Abstract
This study aims to reveal some important insights into the different diagnoses that are listed in Medical Information Mart for Intensive Care (MIMIC) dataset. This dataset includes patients from diverse backgrounds, ethnicity, demographics, etc. The diagnosis records are stored electronically using ICD-09 and ICD-10 codes. It is found that most of the patients were diagnosed at least once for essential hypertension and other related diseases.
Keywords
MIMIC, ICU, Hypertension, Emergency Department, Data mining
Introduction
Since critical patients require constant monitoring, the intensive care unit (ICU) is a data-rich setting. Researchers are drawn to the ICU environment because of the often-acute nature of ICU patient sickness and the requirement of early intervention. There are a lot of publicly available critical care datasets that have enabled research in this domain, which is unique.
These initiatives are mostly based on MIMIC [1], and a waveform database including demographic information digitally transcribed from paper records for over 90 patients. MIMIC- IV v2.2 [2] and MIMIC-IV ED [3] have been investigated in this study.
MIMIC-IV originates from two in-hospital database systems: a customized hospital-wide Electronic Health Record (EHR) and a Clinical Information System specific to Intensive Care Units (ICUs). The development of MIMIC-IV involved a three-step process:
Acquisition: Data extraction was performed for patients admitted to the Beth Israel Deaconess Medical Center (BIDMC) emergency department or any of the intensive care units from the respective hospital databases. A comprehensive master patient list was established, encompassing all medical record numbers corresponding to ICU or emergency department admissions between 2008 and 2019. Source tables were then filtered to include only records related to patients in the master patient list [2].
Preparation: The data underwent reorganization to enhance retrospective data analysis. This involved denormalizing tables, removing audit traces, and restructuring into a more condensed set of tables. The primary objective of this procedure was to simplify retrospective analysis of the database. Notably, data cleaning procedures were intentionally omitted to maintain the representation of a real-world clinical dataset [2].
Deidentification: Patient identifiers, as mandated by the Health Insurance Portability and Accountability Act (HIPAA), were eliminated. Random ciphers were used to replace patient identifiers, resulting in deidentified integer identifiers for patients, hospitalizations, and ICU stays. Structured data underwent filtering using lookup tables and allow lists. If required, a free-text deidentification algorithm was applied to remove Personal Health Information (PHI) from free-text. Additionally, date and times were arbitrarily shifted into the future with an offset measured in days. Each patient ID (e.g., subject ID) was assigned a unique date shift, ensuring internal consistency for a single patient's data. For instance, if the time between two measures in the original data was 4 hours, the calculated time difference in MIMIC-IV would also be 4 hours. However, patients were not temporally comparable, meaning two patients hospitalized in 2130 were not necessarily admitted in the same year. Following these three stages, the database was exported to a character-based comma-delimited format.
MIMIC-IV-ED is a large, publicly accessible database of Beth Israel Deaconess Medical Center emergency department admissions from 2011 to 2019. In the database, there are 422,500 ED stays. Vital signs, triage information, medication reconciliation, medication delivery, and discharge diagnoses are accessible [3]. To comply with the Safe Harbor requirement of the Health Insurance Portability and Accountability Act (HIPAA), all data are deidentified. MIMIC-IV-ED is intended to facilitate a vast array of educational and research endeavors. Patients are evaluated and prioritized for further care in a congested emergency department (ED). The severity of the conditions of ED patients extends from minor cuts to potentially fatal heart conditions. The emergency department (ED) is, at its essence, a setting with limited resources in which the most valuable resource, human attention, is rationed to achieve positive patient outcomes. Recent advancements in algorithmic methods present a thrilling opportunity to improve emergency department care. Large datasets are required for data-driven studies, and open data access facilitates study replication. MIMIC-IV-ED, a large database of admissions to an ED at a Boston, Massachusetts academic medical center, is intended to facilitate data analysis in emergency care [3].
Background Studies
ICU stands for intensive care unit where many hypertensive patients are admitted. The combination of heart failure (HF) and hypertension is a leading cause of hospital mortality, particularly among intensive care unit (ICU) patients. However, under intensive work pressure, the large number of clinical signals generated in the ICU can easily overwhelm the medical staff, leading to treatment delays, suboptimal care, or even incorrect clinical decisions. Individual risk stratification is crucial for the management of ICU patients with HF and hypertension. Artificial intelligence, particularly machine learning (ML), can generate superior prognostic models for these patients [4].
Data Insights
Table 1 shows the number of patients who have been diagnosed at least once with specific ICD codes. It shows the first-time diagnosis that the patients received while they were admitted. Quite obviously, many of the patients have been diagnosed with different diseases throughout their follow-up period. But here, only the first-time diagnosis for patients is reported. Around 50,000 patients were diagnosed with unspecified essential hypertension at least once during their admission. Figure 1 shows an infographic of the same.
|
ICD code |
Long title |
Total patients |
|
4019 |
Unspecified essential hypertension |
49741 |
|
2724 |
Other and unspecified hyperlipidemia |
33448 |
|
I10 |
Essential (primary) hypertension |
31521 |
|
E785 |
Hyperlipidemia, unspecified |
27903 |
|
53081 |
Esophageal reflux |
23955 |
|
Z87891 |
Personal history of nicotine dependence |
21356 |
|
25000 |
Diabetes mellitus without mention of complication, type II or unspecified type, not stated as uncontrolled |
19401 |
|
311 |
Depressive disorder, not elsewhere classified |
19216 |
|
K219 |
Gastro-esophageal reflux disease without esophagitis |
19067 |
|
41401 |
Coronary atherosclerosis of native coronary artery |
17863 |
|
V1582 |
Personal history of tobacco use |
17849 |
|
5849 |
Acute kidney failure, unspecified |
17295 |
|
2859 |
Anemia, unspecified |
16592 |
|
F329 |
Major depressive disorder, single episode, unspecified |
16476 |
|
42731 |
Atrial fibrillation |
16454 |
|
4280 |
Congestive heart failure, unspecified |
14432 |
|
3051 |
Unspecified essential hypertension |
14343 |
|
F419 |
Other and unspecified hyperlipidemia |
14223 |
|
30000 |
Essential (primary) hypertension |
13705 |

Figure 1. Infographic of the top 20 diagnoses across patients.
Table 2 provides insights on the emergency department database (MIMIC-IV-ED). However, the diagnoses do not follow the diagnosis order of Table 1 except for a few. Hypertension takes the first place in both tables since there appears to be a highly disproportionate number of patients being diagnosed with it.
|
ICD code |
Long title |
Total patients |
|
4019 |
Unspecified essential hypertension |
18493 |
|
I10 |
Essential (primary) hypertension |
15410 |
|
R079 |
Chest pain, unspecified |
10499 |
|
78650 |
Chest pain, unspecified |
9515 |
|
R109 |
Unspecified abdominal pain |
8307 |
|
25000 |
Diabetes mellitus without mention of complication, type II or unspecified type, not stated as uncontrolled |
7591 |
|
78909 |
Abdominal pain, other specified site |
7174 |
|
W1830XA |
Fall on same level, unspecified, initial encounter |
7141 |
|
E8889 |
Unspecified fall |
6431 |
|
E119 |
Type 2 diabetes mellitus without complications |
6048 |
|
R51 |
Headache |
5908 |
|
R0600 |
Dyspnea, unspecified |
5812 |
|
2720 |
Pure hypercholesterolemia |
5721 |
|
5990 |
Urinary tract infection, site not specified |
5370 |
|
7840 |
Headache |
5191 |
|
R531 |
Weakness |
5164 |
|
R55 |
Syncope and collapse |
5149 |
|
R42 |
Dizziness and giddiness |
4959 |
|
R4182 |
Altered mental status, unspecified |
4773 |
|
N390 |
Urinary tract infection, site not specified |
4583 |
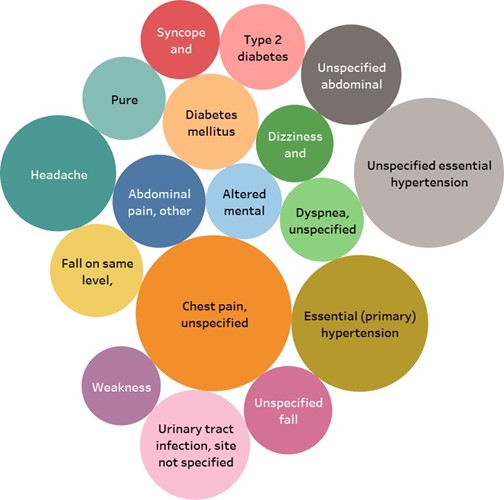
Figure 2. Infographic of t he top 20 diagnoses across ED patients.
Conclusion and Future Directions
This study reveals some insights into an ICU database that is widely used for research. Based on the findings, a disproportionate number of patients are associated with essential hypertension than other related diseases. There are many scopes to investigate hypertensive patients further like tracking the readmission rate, predicting mortality, vitals, etc.
MIMIC IV also contains many clinical notes where large language models can be implemented. Recent developments in scaling large language models (LLMs) have resulted in significant enhancements to several benchmarks for natural language processing [5]. These language models have been partially trained on clinical text. These studies demonstrate that training a language model with clinical notes using masked language modeling (MLM) is an effective method for improving performance on downstream tasks. All these previous works employ architectures with only decoders.
References
2. Johnson AE, Bulgarelli L, Shen L, Gayles A, Shammout A, Horng S, et al. MIMIC-IV, a freely accessible electronic health record dataset. Scientific Data. 2023 Jan 3;10(1):1.
3. Johnson A, Bulgarelli L, Pollard T, Celi LA, Mark R, Horng S. MIMIC-IV-ED (version 1.0). PhysioNet.
4. Peng S, Huang J, Liu X, Deng J, Sun C, Tang J, et al. Interpretable machine learning for 28-day all-cause in-hospital mortality prediction in critically ill patients with heart failure combined with hypertension: A retrospective cohort study based on medical information mart for intensive care database-IV and eICU databases. Frontiers in Cardiovascular Medicine. 2022 Oct 12; 9:994359.
5. Lehman E, Johnson A. Clinical-t5: Large language models built using mimic clinical text. PhysioNet.