donor T cells “in vivo” [33], saturation of CD52 by alemtuzumab was sufficient and GVHD prevented with 30 mg in the HLA-identical situation [34]. Higher doses were complicated by infections and delayed immune restitution [34].
The fourth component of sequential therapy, donor lymphocyte transfusions (DLI) were planned for restitution of immunity after T cell depletion. Adjuvant DLI were beneficial in a matched case comparison [35], but many centers were reluctant because of the risk of GVHD. A recent time dependent analysis of DLI after FLAMSA conditioning in high-risk AML did not find a benefit of DLI [36]. However, a study of similar patients receiving ex vivo T cell depleted transplants showed a significant benefit of DLI [37]. Furthermore, post-transplant relapses could be treated with donor cells in combination with low dose cytarabine [38], or azacytdine [39]. In some patients with more aggressive relapses FLAMSA and donor cells without reduced intensity conditioning were helpful (personal observation). Contrary to CML, AML may be rapidly progressive and unable to differentiate dendritic cells of leukemia origin [40]. We advised DLI after discontinuation of post-grafting immune suppressive treatment and absence of GVHD for 30 days. As a rule, this can be initiated between 120 and 160 days after transplant. DLI should be given in escalating doses starting with low doses between 1 x 106/kg and 1 x 107 /kg T cells. Even then, infections in particular viral infections can set off GVHD. Therefore, precautions should be taken to prevent infections. In the FIGARO trial, DLI were not regularly given, only in patients with mixed chimerism and impending relapse.
The FLAMSA regimen is conceptual for further steps to improve outcome of allogeneic stem cell transplantation (Figure 1). Active and primary refractory disease was well controlled by fludarabine and cytosine arabinoside (ARA-C) and amsacrine as non-cross-reactive drug for antracyclins. The substitution of fludarabin by clofarabine has been advocated by some colleagues [41], but more severe gastrointestinal toxicity has restricted its use. Today we have several new options for improvement: a liposomal formulation of the fixed combination of ARA-C and daunorubicin (CPX351) gave better responses and less toxicity than the conventional 7+3 regimen of ARA-C and daunorubicine [42], targeted drugs to FLT-3 [43], IDH-1 [44] and IDH-2 [45] as well as BCL-2 [46]. Combinations of the hypomethylating agent azacytidine [47] with the BCL2 inhibitor venetoclax [48] or with the IDH-1 inhibitor ivosidenib [44] or the IDH-2 inhibitor enasidenib [45] have been combined with great success. Histone deacetylase inhibitors Panobinostat [49] and vorinostat [50] have also been studied in AML. These new treatments may substitute the antileukemia part of FLAMSA in elderly and frail patients. They induce remissions or reduce blasts to a level at which conditioning with reduced intensity is sufficient to control rejection, GVHD and permit complete donor chimerism. This way even elderly patients may have a chance for transplantation without intensive chemotherapy [51]. Myeloablation with higher doses of radiation or intensive stem-cell toxic chemotherapy as busulfan, treosulfan, melphalan, thiotepa and others may not be necessary. FLAMSA 4 Gy TBI has been found equivalent to myeloablative conditioning in primary refractory and relapsed AML [25]. Unfortunately, levels of MRD were not reported. Cyclophosphamide combined with ATG enhances the generation of complete chimerism. The dose of cyclophosphamide may be reduced in elderly and unfit patients, the reduction to 50 mg/kg was sufficient for conditioning for transplantation in patients with severe aplastic anemia [52]. Antibody conditioning is still in its preclinical stage [53], but recent personalized targeted radio-immunotherapy trials are promising [54]. In this latter trial chimerism was complete at day 100 in over 90 percent of patients.
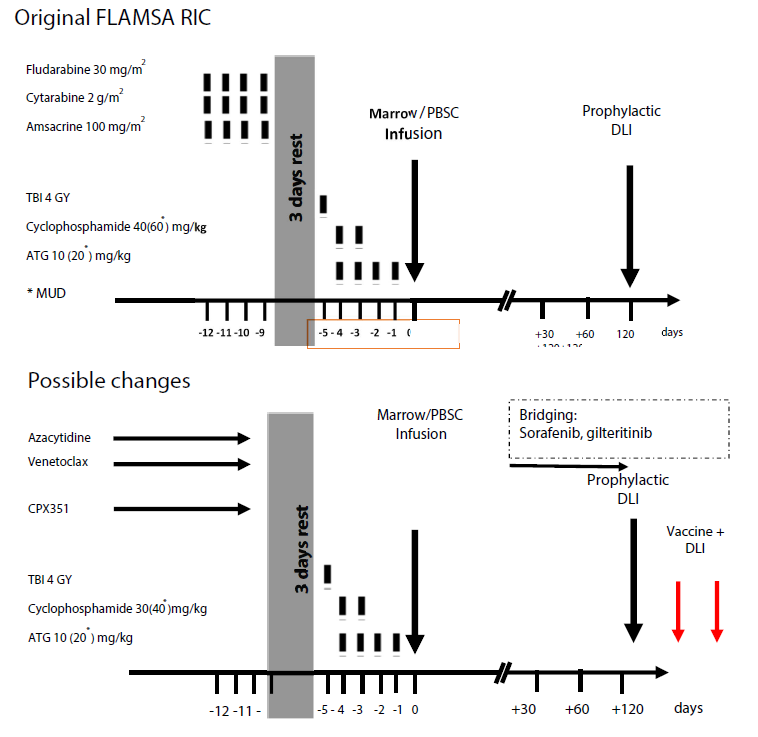
Figure 1: a. The original FLAMSA protocol and possible improvements, and b. Possible modifications. TBI: Total Body Irradiation; ATG: Antithymocyte Globulin (Neovii); MUD: Matched Unrelated Donor; PBSC: Peripheral Blood Stem Cells; DLI: Donor Lymphocyte Transfusions; CPX351: Liposomal formulation Of Cytarabine/Daunorubicin; BsAB: Bispecific Antibody; CAR-DLI: Chimeric Antigen Receptor T cell as DLI.
DLI should restore immune capacity after the depletion of T cells. They could be stored away at the time of transplantation or collected prior to use. The major risk of the transfusion of unmodified donor lymphocytes is GVHD. One precaution is the delay of DLI until tolerance is established and immunosuppressive treatment can be discontinued. The second precaution is repeated transfusions and escalated doses starting at low doses of 1 x 106/kg T cells. A third precaution is the prevention of infection, because they can set off GVHD by inflammation, production of interferons and expression of HLA class II in non-hematopoietic cells. As a rule, the time lag after transplantation is 4 to 5 months including a month off immunosuppressive therapy. During this time rapidly proliferative forms of leukemia tend to relapse. Early relapses are a common problem of FLT3 mutated leukemia, maintenance treatment with sorafenib [55] can prevent relapse. Sorafenib could be started 2 to 3 months after transplantation. Patients with persistent MRD positivity may not benefit, DLI were not part of the protocol. Another maintenance treatment with Panobinostat is also beneficial in high risk MDS and AML [49]. Several ways have been explored to improve graft-versus-leukemia effects without increasing GVHD. In any case patients treated with DLI should be protected from infections. Anti-viral and anti-bacterial prophylaxis can be considered, perhaps also precautions as against SARS-COV 2 with masks, disinfection and safe distance.
The graft-versus-leukemia (GVL) effect of DLI is strong in chronic myelogenous leukemia (CML) in patients with relapse in chronic phase, it is less in transformed phase and in AML. GVL effects can be improved by manipulation of the effector cells and/or manipulation of the target cells and their antigen presentation. The selection of NK cells or cytokine induced killer (CIK) cells has been used with some success. HLA-haploidentical donors can be selected avoiding killer receptor inhibitors [56]. Depletion of T cells has been advised and NK cells generated from stem cells. Depletion of naive T cells can also help to prevent acute GVHD. Marrow infiltrating lymphocytes display tumor specificity and can be expanded, they consist mainly of central memory T cells [57]. T cells can be activated and expanded against multiple leukemia associated antigens (WT1, PRAME, NY-ESO-1, survivin), they show good activity in adjuvant treatment of remission patients [58]. However, loss of antigen, loss of HLA-heterozygosity, PD-L1 expression and infiltration of immune privileged sites results in immune escape. Transduction of EBV reactive T cells with a selected T cell receptor against WT-1 prevented relapse in 12 patients [59]. These approaches are restricted to HLA-A2 and the continued expression of WT1.
We studied improvement of GVL effects by improvement of antigen presentation by differentiation of leukemia blasts to dendritic cells of leukemia origin [60,61]. In contrast to chronic myelogenous leukemia (CML) where antigen expression is stable during chronic phase and long-lasting remissions can be induced, continued differentiation of AML blasts is difficult to achieve. Immune effects of targeted therapies may help. In some cases of azacytidine treatment cytotoxic T cells could be activated against testis antigens [47]. Azacytidine may also initiate the production of endogenous human retrovirus [62]. This way the leukemia cells may become immunogenic. Sorafenib leads to the release of IL 15 [63]. Peptide vaccination may be a way to improve graft- versus-leukemia reactions. Mutated regions of nucleophosmin I have elicited CD4 and CD8 responses in patients with AML [64] and neoepitopes of FLT3 internal tandem duplication (ITD) were recognized by autologous CD8 cells [65]. Recognition of peptides is better by allogeneic T cells than autologous T cells [66]. Therefore, peptide primed DLI may be helpful. Another way to improve the GVL reaction, is treatment with a bispecific antibody that leads to T cell activation on binding with CD123 target antigen [67]. Recent advances in the generation of chimeric antigen receptor positive T cells have also a good chance to induce immunity to AML blasts via binding to CD13 and TIM 3 [68]. Allogeneic CAR-T cells may have advantages in the recognition of neo-antigens, in the effector function and persistence [69].
In summary FLAMSA may be modified by remission induction or blast reduction with targeted therapy Conditioning should include doses of TBI, melphalan, treosulfan or busulfan sufficient for the elimination of MRD and induction of complete donor chimerism at day 100, in vivo depletion of T cells and immune restitution with DLI. Open questions remain the form and duration of maintenance therapy until DLI and the optimal way of applying DLI for improvement of graft-versus-leukemia effects without the risk of severe GVHD.
References
2. Schmid C, Schleuning M, Hentrich M, Markl GE, Gerbitz A, Tischer J, et al. High antileukemic efficacy of an intermediate intensity conditioning regimen for allogeneic stem cell transplantation in patients with high-risk acute myeloid leukemia in first complete remission. Bone Marrow Transplantation. 2008 Apr;41(8):721-7.
3. Schleuning M, Schmid C, Ledderose G, Tischer J, Humann M, Ullmann J, et al. Durable Remission after Prophylactic Donor Lymphocyte Transfusion Following Allogeneic Stem Cell Transplantation with Reduced Conditioning for High-Risk AML and MDS. Blood. 2004;104(11).
4. Schmid C, Schleuning M, Schwerdtfeger R, Hertenstein B, Mischak-Weissinger E, Bunjes D, et al. Long-term survival in refractory acute myeloid leukemia after sequential treatment with chemotherapy and reduced-intensity conditioning for allogeneic stem cell transplantation. Blood. 2006 Aug 1;108(3):1092-9.
5. Kolb HJ, Schmid C. The FLAMSA concept—past and future. Annals of Hematology. 2020;99(9):1979-1988.
6. Krejci M, Doubek M, Dusek J, Brychtova Y, Racil Z, Navratil M, et al. Combination of fludarabine, amsacrine, and cytarabine followed by reduced-intensity conditioning and allogeneic hematopoietic stem cell transplantation in patients with high-risk acute myeloid leukemia. Annals of Hematology. 2013 Oct;92(10):1397-403.
7. Malard F, Labopin M, Stuhler G, Bittenbring J, Ganser A, Tischer J, et al. Sequential intensified conditioning regimen allogeneic hematopoietic stem cell transplantation in adult patients with intermediate-or high-risk acute myeloid leukemia in complete remission: a study from the Acute Leukemia Working Party of the European Group for Blood and Marrow Transplantation. Biology of Blood and Marrow Transplantation. 2017 Feb 1;23(2):278-84.
8. Michallet M, Sobh M, Detrait MY, Labussiere-Wallet H, Hayette S, Tigaud I, et al. Flamsa Sequential Chemotherapy Followed By Reduced Intensity Conditioning and Allogeneic Hematopoietic Transplantation for High Risk Acute Myeloid Leukemia Patients. Blood. 2014;124(21).
9. Pfeiffer T, Schleuning M, Eder M, Krejci M, Kolbe K, Scheid C, et al. Improved Outcome for Patients with Acute Myeloid Leukemia (AML) and Myelodysplastic Syndrome (MDS) with Poor Risk Cytogenetics–Result from An Analysis on 172 Patients Receiving FLAMSA-RIC Conditioning for Allogeneic Stem Cell Transplantatioin (SCT). Blood. 2008 Nov 16;112(11):1971.
10. Pfeiffer T, Schleuning M, Mayer J, Haude KH, Tischer J, Buchholz S, et al. Influence of molecular subgroups on outcome of acute myeloid leukemia with normal karyotype in 141 patients undergoing salvage allogeneic stem cell transplantation in primary induction failure or beyond first relapse. Haematologica. 2013 Apr;98(4):518-25.
11. Pfrepper C, Klink A, Behre G, Schenk T, Franke GN, Jentzsch M, et al. Risk factors for outcome in refractory acute myeloid leukemia patients treated with a combination of fludarabine, cytarabine, and amsacrine followed by a reduced-intensity conditioning and allogeneic stem cell transplantation. Journal of Cancer Research and Clinical Oncology. 2016 Jan 1;142(1):317-24.
12. Ram R, Scheid C, Amit O, Chemnitz JM, Moshe Y, Hallek M, et al. Sequential therapy for patients with primary refractory acute myeloid leukemia: a historical prospective analysis of the German and Israeli experience. Haematologica. 2019 Sep;104(9):1798.
13. Ringdén O, Labopin M, Schmid C, Sadeghi B, Polge E, Tischer J, et al. Sequential chemotherapy followed by reduced-intensity conditioning and allogeneic haematopoietic stem cell transplantation in adult patients with relapse or refractory acute myeloid leukaemia: a survey from the Acute Leukaemia Working Party of EBMT. British Journal of Haematology. 2017 Feb;176(3):431-9.
14. Rodríguez-Arbolí E, Labopin M, Tischer J, Brecht A, Ganser A, Finke J, et al. FLAMSA-Based Reduced-Intensity Conditioning versus Myeloablative Conditioning in Younger Patients with Relapsed/Refractory Acute Myeloid Leukemia with Active Disease at the Time of Allogeneic Stem Cell Transplantation: An Analysis from the Acute Leukemia Working Party of the European Society for Blood and Marrow Transplantation. Biology of Blood and Marrow Transplantation. 2020 Nov 1;26(11):2165-73.
15. Saraceni F, Labopin M, Brecht A, Kröger N, Eder M, Tischer J, et al. Fludarabine-treosulfan compared to thiotepa-busulfan-fludarabine or FLAMSA as conditioning regimen for patients with primary refractory or relapsed acute myeloid leukemia: a study from the Acute Leukemia Working Party of the European Society for Blood and Marrow Transplantation (EBMT). Journal of Hematology & Oncology. 2019 Dec;12(1):1-0.
16. Saure C, Schroeder T, Zohren F, Groten A, Bruns I, Czibere A, et al. Upfront allogeneic blood stem cell transplantation for patients with high-risk myelodysplastic syndrome or secondary acute myeloid leukemia using a FLAMSA-based high-dose sequential conditioning regimen. Biology of Blood and Marrow Transplantation. 2012 Mar 1;18(3):466-72.
17. Schleuning M, Judith D, Kaltenhäuser J, Burlakova I, Taube R, Bertelsmann A, et al. P084 Excellent anti-leukaemic efficacy of allogeneic-SCT after FLAMSA chemotherapy and reduced intensity conditioning in patients with high-risk myeloid malignancies aged 60 years or older. Leukemia Research. 2007(31):S101-2.
18. Schneidawind D, Federmann B, Faul C, Vogel W, Kanz L, Bethge WA. Allogeneic hematopoietic cell transplantation with reduced-intensity conditioning following FLAMSA for primary refractory or relapsed acute myeloid leukemia. Annals of Hematology. 2013 Oct;92(10):1389-95.
19. Fraccaroli A, Prevalsek D, Häbe SE, Bücklein V, Schulz C, Drolle H, et al. Favorable Outcome of Sequential HLA-Haploidentical Transplantation Using Ptcy As GvHD Prophylaxis in High Risk AML and MDS of the Elderly. Blood. 2018 Nov 29;132:3458.
20. Heinicke T, Labopin M, Schmid C, Polge E, Socié G, Blaise D, Mufti GJ, et al. Reduced relapse incidence with FLAMSA–RIC compared with Busulfan/Fludarabine for acute myelogenous leukemia patients in first or second complete remission: a study from the acute leukemia working party of the European Society for blood and marrow transplantation. Biology of Blood and Marrow Transplantation. 2018 Nov 1;24(11):2224-32.
21. Sheth V, Labopin M, Canaani J, Volin L, Brecht A, Ganser A, et al. Comparison of FLAMSA-based reduced intensity conditioning with treosulfan/fludarabine conditioning for patients with acute myeloid leukemia: an ALWP/EBMT analysis. Bone Marrow Transplantation. 2019 Apr;54(4):531-9.
22. Chemnitz JM, von Lilienfeld-Toal M, Holtick U, Theurich S, Shimabukuro-Vornhagen A, Krause A, et al. Intermediate intensity conditioning regimen containing FLAMSA, treosulfan, cyclophosphamide, and ATG for allogeneic stem cell transplantation in elderly patients with relapsed or high-risk acute myeloid leukemia. Annals of Hematology. 2012 Jan;91(1):47-55.
23. Holtick U, Herling M, Pflug N, Chakupurakal G, Leitzke S, Wolf D, et al. Similar outcome after allogeneic stem cell transplantation with a modified FLAMSA conditioning protocol substituting 4 Gy TBI with treosulfan in an elderly population with high-risk AML. Annals of Hematology. 2017 Mar 1;96(3):479-87.
24. Saraceni F, Labopin M, Brecht A, Kröger N, Eder M, Tischer J, et al. Fludarabine-treosulfan compared to thiotepa-busulfan-fludarabine or FLAMSA as conditioning regimen for patients with primary refractory or relapsed acute myeloid leukemia: a study from the Acute Leukemia Working Party of the European Society for Blood and Marrow Transplantation (EBMT). Journal of Hematology & Oncology. 2019 Dec;12(1):1-0.
25. Decroocq J, Itzykson R, Vigouroux S, Michallet M, Yakoub-Agha I, Beckerich F, et al. Allogeneic Hematopoietic Stem Cell Transplantation Offers Similar Outcome after Myeloablative and Sequential Conditioning Regimen in Patients with Primary Refractory or Relapsed Acute Myeloid Leukemia: A Study from the Societe Francaise De Greffe De Moelle Et De Therapie Cellulaire (SFGM-TC). Blood. 2015;126(23).
26. Owattanapanich W, Ungprasert P, Wais V, Kungwankiattichai S, Bunjes D, Kuchenbauer F. FLAMSA-RIC for stem cell transplantation in patients with acute myeloid leukemia and myelodysplastic syndromes: a systematic review and meta-analysis. Journal of Clinical Medicine. 2019 Sep;8(9):1437.
27. Craddock C, Jackson A, Loke J, Siddique S, Hodgkinson A, Mason J, et al. Augmented Reduced-Intensity Regimen Does Not Improve Postallogeneic Transplant Outcomes in Acute Myeloid Leukemia. Journal of Clinical Oncology. 2021 Mar 1;39(7):768-778.
28. Kolb HJ, Rieder I, Bodenberger U, Thierfelder S, Netzel B, Schaffer E, et al. Dose rate and dose fractionation studies in total body irradiation of dogs. Pathologie-biologie. 1979;27(6):370-2.
29. Bernasconi P, Borsani O. Targeting leukemia stem cell-niche dynamics: A new challenge in AML treatment. Journal of Oncology. 2019 Aug 7;2019.
30. Shimoni A, Hardan I, Shem-Tov N, Yeshurun M, Yerushalmi R, Avigdor A, et al. Allogeneic hematopoietic stem-cell transplantation in AML and MDS using myeloablative versus reduced-intensity conditioning: the role of dose intensity. Leukemia. 2006 Feb;20(2):322-8.
31. Storb R, Floersheim GL, Weiden PL, Graham TC, Kolb HJ, Lerner KG, et al. Effect of prior blood transfusions on marrow grafts: abrogation of sensitization by procarbazine and antithymocyte serum. The Journal of Immunology. 1974 Apr 1;112(4):1508-16.
32. Storb R, Blume KG, O'Donnell MR, Chauncey T, Forman SJ, Deeg HJ, et al. Cyclophosphamide and antithymocyte globulin to condition patients with aplastic anemia for allogeneic marrow transplantations: the experience in four centers. Biology of Blood and Marrow Transplantation. 2001 Jan 1;7(1):39-45.
33. Schleuning M, Günther W, Tischer J, Ledderose G, Kolb HJ. Dose-dependent effects of in vivo antithymocyte globulin during conditioning for allogeneic bone marrow transplantation from unrelated donors in patients with chronic phase CML. Bone Marrow Transplantation. 2003 Aug;32(3):243-50.
34. Chakraverty R, Orti G, Roughton M, Shen J, Fielding A, Kottaridis P, et al. Impact of in vivo alemtuzumab dose before reduced intensity conditioning and HLA-identical sibling stem cell transplantation: pharmacokinetics, GVHD, and immune reconstitution. Blood, The Journal of the American Society of Hematology. 2010 Oct 21;116(16):3080-8.
35. Jedlickova Z, Schmid C, Koenecke C, Hertenstein B, Baurmann H, Schwerdtfeger R, et al. Long-term results of adjuvant donor lymphocyte transfusion in AML after allogeneic stem cell transplantation. Bone Marrow Transplantation. 2016 May;51(5):663-7.
36. Weller JF, Mezger M, Seifert LL, Vogel W, Schneidawind D, Faul C, et al. Time dependent analysis of adoptive immunotherapy following sequential FLAMSA reduced intensity conditioning and allogeneic hematopoietic stem cell transplantation in patients with high-risk myeloid neoplasia. European Journal of Haematology. 2021 Dec 11.
37. Eefting M, de Wreede LC, Halkes CJ, von dem Borne PA, Kersting S, Marijt EW, et al. Multi-state analysis illustrates treatment success after stem cell transplantation for acute myeloid leukemia followed by donor lymphocyte infusion. Haematologica. 2016 Apr;101(4):506-14.
38. Schmid C, Schleuning M, Aschan J, Ringden O, Hahn J, Holler E, et al. Low-dose ARAC, donor cells, and GM-CSF for treatment of recurrent acute myeloid leukemia after allogeneic stem cell transplantation. Leukemia. 2004 Aug;18(8):1430-33.
39. Schroeder T, Rachlis E, Bug G, Stelljes M, Klein S, Steckel NK, et al. Treatment of acute myeloid leukemia or myelodysplastic syndrome relapse after allogeneic stem cell transplantation with azacitidine and donor lymphocyte infusions—a retrospective multicenter analysis from the German Cooperative Transplant Study Group. Biology of Blood and Marrow Transplantation. 2015 Apr 1;21(4):653-60.
40. Schmetzer HM, Kremser A, Loibl J, Kroell T, Kolb HJ. Quantification of ex vivo generated dendritic cells (DC) and leukemia-derived DC contributes to estimate the quality of DC, to detect optimal DC-generating methods or to optimize DC-mediated T-cell-activation-procedures ex vivo or in vivo. Leukemia. 2007 Jun;21(6):1338-41.
41. Mohty M, Malard F, Blaise D, Milpied N, Socie G, Huynh A, et al. Sequential regimen of clofarabine, cytarabine and reduced intensity conditioning (RIC) prior to allogeneic stem cell transplantation (allo-SCT) for acute myeloid leukemia (AML) in primary treatment failure. Blood. 2014;124(21).
42. Lancet JE, Uy GL, Cortes JE, Newell LF, Lin TL, Ritchie EK, et al. CPX-351 (cytarabine and daunorubicin) liposome for injection versus conventional cytarabine plus daunorubicin in older patients with newly diagnosed secondary acute myeloid leukemia. Journal of Clinical Oncology. 2018 Sep 10;36(26):2684-92.
43. Smith CC. The growing landscape of FLT3 inhibition in AML. Hematology 2014, the American Society of Hematology Education Program Book. 2019 Dec 6;2019(1):539-47.
44. Daigle SR, Choe S, Quek L, DiNardo CD, Stein A, Stein EM, et al. High rate of IDH1 mutation clearance and measurable residual disease negativity in patients with IDH1-mutant newly diagnosed acute myeloid leukemia treated with ivosidenib (AG-120) and azacitidine. Blood abstr. 2019;134:2706-2706.
45. DiNardo CD, Schuh AC, Stein EM, Fernandez PM, Wei A, De Botton S, et al. Enasidenib plus azacitidine significantly improves complete remission and overall response compared with azacitidine alone in patients with newly diagnosed acute myeloid leukemia (AML) with isocitrate dehydrogenase 2 (IDH2) mutations: interim phase II results from an ongoing, randomized study. Blood abstr. 2019;134:643-643.
46. Pan R, Hogdal LJ, Benito JM, Bucci D, Han L, Borthakur G, et al. Selective BCL-2 inhibition by ABT-199 causes on-target cell death in acute myeloid leukemia. Cancer Discovery. 2014 Mar 1;4(3):362-75.
47. Craddock C, Labopin M, Robin M, Finke J, Chevallier P, Yakoub-Agha I, et al. Clinical activity of azacitidine in patients who relapse after allogeneic stem cell transplantation for acute myeloid leukemia. Haematologica. 2016 Jul;101(7):879-83.
48. DiNardo CD, Maiti A, Rausch CR, Pemmaraju N, Naqvi K, Daver NG, et al. 10-day decitabine with venetoclax for newly diagnosed intensive chemotherapy ineligible, and relapsed or refractory acute myeloid leukaemia: a single-centre, phase 2 trial. The Lancet Haematology. 2020 Oct 1;7(10):e724-36.
49. Bug G, Burchert A, Wagner EM, Kröger N, Berg T, Güller S, et al. Phase I/II study of the deacetylase inhibitor panobinostat after allogeneic stem cell transplantation in patients with high-risk MDS or AML (PANOBEST trial). Leukemia. 2017 Nov;31(11):2523-5.
50. José-Enériz S, Gimenez-Camino N, Agirre X, Prosper F. HDAC inhibitors in acute myeloid leukemia. Cancers. 2019 Nov;11(11):1794.
51. Saure C, Schroeder T, Zohren F, Groten A, Bruns I, Czibere A, et al. Upfront allogeneic blood stem cell transplantation for patients with high-risk myelodysplastic syndrome or secondary acute myeloid leukemia using a FLAMSA-based high-dose sequential conditioning regimen. Biology of Blood and Marrow Transplantation. 2012 Mar 1;18(3):466-72.
52. Anderlini P, Wu J, Gersten I, Ewell M, Tolar J, Antin JH, et al. Cyclophosphamide conditioning in patients with severe aplastic anaemia given unrelated marrow transplantation: a phase 1–2 dose de-escalation study. The Lancet Haematology. 2015 Sep 1;2(9):e367-75.
53. George BM, Kao KS, Kwon HS, Velasco BJ, Poyser J, Chen A, et al. Antibody conditioning enables MHC-mismatched hematopoietic stem cell transplants and organ graft tolerance. Cell Stem Cell. 2019 Aug 1;25(2):185-92.
54. Gyurkocza B, Nath R, Choe H, Seropian S, Stiff PJ, Abhyankar S, et al. Personalized Targeted Radioimmunotherapy with Anti-CD45 Iodine (131I) Apamistamab [Iomab-B] in Patients with Active Relapsed or Refractory Acute Myeloid Leukemia Results in Successful Donor Hematopoietic Cells Engraftment with the Timing of Engraftment Not Related to the Radiation Dose Delivered. Blood. 2020 Nov 5;136:42-4.
55. Burchert A, Bug G, Fritz LV, Finke J, Stelljes M, Röllig C, et al. Sorafenib maintenance after allogeneic hematopoietic stem cell transplantation for acute myeloid leukemia with FLT3–internal tandem duplication mutation (SORMAIN). Journal of Clinical Oncology. 2020 Sep 10;38(26):2993-3002.
56. Ruggeri L, Capanni M, Urbani E, Perruccio K, Shlomchik WD, Tosti A, et al. Effectiveness of donor natural killer cell alloreactivity in mismatched hematopoietic transplants. Science. 2002 Mar 15;295(5562):2097-100.
57. Biavati L, Noonan K, Luznik L, Borrello I. Activated allogeneic donor-derived marrow-infiltrating lymphocytes display measurable in vitro antitumor activity. Journal of Immunotherapy. 2019 Apr 1;42(3):73-80.
58. Lulla PD, Naik S, Vasileiou S, Tzannou I, Watanabe A, Kuvalekar M, et al. Clinical effects of administering leukemia-specific donor T cells to patients with AML/MDS after allogeneic transplant. Blood, The Journal of the American Society of Hematology. 2021 May 13;137(19):2585-97.
59. Chapuis AG, Egan DN, Bar M, Schmitt TM, McAfee MS, Paulson KG, et al. T cell receptor gene therapy targeting WT1 prevents acute myeloid leukemia relapse post-transplant. Nature Medicine. 2019 Jul;25(7):1064-72.
60. Hirn Lopez A, Deen D, Fischer Z, Rabe A, Ansprenger C, Stein K, et al. Role of interferon (IFN) α in “Cocktails” for the generation of (Leukemia-derived) dendritic cells (DCleu) from blasts in blood from patients (pts) with acute myeloid leukemia (AML) and the Induction of antileukemic reactions. Journal of Immunotherapy. 2019 Jun 1;42(5):143-61.
61. Woiciechowsky A, Regn S, Kolb HJ, Roskrow M. Leukemic dendritic cells generated in the presence of FLT3 ligand have the capacity to stimulate an autologous leukemia-specific cytotoxic T cell response from patients with acute myeloid leukemia. Leukemia. 2001 Feb;15(2):246-55.
62. Dear AE. Epigenetic modulators and the new immunotherapies. New England Journal of Medicine. 2016 Feb 18;374(7):684-6.
63. Mathew NR, Baumgartner F, Braun L, O'Sullivan D, Thomas S, Waterhouse M, et al. Sorafenib promotes graft-versus-leukemia activity in mice and humans through IL-15 production in FLT3-ITD-mutant leukemia cells. Nature medicine. 2018 Mar;24(3):282-91.
64. Greiner J, Ono Y, Hofmann S, Schmitt A, Mehring E, Götz M, et al. Mutated regions of nucleophosmin 1 elicit both CD4+ and CD8+ T-cell responses in patients with acute myeloid leukemia. Blood, The Journal of the American Society of Hematology. 2012 Aug 9;120(6):1282-9.
65. Graf C, Heidel F, Tenzer S, Radsak MP, Solem FK, Britten CM, et al. A neoepitope generated by an FLT3 internal tandem duplication (FLT3-ITD) is recognized by leukemia-reactive autologous CD8+ T cells. Blood. 2007 Apr 1;109(7):2985-8.
66. Strønen E, Toebes M, Kelderman S, Van Buuren MM, Yang W, Van Rooij N, et al. Targeting of cancer neoantigens with donor-derived T cell receptor repertoires. Science. 2016 Jun 10;352(6291):1337-41.
67. Uy GL, Aldoss I, Foster MC, Sayre PH, Wieduwilt MJ, Advani AS, et al. Flotetuzumab as salvage immunotherapy for refractory acute myeloid leukemia. Blood, The Journal of the American Society of Hematology. 2021 Feb 11;137(6):751-62.
68. He X, Feng Z, Ma J, Ling S, Cao Y, Gurung B, et al. Bispecific and split CAR T cells targeting CD13 and TIM3 eradicate acute myeloid leukemia. Blood. 2020 Mar 5;135(10):713-23.
69. Depil S, Duchateau P, Grupp SA, Mufti G, Poirot L. ‘Off-the-shelf’allogeneic CAR T cells: development and challenges. Nature reviews Drug discovery. 2020 Mar;19(3):185-99.
70. Decroocq J, Itzykson R, Vigouroux S, Michallet M, Yakoub-Agha I, Huynh A, et al. Similar outcome of allogeneic stem cell transplantation after myeloablative and sequential conditioning regimen in patients with refractory or relapsed acute myeloid leukemia: A study from the Société Francophone de Greffe de Moelle et de Thérapie Cellulaire. American Journal of Hematology. 2018 Mar;93(3):416-423.