Abstract
Introduction: Cervical disc herniation (CDH) can produce severe radiculopathy and functional impairment, and management becomes more complex when neurological comorbidities such as multiple sclerosis (MS) are present. This case study reports on a 35-year-old female with CDH at C5–C6 with a concurrent demyelinating MS lesion at the same level, who presented with debilitating cervical pain, marked left upper-extremity weakness (3/5 strength), sensory loss, absent reflexes, and significant activity limitations.
Methods: Non-surgical spinal decompression using the DRX9000C was selected to avoid elevated surgical risk and potential MS exacerbation. The patient completed 20 decompression sessions over 15 weeks, using robotically controlled intermittent traction targeted at C5–C6.
Results: By the fifth treatment, she reported full resolution of pain and complete return to activities of daily living. Post-treatment examination demonstrated restored strength (5/5), normalized sensation, and symmetrical reflexes, with the Neck Disability Index improving from 36/50 to 1/50. MRI revealed reductions in lesion size (AP length decreased 1.67 mm; SI length decreased 1.27 mm), increased spinal canal diameter (+3.15 mm), and increased left foraminal space (+0.81 mm). At 1-year follow-up, neurological function remained normal, Neck Disability Index measured 0/50, and imaging showed sustained or continued improvements without recurrence of symptoms or worsening of MS.
Conclusion: This case highlights the longitudinal effects, as well as the potential benefits and safety, of targeted cervical non-surgical spinal decompression using the DRX9000C for CDH in the presence of MS. Findings support its role as a viable non-surgical intervention for CDH.
Keywords
Cervical disc lesion, Traction, Non-surgical spinal decompression, Neck pain, Cervical intervertebral disc, Conservative therapy, Case study
Introduction
Cervical disc herniation (CDH) is a clinically significant spinal disorder, most commonly affecting individuals between the ages of 30 and 50 [1,2]. While both sexes are affected, epidemiological data suggest a higher prevalence among females, accounting for approximately 60% of cases [1], in contrast to lumbar disc herniation which shows a male predominance with a 2:1 male-to-female ratio [3]. The clinical presentation of CDH varies depending on the location and degree of neural compression, with severe cases manifesting as debilitating cervical and upper thoracic pain, radiculopathy, and functional impairment of the ipsilateral upper extremity [1,2].
Although surgical intervention such as anterior cervical discectomy and fusion (ACDF) remains a common recommendation for symptomatic patients, it carries risks of neurological injury, infection, and adjacent segment degeneration [4,5]. In patients with comorbid neurological conditions, particularly MS, surgical risk may be further compounded. MS is a chronic autoimmune demyelinating disease of the central nervous system. While it does not directly cause disc herniation, MS-related neuromuscular dysfunction and postural adaptations may predispose patients to accelerated degenerative changes within the spine [6].
As an alternative to invasive procedures, non-surgical spinal decompression therapy has emerged as a viable conservative treatment for cervical disc pathology [1,7,8]. The DRX9000C, a computer-assisted spinal decompression system, has demonstrated promising outcomes in the management of discogenic pain, with reports suggesting a success rate of up to 90.5% in reducing pain, retracting herniated discs, and improving functional status in selected patient populations [9,10].
This case study presents the clinical application of cervical spinal decompression using the DRX9000C in a patient with coexisting CDH and a demyelinating MS lesion at the same cervical segment. It aims to assess the therapeutic benefit, safety considerations, and potential role of non-invasive decompression therapy in the management of spinal pathology within a neurologically complex patient.
Case Presentation
This case study was approved by the University of South Florida Internal Review Board (STUDY004354). The patient provided informed consent for her case to be published. The patient is a 35-year-old moderately athletic female who is a full-time student and regularly exercises at the gym five days per week. The mechanism of injury occurred while lifting a 30-pound ball over her left shoulder, during which her cervical spine was rotated to the right with right lateral flexion. She experienced an immediate sharp pain in the cervical region at the time of injury. Over the following days, the pain progressed and evolved into a burning, aching, and stabbing sensation rated at 5/10 on the verbal numeric rating scale (VNRS). The pain distribution included the left upper trapezius, left rhomboids, left deltoid tuberosity, left biceps, and left posterior cervical region. Her symptoms continued to intensify, reaching a 9/10 VNRS, accompanied by visible muscle atrophy and a significant decrease in muscle strength across all the aforementioned muscle groups, preventing her from participating in daily life activities. At the time of presentation, the patient was not experiencing any symptoms related to their previous MS diagnosis and was not taking any medications due to personal choice.
Physical Exam Findings – Pre-Intervention
Patient states that she is unable to sit up without causing pain. The Neck Disability Index patient reported outcome scored a 36/50, demonstrating complete/ total disability [11]. Strength testing revealed the following on the Medical Research Council Scale for Muscle Strength [12]: left Deltoid 3/5, left Tricep 3/5, left Bicep 3/5, left Finger Flexors 3/5, left Shoulder Depressors 3/5, right Deltoid 5/5, right Tricep 5/5, right Bicep 5/5, right Finger Flexors 5/5, and right Shoulder Depressors 5/5. Dermatome testing demonstrated decreased sensation in the entire left arm (C5-T1), specifically the radial and triceps regions. Reflexes demonstrated an absent C5 brachioradialis on the left with a 2+ on the right, absent C6 biceps reflex on the left with a 2+ on the right; and an absent C7 triceps reflex on the left with a 2+ on the right. The patient expressed a history of burning/ stabbing pain with progressive left-sided muscular weakness and muscle atrophy correlating strongly with C6 nerve root compression. In addition, the C5–C6 dermatomes were affected. MRI imaging was ordered and the imaging confirmed C4–C5, C5–C6, and C6–C7 disc lesions, with the most aggressive lesion at C5–C6 on the left side.
Method of Treatment/ Intervention
This patient was treated with the DRX9000C cervical decompression system. The DRX9000C is a non-surgical spinal decompression device that is used to alleviate pressure on the spine. The DRX9000C has received clearance from the FDA to be used in the treatment of herniated discs, bulging discs, degenerative disc disease, and posterior facet syndrome. This device allows for the targeted treatment of a cervical spine level depending on patient presentation and imaging findings. In this case study, the patient was treated at the C5–C6 level which corresponds to a treatment angle of 13°. The DRX9000C comes with a touch screen computer where the provider is able to input treatment parameters unique to each patient. The provider can select the target treatment level (e.g., C5–C6, C2–C3) based on the patient’s clinical presentation, and the DRX9000C automatically adjusts the angle of pull to target the chosen segment. In addition, the traction force can be modified to optimize patient comfort and determine the most appropriate therapeutic load. The device comes with 4 different cervical headpiece sizes that provide up to 3.5 inches of travel. A pillow is placed under the knees for comfort while the patient is in a supine position to start treatment. The DRX9000C uses a robotically controlled, intermittent traction force to decompress the intervertebral segments. The intermittent traction force uses a logarithmic cycle to repeatedly stretch and decompress the spine while maintaining a negative-pressure environment (Figure 1). Although baseline tension is sustained throughout the treatment, the force is periodically increased to create a pumping effect on the intervertebral discs. This intermittent loading is thought to produce negative pressure within the disc, potentially reducing herniation and facilitating disc rehydration [13].
Figure 1. Logarithmic curve of DRX9000. The figure illustrates (top) the logarithmic loading profile, (middle) the measured patient load, and (bottom) the variance between the two. The red line denotes the current time point within the loading cycle. By quantifying the variance between the prescribed and measured loads, the system adjusts its loading characteristics to ensure accurate force delivery. The transition from minimum to maximum force follows a logarithmic progression.
The patient in this case study underwent 20 treatment sessions of 28 minutes and 15 seconds in length that included 18 cycles of intermittent traction (60 seconds maximum pull followed by 30 seconds of minimum pull). The force was applied using a logarithmic curve with details listed in Table 1. The treatment angle for every visit was 13° to target the C5–C6 level. The profile selection describes the rate of ramp up to the maximum load. Profile 1 consists of the following parameters for the first 8 cycles (¼, ¼, ½, ½, ½, ¾, ¾, ¾ of Max Load). The remaining 10 cycles are alternated between the max and min load listed above. Profile 2 consists of the following for the first 5 cycles (¼. ½, ½, ¾, ¾) before ramping up to the full load for the remaining 13 cycles. Profile 5 consists of ramping up to the maximum load for all 18 cycles. At visit 1, Profile 1 was used. At visit 2, Profile 2 was used. At the 3rd visit and beyond, Profile 5 was used. Profiles 3 and 4 are also provided by the manufacturer but were not used in this case. The use of these profiles enables the provider to tailor loading characteristics to enhance patient comfort, particularly during the initial treatment sessions.
|
Force and Angle Applied to the Cervical Spine at Each Session |
||||
|
Visit Number |
Max Load (lbs) |
Min Load (lbs) |
Treatment Angle (°) |
Profile |
|
1 |
7 |
5 |
13 |
Profile 1 |
|
2 |
7 |
5 |
13 |
Profile 2 |
|
3-4 |
8 |
5 |
13 |
Profile 5 |
|
5 |
9 |
5 |
13 |
Profile 5 |
|
6 |
10 |
5 |
13 |
Profile 5 |
|
7 |
12 |
5 |
13 |
Profile 5 |
|
8-9 |
12 |
6 |
13 |
Profile 5 |
|
10-20 |
13 |
6 |
13 |
Profile 5 |
During the 15 weeks of treatment, the patient was restricted from undergoing any other treatments such as chiropractic treatment or physical therapy to isolate the effects of non-surgical spinal decompression. Additionally, the patient was not allowed to return to normal workouts until after completion of the 20 DRX sessions. Furthermore, the patient did not take any prescription medications during the treatment or during the 1 year follow-up period; the patient was allowed to continue to take vitamin and nutritional supplements that they took before undergoing treatment. The outcomes detailed below include the physical exam and MRI findings before undergoing treatment and then after the 20 sessions of treatment had occurred. A 1-year follow-up is also included to demonstrate the long-term benefit of the DRX treatment. The patient did not undergo any additional treatments on the DRX or use any other therapies during the 1-year follow-up period.
Results of the Intervention
After the 5th treatment (~2.5 weeks), the patient reported that their radicular symptoms had disappeared and all ADLs had returned to normal. The patient indicated that they were now able to carry grocery bags with both arms without pain, which she was unable to do before. Even with the positive outcome early on, the patient continued to complete 20 visits in accordance with the clinical standard of care.
Physical Exam Findings – Post-Intervention
As stated prior, the patient had lack of symptoms by the 5th DRX visit. Pain was 0/10 on the VPRS. The Neck Disability Index patient reported outcome scored a 1/50, demonstrating no disability [11]. Strength testing revealed 5/5 in all muscle groups and equal bilaterally. Dermatome testing demonstrated all sensations intact bilaterally (C5-T1). Reflexes were 2+ bilaterally for the C5, C6, and C7 reflexes.
At the 1-year follow up physical examination, all strength testing continued to be 5/5 in all muscle groups and equal bilaterally. Additionally, sensation remained fully intact in all dermatomes and reflexes were 2+ bilaterally. Sensation remained fully intact and the C5, C6, and C7 reflexes were 2+ bilaterally. The Neck Disability Index score a 0/50, denoting no disability.
MRI Measurements
All MRI imaging obtained was assessed with Weasis DICOM Viewer (v4.6.6) and was assessed longitudinally (Figure 2) [14]. Following non-surgical spinal decompression treatment of the cervical spine, the anterior-posterior (AP) length of the lesion at C5–C6 decreased (Figures 3A and 3B) from 5.45 mm to 3.78 mm (-1.67 mm; 31% decrease) and the superior-inferior (SI) length of the lesion decreased from 10.27 mm to 9.00 mm (-1.27mm; 12% decrease; Figures 3A and 3B). After 1-year follow up, the AP length decreased by an additional 0.25 mm resulting in a total decrease of 1.92 mm (35% decrease); the SI length increased by 1.03mm at the 1-year follow-up resulting in an overall reduction of 0.24mm (10% decrease; Figures 3A and 3C).
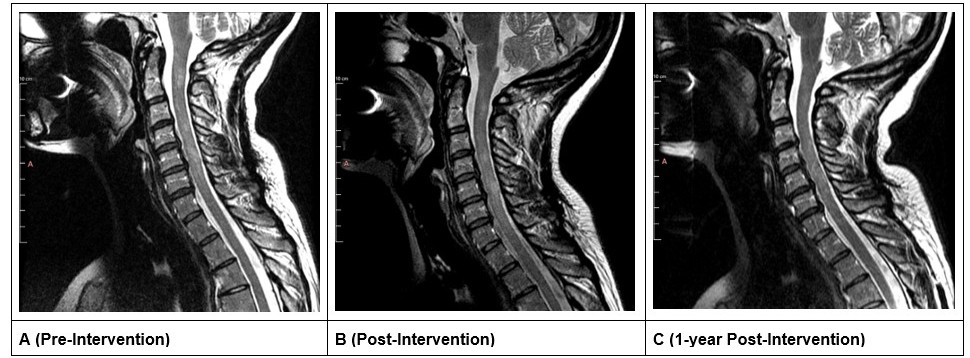
Figure 2. Mid-sagittal slice of the cervical MRI. A is before treatment, B is after treatment, and C is 1-year follow-up.
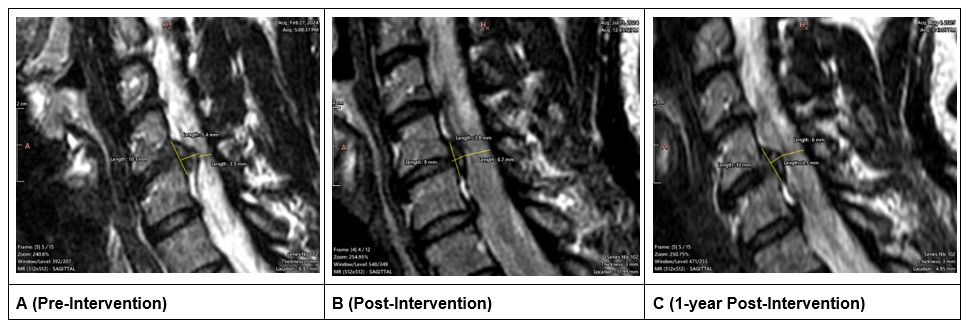
Figure 3. Para-sagittal slice of the left-sided disc lesion. The lesion present on the left side across all three time points. A (pre-treatment), B (post-treatment), C (1 year follow-up).
The AP dimension of the spinal canal at C5–C6 level increased from 3.55 mm to 6.70 mm (+3.15mm; 89% increase) after treatment (Figures 4A and 4B). At 1 year the AP dimension decreased by 0.72 mm resulting in an overall increase of 2.43 mm (68% increase; Figures 4A and 4C). The foraminal gap between the vertebrae and the disc at the C5–C6 level increased from 1.79 mm to 2.60 mm (+0.81 mm; 45% increase) on the left side (symptomatic side) and increased from 3.24 mm to 3.43 mm (+0.19 mm; 5% increase) on the right side (Figures 4A and 4B). At 1 year follow up, the foraminal gap on the left side decreased by 0.08 mm resulting in an overall increase of 0.73 mm (41% increase); on the right side, the foraminal gap increased by an additional 0.03 mm resulting in an overall increase of 0.22 mm (7% increase; Figures 4A and 4C).
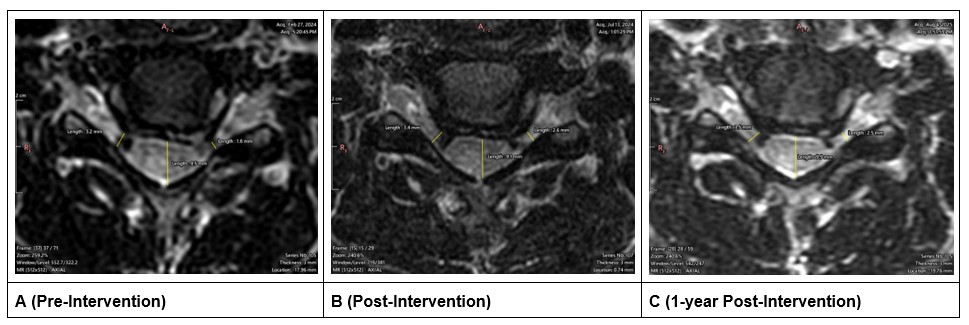
Figure 4. Axial MRI slices at the C5-C6 level. A is before treatment, B is after treatment, C is 1-year follow-up. These images also show the representative measurements of the left and right foraminal gap at its narrowest point.
The average disc height ([Anterior Disc Height + Middle Disc Height + Posterior Disc Height]/3) at the C5–C6 level increased from 3.61 mm before treatment to 3.66 mm after treatment (+0.05mm; 1% increase; Figures 5A and 5B). At 1 year follow-up, the disc height continued to increase an additional 0.12 mm resulting in an overall increase of 0.17 mm (5% increase; Figures 5A and 5C).
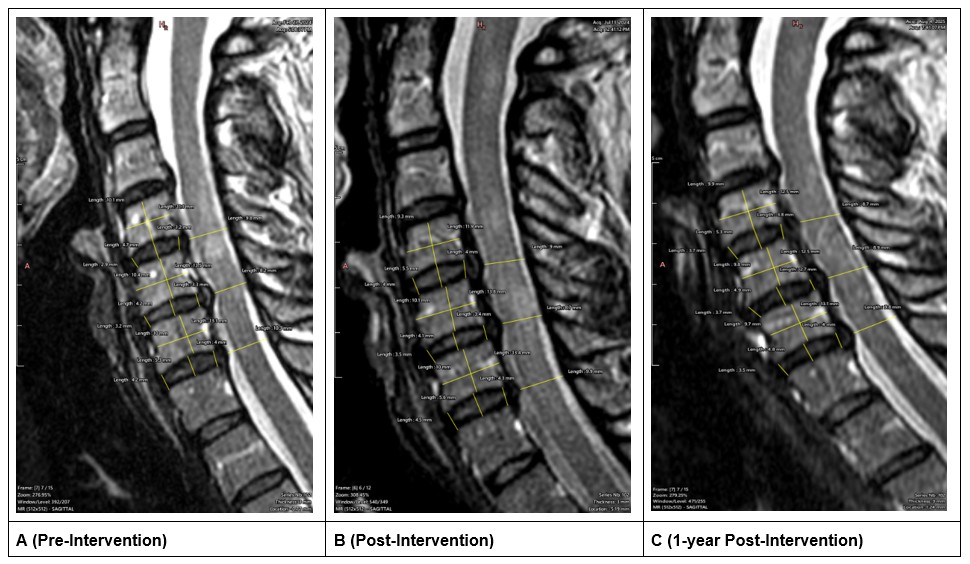
Figure 5. Longitudinal measurements of the mid-sagittal slices. A (pre-treatment), B (post-treatment), C (1 year follow-up).
The ratio of disc height to AP diameter of the overlying vertebrae at the C5–C6 level stayed consistent at 0.27 before treatment and 0.27 after treatment (Figures 5A and 5B). However, at 1-year follow-up, this ratio increased by 0.03 to a final value of 0.30 (11% increase; Figures 5A and 5C). Additionally, the ratio of disc height to height of the overlying vertebrate increased from 0.35 before treatment to 0.36 (3% increase) after treatment and 0.38 (9% increase) at 1 year follow-up. Additional measurements of the adjacent vertebral levels (C4–C5 and C6–C7) are provided in Table 2.
|
Pre |
Post |
1 Year Follow-Up |
Post - Pre |
1 Year - Post |
1 Year - Pre |
|||||||
|
Level |
C4–C5 |
C5–C6 |
C6–C7 |
C4–C5 |
C5–C6 |
C6–C7 |
C4–C5 |
C5–C6 |
C6–C7 |
C5–C6 |
C5–C6 |
C5–C6 |
|
Anterior Disc Height Mid Sag |
2.90 |
3.24 |
4.19 |
4.00 |
3.47 |
4.48 |
3.72 |
3.67 |
3.51 |
0.23 |
0.20 |
0.43 |
|
Mid Disc Height Mid Sag |
4.66 |
4.24 |
5.30 |
5.46 |
4.15 |
5.61 |
5.34 |
4.94 |
4.75 |
-0.09 |
0.79 |
0.70 |
|
Posterior Disc Height Mid Sag |
3.23 |
3.35 |
4.03 |
4.00 |
3.36 |
4.26 |
3.78 |
2.74 |
3.95 |
0.01 |
-0.62 |
-0.61 |
|
Average Disc Height |
3.60 |
3.61 |
4.51 |
4.49 |
3.66 |
4.78 |
4.28 |
3.78 |
4.07 |
0.05 |
0.12 |
0.17 |
|
AP Diameter of Overlying Vertebrae |
11.14 |
13.48 |
13.05 |
11.94 |
13.78 |
13.41 |
12.52 |
12.46 |
13.14 |
0.30 |
-1.32 |
-1.02 |
|
Height of Overlying Vertebrae |
10.14 |
10.42 |
10.01 |
9.32 |
10.08 |
9.97 |
9.86 |
9.84 |
9.67 |
-0.34 |
-0.24 |
-0.58 |
|
AP Canal Dimension Mid Sagittal |
9.76 |
8.22 |
10.30 |
8.98 |
8.73 |
9.85 |
8.74 |
8.87 |
9.81 |
0.51 |
0.14 |
0.65 |
|
Disc Height/AP Diameter of Vertebrae |
0.32 |
0.27 |
0.35 |
0.38 |
0.27 |
0.36 |
0.34 |
0.30 |
0.31 |
0.00 |
0.04 |
0.04 |
|
Disc Height/Height of Vertebrae |
0.35 |
0.35 |
0.45 |
0.48 |
0.36 |
0.48 |
0.43 |
0.38 |
0.42 |
0.02 |
0.02 |
0.04 |
|
Left Foraminal Gap |
4.23 |
1.79 |
4.70 |
3.50 |
2.60 |
5.41 |
2.60 |
2.52 |
4.23 |
0.81 |
-0.08 |
0.73 |
|
Right Foraminal Gap |
3.82 |
3.24 |
4.67 |
3.74 |
3.43 |
5.20 |
4.03 |
3.46 |
2.20 |
0.19 |
0.03 |
0.22 |
|
AP Canal Dimension at Lesion |
- |
3.55 |
- |
- |
6.70 |
- |
- |
5.98 |
- |
3.15 |
-0.72 |
2.43 |
|
Lesion AP Length |
- |
5.45 |
- |
- |
3.78 |
- |
- |
3.53 |
- |
-1.67 |
-0.25 |
-1.92 |
|
Lesion SI Length |
- |
10.27 |
- |
- |
9.00 |
- |
- |
10.03 |
- |
-1.27 |
1.03 |
-0.24 |
|
*All measurements in mm, Grey shaded boxes indicate the specified level of treatment (C5-C6) |
||||||||||||
Discussion
In this case study, the patient’s injury involved cervical right rotation and lateral flexion under load, a biomechanical mechanism that likely led to excessive intradiscal pressure and disc extrusion at C6. From the disc lesion, the patient experienced symptoms of burning, stabbing pain with progression to weakness and muscle atrophy correlated strongly with C6 nerve root compression, affecting the C5–C6 dermatome. MRI confirmed a disc extrusion at the C6 level, aligning with the patient’s neurological presentation and symptom distribution.
The DRX9000C spinal decompression system was used as a non-surgical intervention, applying targeted axial traction to reduce intradiscal pressure and facilitate retraction of the extruded disc material [13]. This decompression therapy is believed to enhance nutrient exchange within the disc, promoting healing and reducing neural impingement [15]. The DRX9000C is a robotically controlled (mechanical) traction device that differs from other forms of cervical traction, such as manual, aquatic, or gravitational methods [16]. Mechanical traction, as delivered by the DRX9000, allows for greater precision in treatment delivery and may offer enhanced safety compared to traditional traction approaches. The DRX9000 distinguishes itself from other intermittent cervical traction devices by its ability to provide real-time, quantifiable feedback on the applied force (Figure 1) and to allow precise adjustment for targeting specific vertebral levels. In addition, it utilizes a logarithmic loading curve, which sets it apart from more conventional loading patterns such as square or triangular waveforms. The subtle changing of the logarithmic curve is theorized to diminish the potential of muscular guarding that would inhibit the therapeutic decompression force.
From the intervention, the patient experienced a significant reduction in pain (from 9/10 to near 0/10), restored muscle strength, reversal of visible atrophy, and full return to daily gym activities. Clinical re-evaluation showed normalization of sensory and motor findings, with no residual neurological deficits at 1 year follow-up.
Although a spontaneous MS exacerbation cannot be entirely excluded, the described mechanism of injury – lifting a 30-pound ball over the left shoulder during cervical rotation and lateral flexion with immediate onset of sharp pain – more strongly supports an acute CDH. This conclusion is further supported by the physical examination, which demonstrated focal findings consistent with pathology at the level of the identified disc lesion. In patients with MS, careful differentiation between cervical disc pathology and MS-related symptom exacerbation is essential. A thorough physical examination, in conjunction with appropriate imaging, is critical to accurately identify the underlying pathology and inform treatment decisions. While cervical traction may theoretically pose a risk in this population due to forces applied to the spinal cord, there is currently limited evidence to either support or refute this concern.
This case illustrates the benefit of spinal decompression therapy for disc extrusion with neurological symptoms, offering a conservative alternative to surgical intervention. In addition, it demonstrates that an individual with a comorbidity of MS can similarly benefit from the conservative approach to a cervical disc lesion. Early identification of red flags such as progressive weakness and atrophy helped guide timely imaging and appropriate treatment. The case underscores the importance of detailed biomechanical assessment, advanced imaging, and non-invasive evidence-based management in optimizing outcomes for disc injuries. Additionally, the patient experienced no exacerbation to her MS symptoms and condition while undergoing the DRX9000C therapy.
Strengths/Limitations
A strength of this study is the long-term (1 year) follow-up with physical examination and advanced MRI imaging. This allowed for the determination of the longitudinal treatment effects for use of the DRX9000C. However, there were some limitations. As a case report, this single case is not generalizable to a broader population. Additionally, in this case presentation, there were multiple herniations at various levels of the cervical spine. C5–C6 was selected for treatment because it was the level with the largest lesion and also the level determined by physical examination as the level for treatment. Manual measurements of MRI images can be prone to error and bias. Measurements taken at the mid-sagittal region and at the level of the lesion may not represent exact anatomical locations due to differences in patient position in the MRI and differences in slice thickness and the distance between slices. However, care was taken to ensure the measurements were conducted at as close a planar slice as possible for the pre and post treatment scans. Although MRI is highly sensitive for detecting disc pathology, these findings do not always correlate with clinical outcomes [17]. Therefore, a comprehensive neurological examination is essential to fully understand the patient’s presentation.
Conclusion
This case study demonstrated successful use of the DRX9000C to treat CDH in an individual with a co-morbid neurological condition of MS. The patient experienced no exacerbation of their MS symptoms or condition while undergoing treatment. This case also demonstrates the longitudinal effectiveness of this treatment with inclusion of a 1-year follow-up in addition to the pre- and post-intervention measures. As a case study, additional research is warranted to determine causality and allow for generalization of these results to other individuals with CDH.
Conflicts of Interest
Author NDS has received industry, foundation, and federal grant funding for research with use of the DRX9000 technology. However, all funding allow for full academic freedom for manuscripts and presentation to report the results, whether positive or negative, for the outcomes of the DRX9000.
Funding Statement
This work was supported by the Florida Department of State Center for Neuromusculoskeletal Research.
References
2. Radhakrishnan K, Litchy WJ, O’Fallon WM, Kurland LT. Epidemiology of cervical radiculopathy. Brain 1994;117:325–35.
3. Jordan J, Konstantinou K, O’dowd J. Herniated lumbar disc. BMJ Clin Evid 2009.
4. Epstein NE. A review of complication rates for anterior cervical diskectomy and fusion (ACDF). Surg Neurol Int 2019;10.
5. Yee TJ, Swong K, Park P. Complications of anterior cervical spine surgery: A systematic review of the literature. Journal of Spine Surgery 2020;6:302–22.
6. Chhugani S, Agarwal N, Sheikh F, Borca F, Spanoulis A, Galea I. Cervical spinal degenerative disease in multiple sclerosis. Eur J Neurol 2021;28:2497–502.
7. Xu Q, Tian X, Bao X, Liu D, Zeng F, Sun Q. Nonsurgical spinal decompression system traction combined with electroacupuncture in the treatment of multi-segmental cervical disc herniation: A case report. Medicine (United States) 2022;101:E28540.
8. Ma SY, Kim HD. The effect of motorized spinal decompression delivered via spineMED combined with physical therapy modalities for patients with cervical radiculopathy. J Phys Ther Sci 2010;22:429–35.
9. Schueren S, Luginsland LA, Medina GA, Schilaty ND. Retrospective Chart Review of Nonsurgical Spinal Decompression as a Therapeutic Modality for Low Back Pain. Mil Med 2025;190:134–40.
10. Connolly JA, Luginsland LA, Welsh S, Bexley JA, Pirone J, Martin WR, et al. Clinical and Imaging Outcomes of Non-Surgical Spinal Decompression for Lumbar Intervertebral Disc Lesions: A Case Series. J Contemporary Chiropr 2025; 8:81–7.
11. Vernon H, Mior S. The Neck Disability Index: a study of reliability and validity. J Manipulative Physiol Ther 1991;14:409–15.
12. Compston A. Aids to the Investigation of Peripheral Nerve Injuries. Medical Research Council: Nerve Injuries Research Committee. His Majesty’s Stationery Office: 1942; pp. 48 (iii) and 74 figures and 7 diagrams; with Aids to the Examination of the Peripheral Nervous System. By Michael O’Brien for the Guarantors of Brain. Saunders Elsevier: 2010; pp. [8] 64 and 94 Figures. Brain 2010;133:2838–44.
13. Ramos G, Martin W. Effects of vertebral axial decompression on intradiscal pressure. J Neurosurg 1994;81:350–3.
14. Roduit N. Weasis DICOM Viewer 2025:Version 4.6.6. Available from: https://github.com/nroduit/Weasis (accessed February 22, 2026).
15. Kuo Y-W, Hsu Y-C, Chuang I-T, Chao P-HG, Wang J-L. Spinal Traction Promotes Molecular Transportation in a Simulated Degenerative Intervertebral Disc Model. Spine (Phila Pa 1976) 2014;39:E550–6.
16. Alrwaily M, Almutiri M, Schneider M. Assessment of variability in traction interventions for patients with low back pain: A systematic review. Chiropr Man Therap 2018;26:1–11.
17. Eldaya RW, Parsons MS, Hutchins TA, Avery R, Burns J, Griffith B, et al. ACR Appropriateness Criteria® Cervical Pain or Cervical Radiculopathy: 2024 Update. J Am Coll Radiol 2025;22:S136–62.