Abstract
A patient with a unilateral congenital vitreous cyst attached to the posterior lens capsule is now described, with its photographic appearance.
Keywords
Vitreous cyst, Biomicroscopy, Congenital vitreous cyst
Introduction
Vitreous cysts are regarded as ‘ocular curiosities’ as they are rarely seen and reported [1]. They can be either congenital or acquired. Congenital vitreous cysts are usually isolated clinical findings and acquired cysts are observed in conditions like high myopia, ocular trauma, degenerative pathologies of the retina & choroid, and infections like Cysticercosis and Toxoplasmosis [2-4].
Case Report
A 46-year-old female presented with difficulty in reading for 1 year. The best corrected visual acuity for distance was 6/6 in both eyes (OU) and for near was N6 (OU) with +1D. Ocular pressures were 14 mmHg in both eyes.
Examination of the anterior segment revealed a small rounded, greyish-colored cyst in the anterior vitreous attached to the posterior lens capsule with a stalk (Figure 1 and 2). It moved with the movement of the eyeball and became stationary when the eyeball stopped moving. There was local liquefaction of the vitreous in the area navigated by the cyst during its movement.
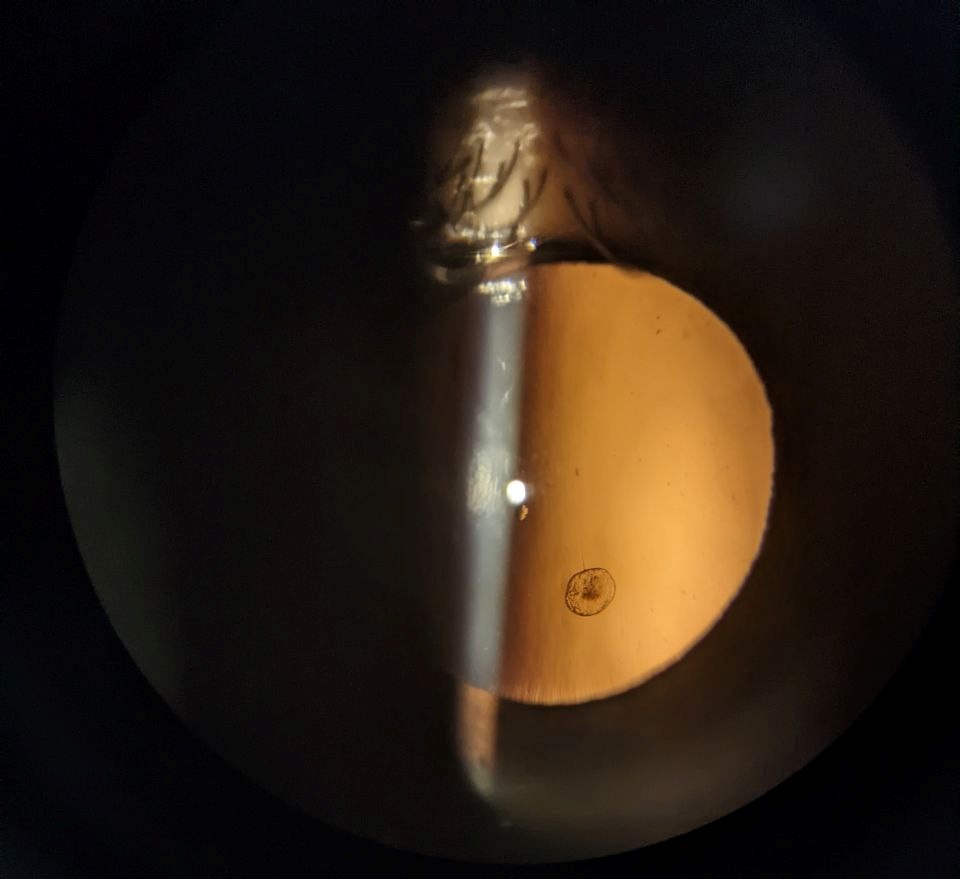
Figure 1. The cyst appears centrally opaque with retro-illumination, a very thin stalk attached to the cyst can be seen.
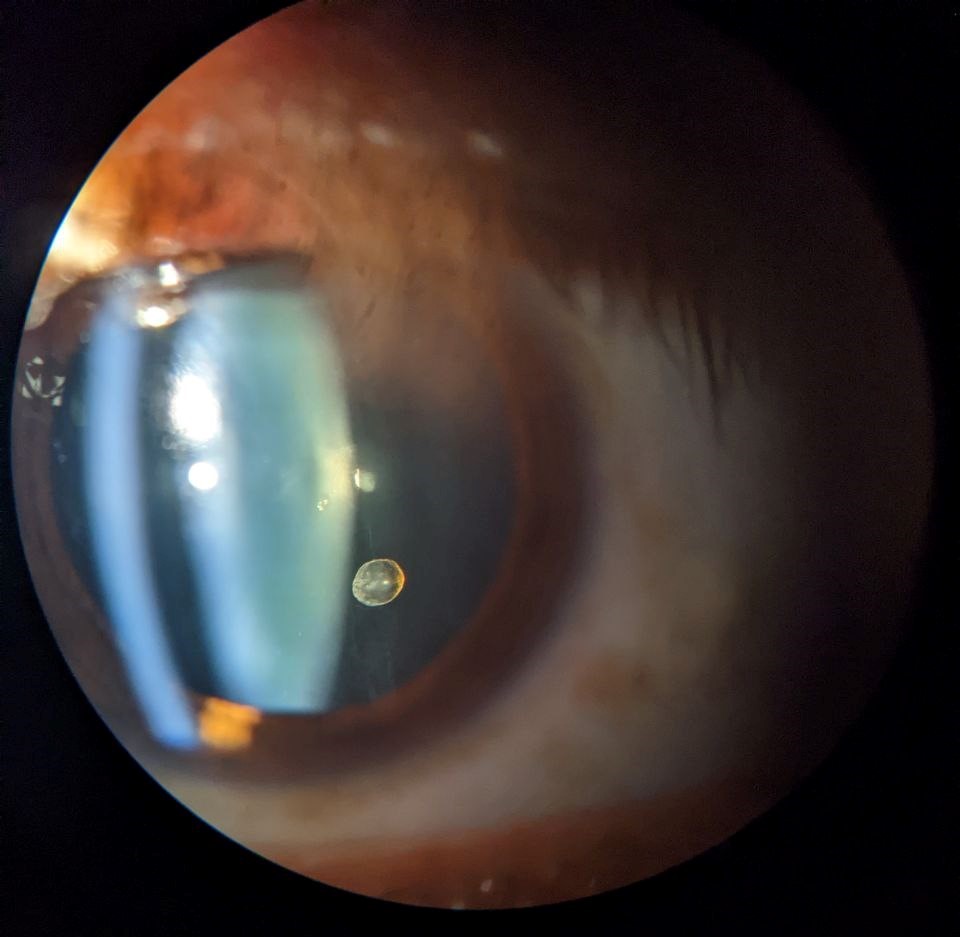
Figure 2. Slit-lamp photograph of the vitreous cyst behind the lens attached with a thin stalk.
Ultrasound biomicroscopy (UBM) showed echo reflections from the anterior and posterior surface of the cyst encompassing an anechoic area in between. The size of the cyst (0.63 mm) and the length of the stalk (0.48 mm) were measured on UBM (Figure 3). No other mass or cyst was noted in the iris or the ciliary body.
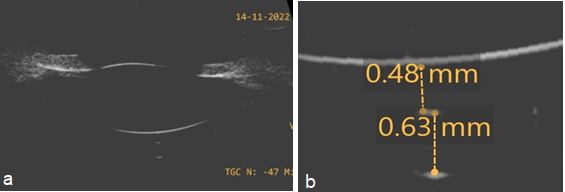
Figure 3. a) UBM shows a vitreous cyst with hyperechogenic walls and an acoustically hollow interior. No scolex seen. Suggestive of a primary vitreous cyst. b) shows measurement of stalk (0.48 mm) and cyst diameter (0.63 mm).
B-Scan did not show the cyst wall reflectivity due to its anterior proximity and no other cyst in the posterior vitreous or orbit was seen. Non-contrast CT of the brain and orbit ruled out intracranial cysticercosis. Blood serology tests were negative for Toxoplasma gondii, Toxocara canis, cysticercosis, and Echinococcus.
The patient was diagnosed as a case of congenital vitreous cyst and was observed for six months. No change in clinical appearance was noted.
Discussion
Congenital vitreous cysts are usually benign, asymptomatic, and non-progressive in nature. Histopathological findings of Nork and Millecchia [5] on non-pigmented grey cyst, suggest that the cyst is a choristoma of the primary hyaloid vessels. Orellana et al. [6] studied pigmented cysts and observed that the pigmented layer of cuboidal cells contains mature melanosomes and some immature melanosomes, suggesting that the pigmented cyst originates from the pigment epithelium.
Congenital cysts are of little clinical importance, but their grey opaque clinical appearance might resemble cysticercosis [7] or it may be confused with malignant melanoma [2] due to its pigmented appearance. Hence serological and radiological investigations need to be done to rule out other serious conditions.
In our case, the absence of signs of ocular inflammation and unremarkable ocular and systemic history ruled out acquired causes. Further, the retrolental attachment of the cyst suggests its origin to be a remnant of the hyaloid tissue.
Cysts of this type have been reported by Purper [8], who observed a "clearly visible" thread leading from the cyst to the posterior margin of the lens or possibly to the ciliary body and the cyst was multiloculated with glistening yellow spots on the surface with clearly visible lightly pigmented septa.
To the best of our knowledge, our case displays the first clinical photograph of a vitreous cyst attached to the lens.
As far as management is concerned, asymptomatic cysts do not require treatment. However, Pars plana vitrectomy, Laser cystotomy by Argon laser, or Nd: Yag laser have been done for symptomatic cases [6,9].
Conclusion
Congenital vitreous cysts are of little clinical significance, but they need to be differentiated from acquired cysts and from other serious conditions that mimic its appearance.
Conflicts of Interest
No conflicts of interest.
Funding Statement
No funding received.
References
2. Tuncer S, Bayramoglu S. Pigmented free-floating vitreous cyst in a patient with high myopia and uveal coloboma simulating choroidal melanoma. Ophthalmic Surgery, Lasers and Imaging Retina. 2011 Apr 14;42(6):e49-52.
3. Tranos PG, Ferrante P, Pavesio C. Posterior vitreous cyst and intermediate uveitis. Eye. 2010 Jun;24(6):1115-6.
4. Pannarale C. On a case of preretinal mobile cysts in a subject affected by congenital toxoplasmosis. Giornale Italiano Di Oftalmologia. 1964;17(5):306-17.
5. Nork TM, Millecchia LL. Treatment and histopathology of a congenital vitreous cyst. Ophthalmology. 1998 May 1;105(5):825-30.
6. Orellana J, O'Malley RE, McPherson AR, Font RL. Pigmented free-floating vitreous cysts in two young adults: electron microscopic observations. Ophthalmology. 1985 Feb 1;92(2):297-302.
7. Wood TR, Binder PS. Intravitreal and intracameral cysticercosis. Annals of Ophthalmology. 1979 Jul 1;11(7):1033-6.
8. Purper H. A rare condition of the vitreous body. Klin Monatsbl Augenheilkd. 1950;116:85-86.
9. Jones WL. Free-floating vitreous cyst. Optometry and Vision Science. 1998 Mar 1;75(3):171-3.