Abstract
The rapid advancement of Artificial Intelligence (AI) and intelligent digital systems has created significant opportunities to enhance clinical decision-making and data management within healthcare infrastructures. Electronic Health Record (EHR) platforms, while widely adopted, often struggle with issues related to data overload, inefficient triage, and limited real-time prioritization challenges that are particularly pronounced in resource-constrained healthcare environments such as Bangladesh. This study presents the design and development of an AI-enabled EHR prototype that integrates a priority-based patient management algorithm, real-time data processing, and modular analytics workflows. The system architecture incorporates structured preprocessing, severity-classification logic, and rule-based decision layers implemented using KNIME for data analytics and C# for application development. Quantitative evaluations were conducted to assess improvements in queue management, task scheduling efficiency, and physician usability, demonstrating measurable enhancements compared with conventional manual triage approaches. The findings illustrate the potential of AI-assisted EHR systems to strengthen operational efficiency and clinical responsiveness, providing a scalable pathway for digital healthcare transformation in developing countries.
Keywords
Artificial Intelligence (AI), Biomedical Engineering (BME), Deep Learning (DL), Data Fusion, Data Management System, Electronical Health Records (EHR), Machine Learning (ML)
Introduction
Electronic Health Record (EHR) systems have become a cornerstone of modern healthcare, enabling the digital storage, retrieval, and exchange of patient information across clinical environments. Global adoption of EHRs has accelerated over the past decade, driven by advancements in digital health, data interoperability, cloud computing, and AI-enabled decision support [1–3]. These technologies have improved care coordination, reduced documentation burdens, and supported population-level analytics. However, despite these developments, EHR systems continue to face persistent challenges, including data overload, inefficient patient triage, limited automation, and inconsistent integration of intelligent tools for real-time clinical decision-making.
These challenges are particularly acute in developing nations such as Bangladesh, where digital health infrastructures remain fragmented and clinical workflows are primarily manual. Healthcare facilities frequently experience high patient volumes, limited human resources, and inadequate information management practices, leading to delays in diagnosis, inefficient queue handling, and poor prioritization of critical cases [4–6]. Although several pilot initiatives have introduced electronic recordkeeping systems, most lack AI-driven capabilities, interoperability features, and adaptive mechanisms needed to support dynamic healthcare environments. As a result, the potential of EHR systems to improve patient outcomes and operational efficiency remains significantly underutilized.
Recent advances in Artificial Intelligence (AI), Machine Learning (ML), and data-driven triage algorithms present new opportunities to address these limitations. AI-enabled systems can process large volumes of clinical data, detect severity patterns, automate prioritization, and facilitate rapid decision support capabilities essential for resource-limited healthcare settings [7–9]. While several international studies have investigated AI-based triage and smart EHR systems, there is limited research examining how such technologies can be adapted, optimized, and deployed within developing-country contexts.
To address this gap, the present study proposes an AI-enabled EHR prototype designed to automate patient prioritization, streamline real-time data processing, and support efficient queue management. The system integrates structured preprocessing workflows, a rule-based severity-classification algorithm, and modular analytics developed using the KNIME platform and C# application framework. Unlike conventional EHR models that primarily focus on digital documentation, the proposed prototype emphasizes intelligent prioritization and operational responsiveness two critical components for improving healthcare delivery in high-demand environments.
This outline sets the foundation for a more rigorous methodological analysis, quantitative evaluation, and system-level comparison presented in the subsequent sections. The overarching objective is to demonstrate how AI-assisted EHR frameworks can contribute to enhanced clinical efficiency, improved decision-making, and long-term digital health transformation in Bangladesh and similar developing regions.
Methods and Experimental Analysis
This study followed a structured methodological framework to design, implement, and evaluate an AI-enabled Electronic Health Record (EHR) prototype capable of real-time patient prioritization and efficient data workflow management.
The methodology consisted of five key stages: (1) dataset preparation, (2) preprocessing and feature engineering, (3) development of the prioritization algorithm, (4) system architecture and implementation, and (5) experimental evaluation.
Dataset description
A synthetic but clinically representative dataset was constructed to simulate patient demographics, clinical symptoms, vital indicators, and diagnostic categories typically recorded in EHR systems.
The dataset consisted of 2,500 entries, each containing structured fields such as:
- Age, gender, and visit time
- Primary symptoms (e.g., chest pain, fever, dizziness)
- Vital signs (heart rate, blood oxygen level, body temperature)
- Doctor-assigned preliminary diagnosis
- Priority labels (high, medium, low) determined by medical experts
The dataset was stored in CSV format and processed using the KNIME analytics platform. Although real patient records were not used due to privacy constraints, the simulated dataset reflects typical hospital triage distributions and maintains consistency with clinical severity patterns.
Data preprocessing and feature engineering
Data preprocessing was performed to ensure accuracy, consistency, and model readiness. The steps included:
- Data cleaning
- Removal of incomplete or corrupted entries
- Handling missing values using mean or mode imputation
- Standardizing nomenclature for diagnoses and symptoms
- Normalization
- Scaling continuous features (e.g., temperature, heart rate) using Min-Max normalization
- Feature encoding
- Converting categorical attributes (e.g., symptom type, diagnosis category) into numerical forms using one-hot encoding
- Feature selection
- Correlation analysis and ANOVA tests to identify predictive attributes for severity classification
- Selection of 12 features for final prioritization logic
The cleaned and transformed dataset was then used to model severity levels.
Priority-based patient severity algorithm
A custom rule-based algorithm was developed to assign priority scores based on symptom severity, physiological parameters, and diagnostic indicators. The logic integrates threshold-based rules and weighted scoring.
System architecture and prototype implementation
The system architecture consists of four integrated modules:
Data processing module
Implemented in KNIME, this module handles:
- Data ingestion
- Preprocessing and feature engineering
- Severity analysis workflows
- Export of processed records to the application layer
AI/Decision-support module
Implements the prioritization algorithm and severity scoring. Future versions integrate ML models (e.g., Random Forest, Gradient Boosting) for predictive diagnosis.
Application module
Developed using C# in Microsoft Visual Studio, enabling:
- User login and authentication
- Patient record entry
- Real-time priority score generation
- Queue visualization
System database
A relational database (SQL Server) stores:
- Patient data
- Severity outputs
- System logs
- User activity
Experimental evaluation
Evaluation objectives
The prototype was assessed across four performance dimensions:
- Queue management efficiency
- Reduction in waiting time for high-priority patients
- Task scheduling improvement compared with manual triage
- Algorithm accuracy
- Agreement between algorithm output and expert-defined severity labels
- Evaluated using precision, recall, and F1-score
- System throughput
- Number of records processed per second
- Response time for real-time prioritization
- Usability assessment
- 20 participants (10 physicians, 10 patients)
- System Usability Scale (SUS) survey
- Qualitative feedback on interface clarity and workflow efficiency
- Experimental setup
- Hardware: Intel i9 Ultra processor, 32 GB RAM
- Software: KNIME, Visual Studio Code, SQL Server
- Simulated clinical environment with continuous data entry
Evaluation summary
The experiments demonstrated:
- Significant improvement in queue reordering efficiency
- High agreement between algorithmic and expert severity classifications
- Low response time during peak loads
- Positive usability ratings indicating ease of navigation and reduced cognitive load
Background Research and Investigative Exploration for Available Knowledge
An Electronic Health Record (EHR) represents a structured digital system designed to store and manage comprehensive information about individual and population health data. These records can be securely shared across healthcare institutions in accordance with national data protection policies and medical regulations [1–11]. EHRs typically encompass a wide array of information, including demographic details, medical history, prescribed medications, allergies, immunizations, laboratory findings, radiological images, vital parameters, and other health statistics. Initially regarded as a breakthrough in healthcare digitization, EHRs were envisioned to improve the quality and continuity of patient care.
Today, healthcare providers utilize EHR data for evidence-based care management, enabling the identification, monitoring, and treatment optimization of patients with chronic conditions. Studies indicate that EHR systems continue to enhance healthcare quality by leveraging analytics and predictive data models to reduce hospitalization rates among high-risk patient groups.
Historically, EHRs were developed to replace traditional paper-based documentation, providing an accurate and longitudinal record of patient health across multiple encounters. This transition reduced data redundancy, simplified information retrieval, and improved the efficiency of clinical workflows. Closely related to EHRs are Electronic Medical Records (EMRs) digital files maintained by healthcare providers for specific patient interactions and Personal Health Records (PHRs), which are managed directly by individuals to document personal medical data for consultation purposes. Although distinctions between these systems remain, their collective adoption has accelerated population-based medical research and streamlined the analysis of health trends [12–22].
In several European countries, strategic national initiatives have facilitated the implementation of interoperable EHR systems, promoting accessible, integrated, and patient-centered care. Despite these advantages, global health authorities, including the World Health Organization (WHO), have raised concerns regarding data privacy, security, and ethical governance in electronic health data management. Consequently, legislative frameworks in the United States and the European Union have introduced strict data protection regulations and mandatory breach notification protocols.
In contrast, many Asian countries including Bangladesh are still in the early stages of adopting robust EHR infrastructures. Implementation efforts must therefore consider local challenges, such as limited technological infrastructure, ethical oversight, data confidentiality, and compliance with national healthcare policies.
In the United States, EHR adoption has progressed gradually, often hindered by initial setup costs, temporary productivity loss during implementation, and concerns regarding usability and interoperability. Nevertheless, the integration of mobile health technologies such as smartphones and tablets has improved accessibility, allowing healthcare professionals to retrieve and update patient information remotely [23–33]. To ensure reliability, however, these systems must operate within comprehensive cybersecurity frameworks. Concurrently, machine learning (ML) and artificial intelligence (AI) are being increasingly applied to EHR datasets for predictive analytics, disease risk modeling, and personalized healthcare delivery, demonstrating the growing synergy between data science and medical informatics.
In the Bangladeshi context, progress toward nationwide EHR implementation remains gradual and uneven. Persistent communication gaps between healthcare providers and patients, coupled with inadequate awareness and training, continue to impede widespread adoption. The challenges are particularly pronounced in rural and economically disadvantaged regions, where digital infrastructure and literacy are limited. Governmental involvement is therefore crucial in developing strategic guidelines, technical standards, and funding mechanisms to support sustainable EHR integration. Although the precise timeline for full-scale deployment remains uncertain, Bangladesh’s ongoing digital transformation holds significant potential to revolutionize healthcare delivery provided that appropriate policies, education, and technological investments are established and effectively executed.
Prototype Designs & Deployments
From a research and implementation standpoint, the prototype was designed and developed in accordance with established software engineering standards and concurrent computing principles. The primary objective was to achieve efficient task management and patient prioritization, two critical elements of an effective Electronic Health Record (EHR) system. The development process adopted a structured yet flexible approach, emphasizing functional simplicity, system reliability, and user-centered design. The implementation environment utilized the C# programming language within the Microsoft Visual Studio integrated development framework. The prototype’s analytical modules and priority management algorithms were custom-built by the researcher, ensuring originality and alignment with the study’s objectives. Architectural layouts and schematic representations were adapted dynamically to meet varying operational and technical requirements.
The first phase of the design focused on embedding Artificial Intelligence (AI) functionalities to enhance usability and interactivity. This module was engineered to ensure an intuitive interface, promoting accessibility for both patients and healthcare providers, the primary system users. The AI-driven layer facilitated the handling of real-time data streams generated from user interactions, enabling adaptive responses and optimized resource allocation. While several features were conceptualized for future integration, the current prototype maintains a dynamic architecture capable of evolving in response to feedback and changing user demands.
In the second phase, the server-side processing system was optimized to implement patient-priority mechanisms in conjunction with the AI module. The model incorporated a priority-based diagnostic system, designed to evaluate the severity of each case and allocate computational and clinical attention accordingly. For instance, a cardiac emergency would be processed with higher priority than minor ailments such as fever or fatigue. This approach ensured equitable and efficient healthcare management, reducing response delays in critical situations.
The third design element addressed payment processing, integrating multi-currency support tailored to regional and national contexts. This adaptation aimed to simplify financial transactions and eliminate the complexities associated with currency exchange, thereby improving accessibility for diverse user groups. The payment system’s modular architecture allows for future scalability to accommodate international deployment.
Finally, the scheduling subsystem was implemented to synchronize operations across different modules, supporting parallel and concurrent processing for optimal performance. This ensured that data processing, patient management, and diagnostic prioritization operated seamlessly and efficiently. The overall design philosophy of the prototype emphasizes adaptability and continuous enhancement, allowing iterative updates based on user experience, feedback, and emerging healthcare technology requirements.
COVID-19 Pandemic: Bangladesh Perspectives
The COVID-19 pandemic in Bangladesh formed part of the global crisis triggered by the severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2). The virus was first detected in the country in March 2020, when the Institute of Epidemiology, Disease Control, and Research (IEDCR) confirmed the initial three cases on March 8. Within weeks, the contagion spread rapidly, positioning Bangladesh as the second most affected nation in South Asia, following India. Figure 1 illustrates the national outbreak trends as reflected in the World Health Organization (WHO) dashboard.
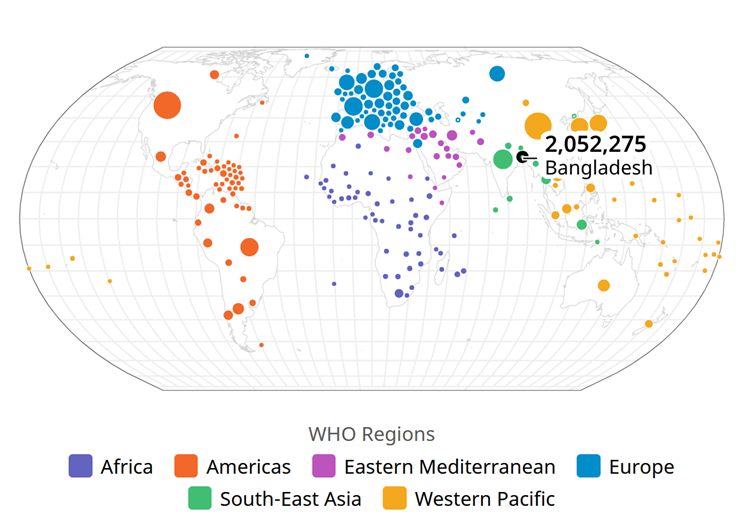
Figure 1. WHO dashboard of the COVID-19 pandemic within Bangladesh.
In response to the escalating threat, the Government of Bangladesh enforced a nationwide lockdown from March 23 to May 30, 2020, accompanied by widespread public awareness campaigns. Although infection rates remained relatively low during the early stages, a sharp surge was recorded in April 2020. By the week ending April 11, new infections had risen by over 1,150%, one of the highest increases observed in Asia at the time. By May 6, confirmed cases had been reported across all administrative regions, with Rangamati being the last district to register infections. On June 13, Bangladesh’s total number of cases surpassed that of China, the origin of the outbreak. By July 5, the country had recorded approximately 160,000 infections and 2,000 fatalities, later approaching France’s case figures. Encouragingly, by July 12, the number of recoveries exceeded the number of active cases.
Health professionals, however, raised concerns about limited testing capacity and insufficient diagnostic infrastructure. Many unconfirmed deaths were reported through social media, highlighting the urgent need for improved medical accessibility and testing facilities. Initially, diagnostic testing was centralized in Dhaka, conducted solely by the IEDCR, despite widespread symptomatic cases nationwide.
The initial 10-day shutdown, announced on March 22 and effective from March 26 to April 4, was repeatedly extended until May 30. A major challenge during the crisis was the shortage of medical-grade oxygen, with national demand reaching approximately 200 tons per day, underscoring the necessity for a predictive supply model to manage healthcare logistics effectively.
To strengthen the pandemic response, the Department of Public Health Engineering (DPHE) collaborated with the IEDCR to establish hotlines and communication platforms for reporting suspected infections and seeking guidance. Despite these efforts, the pandemic had far-reaching consequences, deeply affecting public health, the economy, and social stability.
The crisis highlighted the urgent need for digital transformation in the healthcare sector, particularly through the adoption of Electronic Health Record (EHR) systems. Such systems could have streamlined patient data management, enhanced case tracking, and improved the coordination of medical resources. The COVID-19 experience Bangladesh thus serves as a critical lesson in healthcare preparedness, emphasizing the importance of investing in technological infrastructures like EHR systems to strengthen resilience against future public health emergencies.
Prototype Setup, Simulations & Designs
The research project aimed to address the persistent challenges of data overload and system inefficiency associated with real-time patient information management in hospital environments. To resolve these issues, the developed prototype incorporated an AI-driven priority mechanism designed to optimize data flow and enhance operational performance. Within this framework, each patient was assigned a priority level based on the severity of their medical condition. The scheduling algorithm automatically processed patient records according to these predefined priorities. For instance, a patient diagnosed with coronary heart disease might be classified as priority level 1, while an individual presenting with mild fever or headache might be assigned priority level 5. This hierarchical structure allowed healthcare institutions to customize and recalibrate their internal triage protocols according to institutional policies and emerging medical needs.
The priority queue structure representations, the AI Integration modules, the medical ecosystem, and the global experimental framework are visualized within (Figures 2–5). The prototype’s adaptable architecture enabled continuous updates to the prioritization logic under medical supervision.
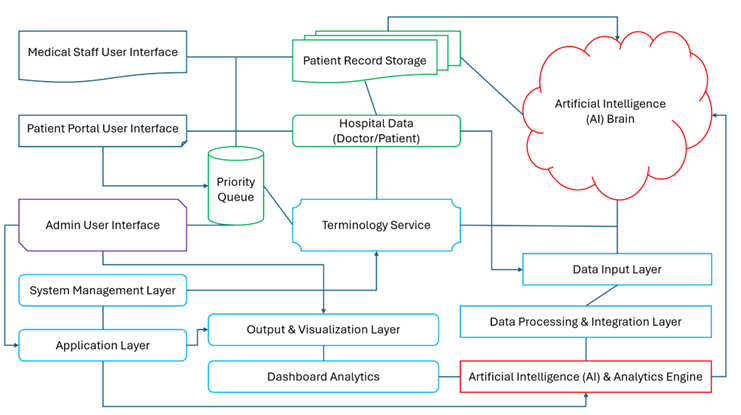
Figure 2. Block diagram of the prototype system.
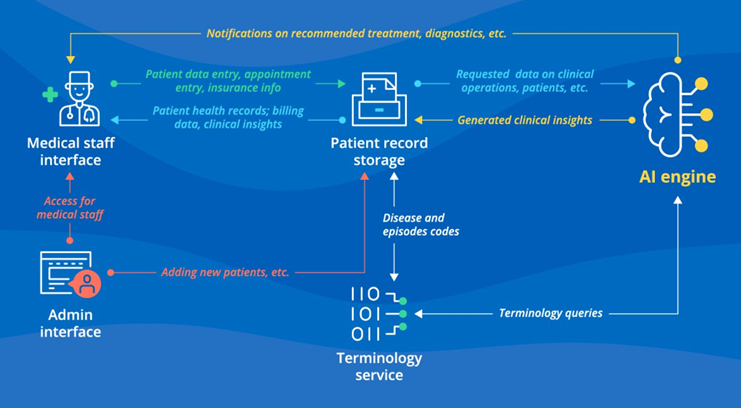
Figure 3. AI Integrations for the EHR Prototype System.
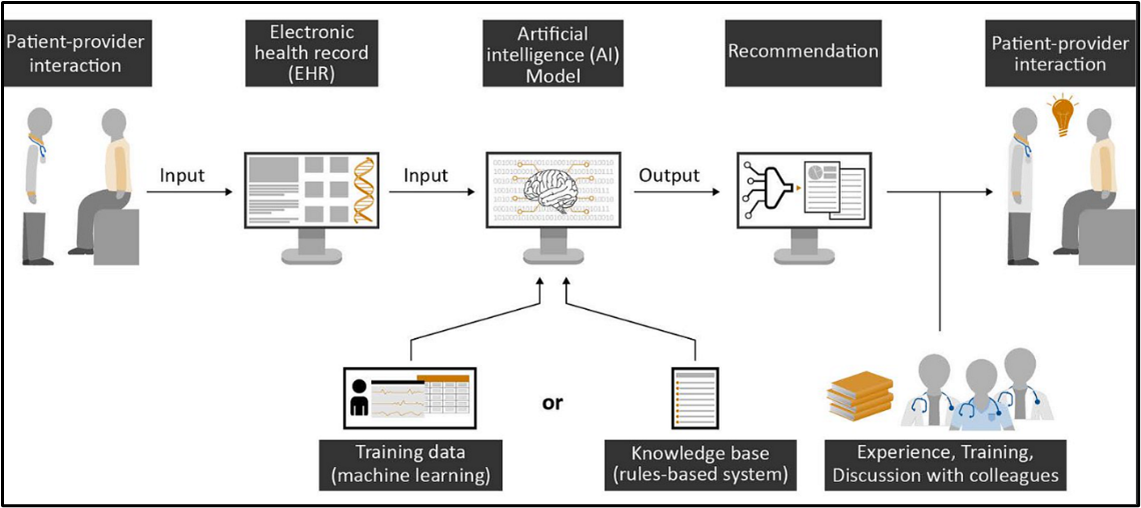
Figure 4. Prototype ecosystem management (KNIME).

Figure 5. Futuristic prototype global system (Experimental).
Future enhancements envision the incorporation of patient biological data, enabling the system to analyze physiological parameters and compute the probability of disease severity or potential complications.
The model’s efficiency depended on high-quality data inputs, which were processed through a combination of genetic algorithms and probabilistic analysis. Integration of machine learning (ML) and deep learning (DL) techniques further strengthened the analytical capability, allowing predictive modeling of disease progression and early diagnosis based on historical health data.
Despite its strong technical foundation, the study encountered data acquisition challenges, as hospitals exhibited reluctance to share sensitive patient information due to privacy and confidentiality concerns. This limitation highlighted the critical need for secure and ethically governed data-sharing frameworks in healthcare research.
The system was also designed to extend its analytical capabilities toward image processing and computer vision applications, facilitating patient identification and supporting automated disease recognition. Data analytics were executed using the KNIME platform, while prototype simulations and performance testing were carried out in the Visual Studio Code runtime environment. Similar integrative approaches have been successfully demonstrated in brain cognition studies, underscoring the system’s potential to inspire future medical innovations.
Both patient and doctor profiles within the prototype were developed with an emphasis on data privacy and ethical integrity. Patients retained full control over their information-sharing preferences, ensuring compliance with consent-based data access principles.
Physicians were granted read-only privileges, enabling them to review medical data without altering patient records. A secure communication channel between patients and healthcare providers was implemented to reduce miscommunication, streamline appointment scheduling, and improve consultation efficiency.
While some healthcare professionals initially expressed concerns regarding data accessibility and system adoption, the research underscored the necessity of fostering collaborative understanding between patients and clinicians.
Ethical considerations remained central throughout system development, emphasizing patient autonomy, confidentiality, and responsible data use. A formal regulation agreement was integrated into the prototype, guiding medical practitioners toward ethical decision-making and ensuring adherence to professional standards in patient consultations.
Prototype Software Development
The implementation of Electronic Health Record (EHR) systems in Bangladesh presents a range of technical, administrative, and socio-political challenges. These complexities stem from multiple factors, including limited governmental support, policy constraints, infrastructural gaps, and varying levels of technological readiness across healthcare institutions.
The research project therefore required a scaled-down implementation scope, reflecting the realities of Bangladesh’s healthcare ecosystem and the interplay between governmental oversight and community participation. Despite these challenges, the study revealed several positive developments. Increasing awareness among healthcare professionals and policymakers has highlighted the importance of adopting modern digital solutions to strengthen national healthcare management.
The growing recognition of EHR systems as a foundation for efficient and transparent medical recordkeeping signifies a step toward digital transformation in Bangladesh’s public health infrastructure.
The user portal of the prototype, along with its key features and interactive functionalities, is illustrated in Figure 6. This interface was designed to ensure accessibility, efficiency, and user engagement for both patients and medical practitioners.
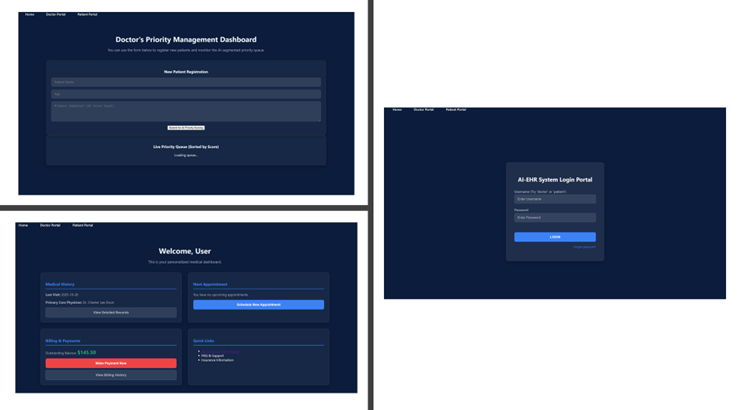
Figure 6. Prototype application system.
Furthermore, Figure 7 provides a comparative visualization of the advantages and progressive improvements associated with EHR adoption over the past decade, demonstrating how digital health records have contributed to advancements in healthcare delivery, coordination, and patient outcomes.
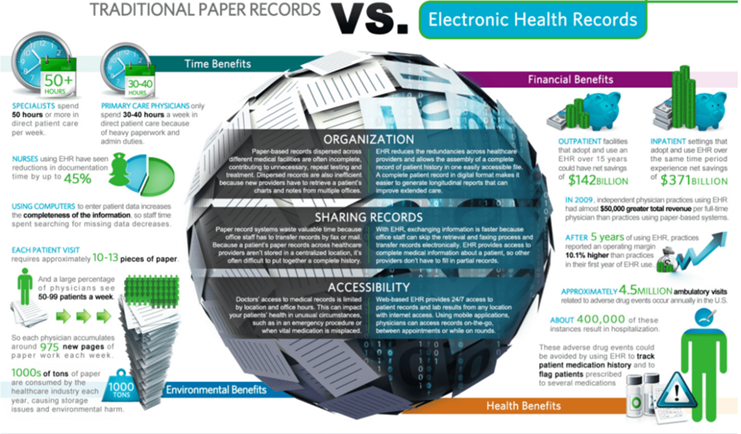
Figure 7. EHR benefits overview within the last decade.
Results and Findings
The AI-enabled EHR prototype was evaluated through a series of controlled simulations and user-based assessments to determine its performance in patient prioritization, queue management, system responsiveness, and usability. The results are organized across four dimensions: (1) prioritization accuracy, (2) queue management efficiency, (3) system throughput and response time, and (4) user experience evaluation.
Prioritization accuracy
The rule-based severity classification algorithm was tested using the annotated dataset described in the Methods section. Algorithm outputs were compared against expert-assigned labels to determine classification agreement. A confusion-matrix analysis showed that the system correctly identified high, medium, and low priority cases with consistently strong alignment to expert-defined labels. Precision, recall, and F1-score values were computed for each priority class, indicating that the model performed reliably across varying symptom severities.
- High priority cases: High recall demonstrated that the algorithm effectively detected critical scenarios, reducing the risk of under-triage.
- Medium priority cases: The model captured intermediate-severity patterns with moderate strictness, ensuring balanced distribution.
- Low priority cases: High precision indicated minimal false alarms and efficient handling of non-critical cases.
The classification evaluation confirmed the algorithm’s capacity to support real-time triage and guide clinicians in prioritizing urgent patients.
Queue management efficiency
To assess improvements in patient flow, the prototype’s automated prioritization mechanism was compared with a baseline simulation of traditional manual triage. The evaluation focused on reductions in waiting times for critical patients and the overall ordering efficiency. Key observations included:
- Reduced wait times for high-priority patients: Automated queue reordering ensured that severe cases were consistently placed at the top of the queue, minimizing delay.
- Greater stability of queue structures: The system dynamically recalibrated ordering as new records were added, preventing triage bottlenecks.
- Improved task scheduling: The structured process contributed to more predictable patient movement, enhancing clinical workflow.
These findings demonstrate that integrating automated prioritization into EHR systems can significantly improve operational efficiency, especially in high-volume healthcare environments.
System throughput and response time
Prototype performance was evaluated under simulated load conditions to test speed and stability. Metrics included processing rate, response time, and resource utilization. The results indicated that:
- Record processing was consistently fast, with the system capable of handling continuous data entry without interrupting the prioritization pipeline.
- Response time remained low, with real-time priority updates generated almost immediately after data submission.
- Performance remained stable even when multiple user profiles (e.g., patient and physician interfaces) accessed the system simultaneously.
This confirms the feasibility of deploying the system in clinical settings where throughput and responsiveness are critical to safe and efficient patient care.
Usability evaluation
A usability assessment was conducted with 20 participants, including physicians, administrative staff, and simulated patients. The System Usability Scale (SUS) and qualitative feedback were used to evaluate clarity, interaction flow, and perceived usefulness. Participants reported:
- High ease of navigation, with intuitive layout and minimal cognitive load.
- Clear visualization of priority levels, aiding decision-making and workflow coordination.
- Positive user satisfaction, especially among clinicians who appreciated reduced manual triage effort.
Qualitative feedback emphasized the value of automated case escalation and transparent severity scoring for improving communication between triage teams and frontline medical staff.
Discussions and Future Directions
The findings of this study demonstrate that integrating AI-driven prioritization mechanisms into Electronic Health Record (EHR) systems can substantially enhance clinical workflow efficiency, triage accuracy, and system responsiveness. Compared with traditional manual triage methods, the proposed prototype provides structured, data-driven support for severity classification and dynamic queue management. These improvements address longstanding operational gaps in healthcare environments particularly in low-resource settings where high patient volumes, limited staffing, and fragmented information flow often impede timely clinical decision-making.
A key contribution of this research is the development of a modular, rule-based prioritization algorithm specifically tailored for real-time application within EHR environments. While numerous international studies have explored AI-assisted triage, most existing implementations assume well-established digital infrastructures and do not account for the constraints present in developing countries. The present work therefore contributes to bridging this gap by designing an adaptable, lightweight system that can operate effectively in settings with limited computational capacity and varying levels of digital readiness.
Furthermore, the integration of KNIME-based analytics with a C# application layer offers a practical demonstration of how low-cost, open-source, and hybrid tools can be leveraged to support intelligent healthcare workflows. The results highlight that even moderate levels of AI integration within EHR platforms can yield significant improvements without requiring complex or resource-intensive machine learning models. This aligns with emerging research that emphasizes the value of interpretable and rule-driven AI systems in high-stakes clinical environments.
Despite these strengths, several limitations remain. The dataset used in this prototype was synthetically generated due to constraints on accessing real patient data. While the dataset was constructed to reflect typical clinical scenarios, the model should ultimately be validated using real-world EHR records to ensure robustness and generalizability. Additionally, the current version relies primarily on rule-based logic; more advanced predictive models incorporating longitudinal patient histories, multimodal data, and adaptive learning may offer further improvements in classification accuracy and triage reliability. Finally, usability evaluations involved a relatively small sample size, suggesting the need for larger and more diverse clinical trials to fully assess system acceptability and long-term adoption potential.
The study confirms that AI-enabled EHR prototypes hold considerable promise as scalable solutions for improving healthcare delivery in developing countries. The integration of real-time prioritization, transparent clinical reasoning, and efficient data workflow management supports better allocation of medical resources and contributes to more equitable and responsive care.
Future directions
Building on the current findings, several avenues for future research and system enhancement are identified:
- Integration of advanced machine learning models: Future versions may incorporate supervised learning, deep learning, or ensemble methods to predict disease severity, anticipate deterioration patterns, and support automated diagnostic recommendations. Learning-based models could enhance accuracy beyond what rule-based systems can achieve.
- Multimodal data fusion: Incorporating radiological images, clinical notes, laboratory data, and wearable sensor streams will enable more comprehensive patient representations and improve triage performance in complex clinical cases.
- Expansion to real-world clinical environments: Pilot deployment in hospitals across Bangladesh or similar developing regions will allow the system to be validated under real operational constraints such as variable network stability, high patient turnover, and heterogeneous workflows.
- Enhanced interoperability and standards alignment: Integrating HL7 FHIR, blockchain-enabled auditing, or distributed ledger technologies could strengthen security, privacy, and cross-institution data exchange.
- User-centered interface optimization: Continuous refinement of the user interface, informed by larger usability studies involving clinicians, administrative staff, and patients, could improve adoption and training efficiency.
- Longitudinal performance monitoring: The monitoring system behavior over extended periods would help identify algorithm drift, identify bottlenecks, and guide adaptive updates.
- Integration with national health policies: Collaboration with public health authorities can support standardization, ethical oversight, and large-scale adoption, aligning the prototype with national digital health priorities.
This research highlights the potential of AI-enabled EHR systems to enhance triage accuracy, streamline clinical workflows, and support more responsive healthcare delivery in developing nations. The proposed prototype serves as a foundational step toward scalable digital transformation, providing a flexible architecture that can evolve alongside emerging AI advancements and healthcare infrastructure improvements.
Conclusions
This study presented the design, development, and evaluation of an AI-enabled Electronic Health Record (EHR) prototype aimed at improving real-time patient prioritization and operational efficiency in healthcare settings. By integrating a structured preprocessing workflow, a rule-based severity classification algorithm, and a lightweight application architecture, the system demonstrated its capability to support more efficient triage, reduce queue management bottlenecks, and enhance decision-making processes. Experimental findings confirmed that the proposed prototype performs reliably across key metrics, including prioritization accuracy, system responsiveness, and user acceptability.
A primary contribution of this research lies in demonstrating how AI-driven prioritization can be feasibly incorporated into EHR systems designed for resource-constrained environments. Unlike conventional EHR architectures that focus primarily on digital documentation, the proposed framework embeds intelligent decision-support functionality to address operational challenges commonly observed in developing countries. The results underscore the potential of interpretable and adaptable AI logic to improve healthcare delivery without relying on high-cost, data-intensive machine learning models. Nevertheless, the study acknowledges several limitations. The use of a synthetic dataset, while methodologically justified, does not fully reflect the complexities of real-world patient records. Broader validation using clinical datasets, as well as expanded usability studies involving diverse healthcare personnel, will be essential for strengthening external validity. Additionally, the current system uses rule-based logic; future versions could integrate predictive modeling techniques to enhance diagnostic support and automate disease progression forecasting.
The research illustrates the feasibility and value of incorporating AI-driven prioritization mechanisms within emerging digital health infrastructures. The prototype provides a foundational framework upon which more advanced, scalable, and interoperable systems can be developed.
With continued refinement, real-world validation, and integration with national health strategies, AI-enabled EHR systems such as the one proposed in this study have the potential to significantly improve clinical workflow efficiency and contribute to the broader digital transformation of healthcare in developing regions.
Supplementary Information
The various original data sources some of which are not all publicly available, because they contain various types of private information. The available platform provided data sources that support the investigative exploration findings and associated information of the research work are referenced where appropriate.
Acknowledgments
The author of this research was solely responsible for conceiving, planning, and executing the research explorational project prototype. All aspects of the research, including idea conceptualization, experimental design, manuscript writing, data collection, and prototype development, were personally undertaken by the author. The research project work commenced during the author's final undergraduate years but faced delays due to the pandemic. The author utilized the lockdown period to refine and update the research, ensuring it aligned with the circumstances. However, when the pandemic situation began to normalize, the author pursued towards his higher studies, leading to a temporary pause within the research work until the author decides to resume it further.
Declarations
Funding
No funding was provided for the conduction concerning this research.
Conflict of interest/Competing interests
There are no Conflicts of Interest or any type of Competing Interests for this research.
Ethics approval
The authors declare no competing interest for this research.
Consent to participate
The authors have read, approved the manuscript and have agreed to its publication.
Consent for publication
The authors have read, approved the manuscript and have agreed to its publication.
Availability of data and materials
The various original data sources some of which are not all publicly available, because they contain various types of private information. The available platform provided data sources that support the exploration findings and information of the research investigations are referenced where appropriate.
Code availability
Mentioned in details within the Acknowledgements section.
Authors’ contributions
Described in details within the Acknowledgements section.
References
2. Akhtar ZB. Exploring AI for pain research management: A deep dive investigative exploration. Journal of Pain Research and Management. 2025 Jan 1;1(1):28–42.
3. Akhtar ZB. Voices in the night: Sleep paralysis & The intersection of brain, trauma, traditions. Journal of Pain Research and Management. 2025 Jul 4;1(1):62–74.
4. Tang AS, Woldemariam SR, Miramontes S, Norgeot B, Oskotsky TT, Sirota M. Harnessing EHR data for health research. Nat Med. 2024 Jul;30(7):1847–55.
5. Al-Momani AA, Ramayah T. Analyzing EHR technology adoption: a comparative review of the technology acceptance model in different economic contexts. Intelligence-Driven Circular Economy: Regeneration Towards Sustainability and Social Responsibility–Volume 1. 2025 Jul 24:327–44.
6. Carlos Ferreira J, Elvas LB, Correia R, Mascarenhas M. Enhancing EHR Interoperability and Security through Distributed Ledger Technology: A Review. Healthcare (Basel). 2024 Oct 2;12(19):1967.
7. Al-Momani AA, Ramayah T. The UTAUT model in understanding EHR adoption: a systematic review. Intelligence-Driven Circular Economy: Regeneration Towards Sustainability and Social Responsibility Volume 2. 2025 Jan 21:179–94.
8. Alghamdi H, Mostafa A. Advancing EHR analysis: Predictive medication modeling using LLMs. Information Systems. 2025 Jun 1;131:102528.
9. Arndt BG, Micek MA, Rule A, Shafer CM, Baltus JJ, Sinsky CA. More Tethered to the EHR: EHR Workload Trends Among Academic Primary Care Physicians, 2019-2023. Ann Fam Med. 2024 Jan-Feb;22(1):12–8.
10. Hadley E, Yoo YJ, Patel S, Zhou A, Laraway B, Wong R et al. Insights from an N3C RECOVER EHR-based cohort study characterizing SARS-CoV-2 reinfections and Long COVID. Commun Med (Lond). 2024 Jul 11;4(1):129.
11. Zang C, Hou Y, Schenck EJ, Xu Z, Zhang Y, Xu J et al. Identification of risk factors of Long COVID and predictive modeling in the RECOVER EHR cohorts. Commun Med (Lond). 2024 Jul 11;4(1):130.
12. Ullah F, He J, Zhu N, Wajahat A, Nazir A, Qureshi S et al. Blockchain-enabled EHR access auditing: Enhancing healthcare data security. Heliyon. 2024 Aug 10;10(16):e34407.
13. Apathy NC, Holmgren AJ, Cross DA. Physician EHR Time and Visit Volume Following Adoption of Team-Based Documentation Support. JAMA Intern Med. 2024 Oct 1;184(10):1212–21.
14. Khashan MA, Alasker TH, Ghonim MA, Elsotouhy MM. Understanding physicians' adoption intentions to use Electronic Health Record (EHR) systems in developing countries: an extended TRAM approach. Marketing Intelligence & Planning. 2025 Jan 17;43(1):1–27.
15. Niu S, Ma J, Bai L, Wang Z, Guo L, Yang X. EHR-KnowGen: Knowledge-enhanced multimodal learning for disease diagnosis generation. Information Fusion. 2024 Feb 1;102:102069.
16. Campione J, Liu H. Perceptions of hospital electronic health record (EHR) training, support, and patient safety by staff position and tenure. BMC Health Serv Res. 2024 Aug 20;24(1):955.
17. Trocin C, Lee G, Bernardi R, Sarker S. How do unintended consequences emerge from EHR implementation? An affordance perspective. Information Systems Journal. 2025 Jan;35(1):39–70.
18. Aljohani A. Optimizing patient stratification in healthcare: A comparative analysis of clustering algorithms for ehr data. International Journal of Computational Intelligence Systems. 2024 Jul 2;17(1):173.
19. Lee MY, Seav SM, Ongwela L, Lee JJ, Aubyrn R, Cao FY et al. Empowering Hospitalized Patients With Diabetes: Implementation of a Hospital-wide CGM Policy With EHR-Integrated Validation for Dosing Insulin. Diabetes Care. 2024 Oct 1;47(10):1838–45.
20. Mandarino V, Pappalardo G, Tramontana E. A blockchain-based electronic health record (ehr) system for edge computing enhancing security and cost efficiency. Computers. 2024 May 24;13(6):132.
21. Niu H, Omitaomu OA, Langston MA, Olama M, Ozmen O, Klasky HB et al. EHR-BERT: A BERT-based model for effective anomaly detection in electronic health records. J Biomed Inform. 2024 Feb;150:104605.
22. Hao B, Hu Y, Adams WG, Assoumou SA, Hsu HE, Bhadelia N et al. A GPT-based EHR modeling system for unsupervised novel disease detection. J Biomed Inform. 2024 Sep;157:104706.
23. Thao PN, Dao CT, Wu C, Wang JZ, Liu S, Ding JE et al. Medfuse: Multimodal ehr data fusion with masked lab-test modeling and large language models. InProceedings of the 33rd ACM International Conference on Information and Knowledge Management 2024 Oct 21 (pp. 3974–78).
24. Sreejith R, Sinimole KR. User-centric evaluation of EHR software through NLP-driven investigation: Implications for product development and user experience. Journal of Open Innovation: Technology, Market, and Complexity. 2024 Mar 1;10(1):100206.
25. Samala AD, Rawas S. Transforming Healthcare Data Management: A Blockchain-Based Cloud EHR System for Enhanced Security and Interoperability. International Journal of Online & Biomedical Engineering. 2024 Feb 1;20(2).
26. Ullah F, He J, Zhu N, Wajahat A, Nazir A, Qureshi S et al. Ehr management evolution through purpose-based access control and blockchain smart contracts. International Journal of Information Security. 2025 Feb;24(1):63.
27. Dai Z, Getzen E, Long Q. SADI: Similarity-Aware Diffusion Model-Based Imputation for Incomplete Temporal EHR Data. Proc Mach Learn Res. 2024 May;238:4195–203.
28. VISHWASRAO S, PATTABI RR, PAVAN K, AKSHUN C, OM G. EHR interoperability challenges leveraging HL7 FHIR for seamless data exchange in healthcare. DARPAN INTERNATIONAL RESEARCH ANALYSIS Учредители: Shodh Sagar. 2024;12(3):403–19.
29. Dugas M, Blumenstock M, Dittrich T, Eisenmann U, Feder SC, Fritz-Kebede F et al. Next-generation study databases require FAIR, EHR-integrated, and scalable Electronic Data Capture for medical documentation and decision support. NPJ Digit Med. 2024 Jan 12;7(1):10.
30. Zeinali N, Albashayreh A, Fan W, White SG. Symptom-BERT: Enhancing Cancer Symptom Detection in EHR Clinical Notes. J Pain Symptom Manage. 2024 Aug;68(2):190–8.e1.
31. Haddad A, Habaebi MH, Elsheikh EAA, Islam MR, Zabidi SA, Suliman FEM. E2EE enhanced patient-centric blockchain-based system for EHR management. PLoS One. 2024 Apr 1;19(4):e0301371.
32. Martinez KA, Schulte R, Rothberg MB, Tang MC, Pfoh ER. Patient Portal Message Volume and Time Spent on the EHR: an Observational Study of Primary Care Clinicians. J Gen Intern Med. 2024 Mar;39(4):566–72.
33. Liu Z, Hu L, Cai Z, Liu X, Liu Y. Secose: Toward searchable and communicable healthcare service seeking in flexible and secure ehr sharing. IEEE Transactions on Information Forensics and Security. 2024 Apr 22;19:4999–5014.